










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.15 n.41 Murcia Jan. 2016
ADMINISTRACIÓN - GESTIÓN - CALIDAD
Safety culture: The perception of intensivist nurses
Cultura de segurança: a percepção dos profissionais de enfermagem intensivistas
Cultura de seguridad: la percepción de los profesionales de enfermería intensivista
Schwonke, Camila Rose Guadalupe Barcelos*; Filho, Wilson Danilo Lunardi**; Lunardi, Guilherme Lerch***; da Silveira, Rosemary Silva****; Rodrigues, Maria Cristina Soares***** and Guerreiro, Márcio Osório******
*PhD in nursing at the Postgraduate nursing Program/University of Rio Grande (PPGEnf/FURG). Nurse coordinator of Research at the hospital of the Federal University of Pelotas, Brazil. Member of the Study and Research Group on Labor of Nursing and Health Organization - GEPOTES. Rio Grande, Rio Grande do Sul. E-mail: camila.schwonke@gmail.com
**PhD in nursing. Professor at PPGEnf/FURG. Leader of GEPOTES.
***Business administrator. PhD in administration. Professor PPGEnf/FURG.
****Nurse, PhD in nursing. Professor at PPGEnf- FURG.
*****Nurse. Phd in Health Sciences. Professor at Postgraduate nursing Program - University of Brasília
******Md. PhD in Health Sciences. Coordinator at the UCI of the University Hospital São Francisco de Paula. Professor at Federal University of Pelotas, Brazil.
ABSTRACT
This is a study which has as an objective to characterize the safety culture of the hospital institutions in the perception of the nursing professionals in intensive care. To this end, the tool of perception of the safety culture proposed by singer et al (2003) was adapted to the Brazilian context.
The sample is formed of 173 nursing professionals, acting in seven different intensive care units in Rio Grande do Sul State. After the tool validation, four constructs were proposed containing different attitudes regarding the patient safety: promoting patient safety in organizational level, patient care safety, error prevention as an organizational priority and risk and organization errors perception.
The results show the necessity of better management from the health services concerning patient safety.
Key words: Patient Safety; Intensive Care Units; Nursing; Validation Studies.
RESUMO
Trata-se de um estudo que teve por objetivo caracterizar a cultura de segurança de instituições hospitalares, na percepção dos profissionais de enfermagem intensivistas. Para tal, adaptou-se o instrumento de percepção de cultura de segurança, proposto por Singer et al. (2003), para o contexto brasileiro.
A amostra constituiu-se de 173 profissionais de enfermagem, atuantes em sete unidades de terapia intensiva, localizadas no Rio Grande do Sul. A partir da validação do instrumento, foram propostos quatro construtos, contendo diferentes atitudes, em relação à segurança do paciente: promoção da segurança do paciente em nível organizacional; segurança no cuidado ao paciente; prevenção de erros como prioridade organizacional; e percepção de riscos e erros que ocorrem na organização.
Os resultados apontam para a necessidade de melhor condução, por parte dos serviços de saúde, das questões que envolvem a segurança do paciente.
Palavras chave: Segurança do Paciente; Unidades de Terapia Intensiva; Enfermagem; Estudos de Validação.
RESUMEN
Se trata de un estudio que tuvo por objetivo caracterizar la cultura de seguridad de las instituciones hospitalarias, en la percepción de los profesionales de enfermería intensivista. Para ello, se adaptó el instrumento de percepción de cultura de seguridad, propuesto por Singer et al (2003), para el contexto brasileño.
La muestra se constituyó de 173 profesionales de enfermería, trabajadores en siete unidades de terapia intensiva localizadas en Río Grande del Sur. A partir de la validación del instrumento, fueron propuestos cuatro construtos conteniendo diferentes actitudes en relación a la seguridad del paciente: promoción de la seguridad del paciente a nivel organizacional, seguridad en el cuidado al paciente, prevención de errores como prioridad organizacional y percepción de riesgos y errores que ocurren en la organización.
Los resultados apuntan la necesidad de conducir mejor por parte de los servicios de salud las cuestiones que involucran la seguridad del paciente.
Palabras clave: Seguridad del Paciente; Unidades de Cuidados Intensivos; Enfermería; Estudios de Validación.
Introduction
Technological advances related to prevention, diagnosis and diseases treatment, developed by the health sector, has been significant in recent years. Health professionals, since its formation process are concerned and undertake with the assistance provided, aiming at a quality care. However, despite efforts to upgrade the education of professionals and in providing assistance using all available technology, the patient may be placed in situations of risk and damage. Since the 70s, medical record reviews studies showed high rates of adverse events (AE) related to the care provided during hospitalization(1).
However, in the current context of studies on human error, was from the work To err is human: building a safer health care system, published in 2000 by the Institute of Medicine (IOM) that issues related to patient safety are highlighted. This study describes that during the health care, mistakes happen and are frequent, promoting thousands of deaths and irreversible consequences, being identified in that country, as the eighth cause of death, surpassing those caused by car accidents, breast cancer and immunodeficiency syndrome acquired (AIDS), despite the large investments made in this area. It is estimated by the data in this publication that every day 100 hospitalized Americans die for damages related to errors and not the disease(2). Still, WHO data show that thousands of patients worldwide suffer some kind of error related to health care, and some of these errors can result in injuries and deaths of patients, estimated that out of 10 patients, one is the victim of errors during assistance(3).
Recently in Brazil, the 2013 decree # 529 of the Ministry of Health established the National Patient Safety Program (NPSP)4 which has the overall objective to contribute to the qualification of health care in all health services in the country. This decree provides a conceptualization and strategies that need to be implemented around the Safety Culture establishment which constitutes a key element for the success of the actions surrounding the Patient Safety(4).
From a conceptual perspective, the NPSP establishes that Safety Culture sets up from five characteristics operationalized by the organization's security management, they are: a- culture in which all employees, both healthcare and managers, take responsibility for their own safety, the safety of their colleagues, patients and families; b- culture that prioritizes safety above financial and operational goals; c- culture that encourages and rewards the identification, reporting and resolution of security issues; d- culture that, from the occurrence of incidents, promotes organizational learning; e- culture that provides resources, structure and responsibility for effective safety maintenance. The strategies established by PMSP range from the production of manuals, training of health teams, evaluation of indicator targets services to the promotion of safety culture, focusing on learning and organizational improvement, engagement professional and patients in preventing incidents with emphasis on safety systems, avoiding the individual responsibility processes(4).
Given this context, the aim of this study was to characterize the safety culture of the hospitals in the perception of intensive care nurses. The choice of the intensive care environment is because of the peculiarity of these units that, due to the patient's severity, requires quick action, effective and risk-free.
For this to occur is required, the performance of prepared teams for this purpose, set in an organizational context that prioritizes patient safety.
Methods
This study is a quantitative and exploratory research with descriptive design, carried out with 173 nursing professionals working in Intensive Care Units (ICUs) of seven hospitals in three cities of Southern Brazil. To compose the study population, were adopted as inclusion criteria: be professional nurses registered with the Regional Council of State Nursing of Rio Grande do Sul (COREn/RS), have employed by one of the institutions where the study was conducted, agree to participate and perform direct patient care activities.
The terms contained in the National Health Council Resolution 196/96 were respected - CONEP/MS on Research Involving Human Subjects, and the research project was submitted to the Ethics Committee in Research in the Area of Health of the Federal University of Rio Grande - CEPAS/FURG, having obtained a favorable opinion for its implementation (Opinion 152/2011).
Preparation and Instrument Validation
The research instrument proposed for data collection features 13 of the sample characterization questions and 30 closed - operationalized on a Likert scale, containing 5 reset intervals, ranging from strongly disagree to agree, adapted from the study(5), representing situations involving different aspects related to safety culture in hospitals where their agreement, point to an increased perception of safety culture. From the original questions, 11 were reversed, that is, situations that, if were listed in their agreement, would point to a lower perception by the informant about the safety culture in this institution. This required recoding of these issues for interpretation, reversing the obtained scores when grouping to the other questions.
The questionnaire was submitted to a validation process, which took place in four stages(6-7):
a) Back translation: where the original questions were translated from English into Portuguese by two professional Bachelor of Arts with specialization in English language and retranslated from Portuguese to English by two other professionals with the same training, and comparing subsequently between the two versions to assess the possible differences(6);
b) Face validity: it was verified that the questions translated present form and vocabulary for the purpose of measurement, performing the application and questionnaire discussion with three researchers in the field (in this step were suggested some adjustments expressions and words in order to make it understandable to the local reality what was being questioned);
c) Content Validity: it was checked through a pre-test with 31 nurses graduate students from a Specialization Course in Intensive Care Nursing at a private college of Rio Grande do Sul, if the questionnaire items represented the content that was intended to be analyzed;
d) Dimension validity: where we attempted after the questionnaire, to define the dimensions characteristics interested for the research, testing the internal consistency of each item (ie, the scale reliability) and convergent and divergent validity of the instrument. It should be noted that this step of the validation process involved two statistical tests: a factor analysis and Cronbach's alpha.
Factor analysis is a method which seeks to identify related items on a scale. The procedure is used to identify and group the different measures of some underlying attribute and to distinguish them from different measures attribute(7). This analysis grouped questions concerning the perception of nursing professionals about the existing safety culture in hospitals where they work in four dimensions (constructs) and suggested the elimination of 13 of the 30 questions of the questionnaire for these presented low correlations in their blocks or did not adhere to conceptually formed dimensions.
The four proposed dimensions explain 54.8% of the variance of the original issues, which is a moderate degree of synthesizing the data. Table 1 shows the factor scores for each dimension, according to its formation on factors, which correspond to the four dimensions discussed in the results.
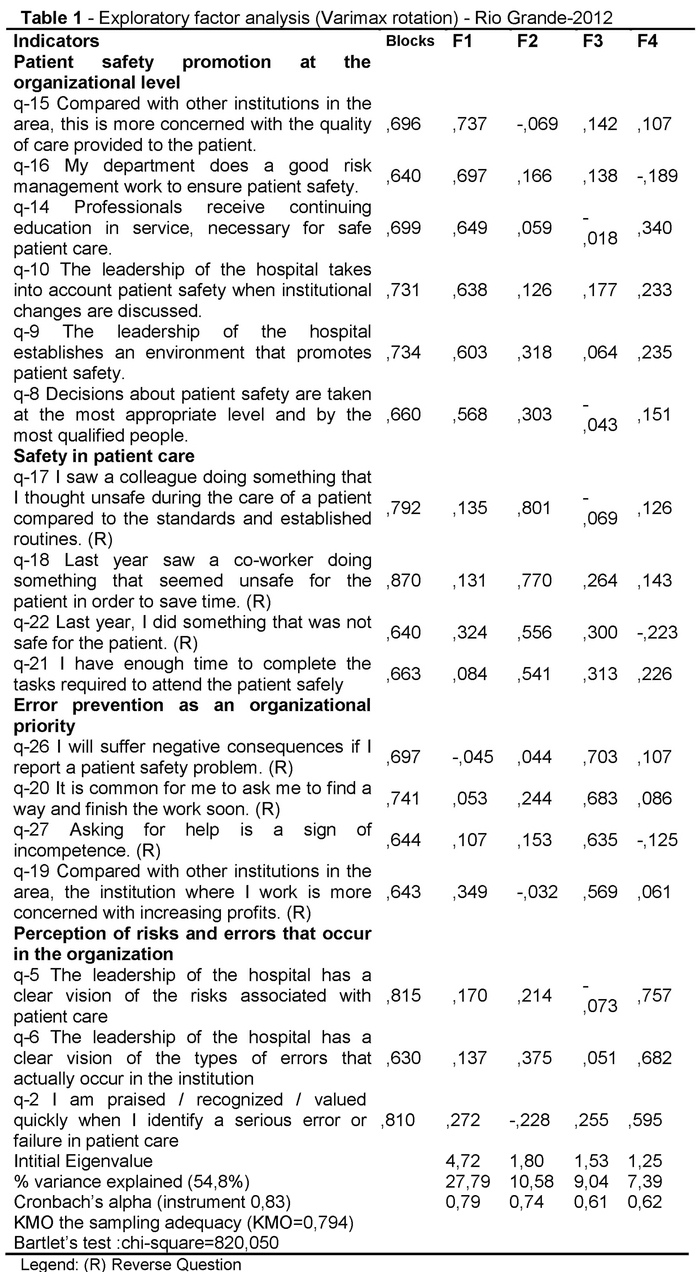
The reliability of the dimensions was tested by Cronbach's alpha calculation(8). Values for this test range from 0 to 1 and the higher the reliability coefficient, the more accurate (internally consistent) are the measure(7). The instrument presented Cronbach's alpha value 0.83, while the size of the coefficients were between 0.61 and 0.79. It is noted that for exploratory studies, the suggested values are between 0.60 and 0.80, which indicates the reliability of the instrument(9).
Based on the above considerations, the four dimensions proposed were conceptually defined as: patient safety promotion at the organizational level, regarding the expectations and actions of managers to promote patient safety(5); safety in patient care, which refers to the non-occurrence of forgetfulness, carelessness, mistakes, lapses and violations of procedures committed in patient care(10-11); preventing errors as organizational priority, regarding the recovery of the patient safety as the first priority, even at the expense of production or efficiency(5); and perception of risks and errors that occur in the organization, which refers to the presence of a systemic view of prevention and analysis of errors in health care(12).
For data analysis, we used the Statistical Package for Social Sciences software SPSS, version 13.0. In addition to the validation tests, were carried out a descriptive analysis, mean and standard deviation and using the t-test and analysis of variance, in order to identify possible differences in perception between subgroups.
Results
The study sample was composed of 173 (80%) respondents from a universe of 216 (100%) nursing professionals working in the seven studied ICUs. Other professionals did not participate in study, because they were on holiday, on sick or maternity leave or did not accept to participate. Among the professionals who participated in the study, 17.9% were nurses, 64.8% nursing technicians and 17.3% of nursing assistants. In terms of gender, there was a predominance of females (85.5%). The age ranged between 21 and 60 years, and the highest prevalence were between 31 and 40 years, with 41%. The graduate time varied between 2 months and 39 years, with 56.6% of respondents had been working between 2 and 10 years after graduation and 77.5% came from private educational institutions. Regarding the time of work in intensive care, this was between 1 month to 29 years, with the majority of professionals (56%) worked between 2 and 10 years in this area. Regarding the type of institution, 49.1% of them work in teaching hospital, while 50.1% work in charity hospital.
The descriptive analysis of the data allowed to identify the perception of nursing professionals about the safety culture of attitudes present in their institutions. Each of the four dimensions identified in the research was operationalized through a numeric value that represents the arithmetic mean of the issues that composed individually -previously grouped in the factor analysis - reversing the reverse-scored questions. The mean of the dimensions and the respective indicators are in Table 2.
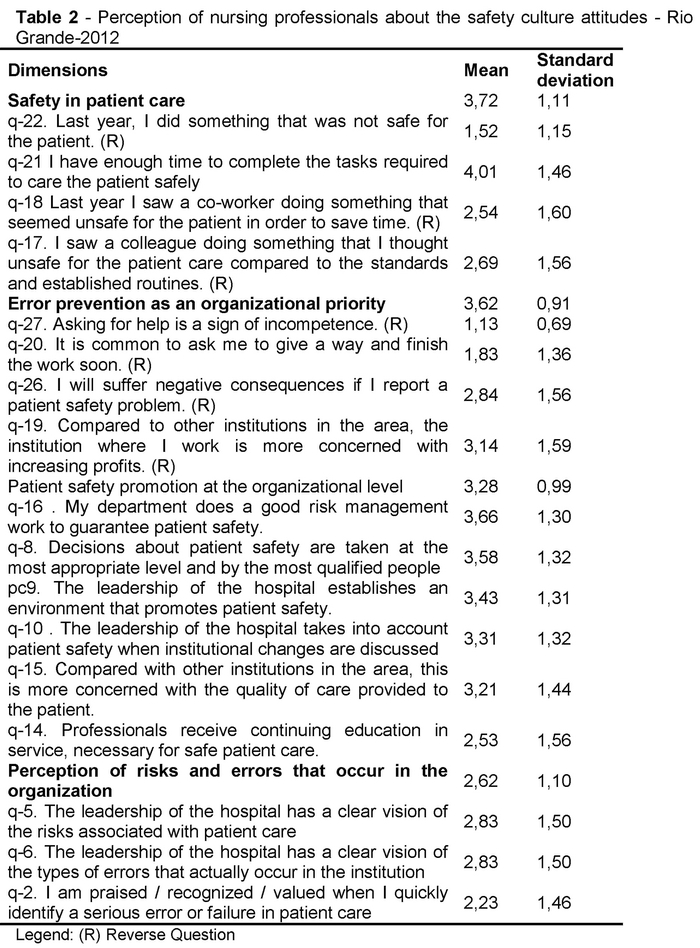
Mean perceptions of nursing professionals investigated about the attitudes around the safety culture in the institutions they work, ranged from 3.72 to 2.62, being the safety in patient care dimension, the one with the highest average (3.72), with emphasis on the issues "in the last year, I did something that was not safe for the patient" (1.52), "last year I saw a co-worker doing something that seemed unsafe for the patient, in order to save time "(2.54) and" I saw a colleague doing something that I thought unsafe for the care of a patient compared to the established rules and routines "(2.69), in which most professionals did not agree with what was being asked.
From the perception of the informants of this study, is possible to find lower means on the statements "I am praised / recognized / valued when quickly identify an error or serious error in patient care" which presented one of the lowest means (2.23). That is, most of the respondents disagreed or partially doubted that this was an attitude that occurs at the institution they work. Regarding the possibility of punishment, expressed in question 26, "I will suffer negative consequences if I report a security problem of the patient" (2.84), most professionals partially disagreed or doubted, can be inferred that this attitude may be a practice that occurs the analyzed institutions, as the perception of the professionals interviewed.
Still, the perception of the investigated professionals, constructs promotion of safety culture at the organizational level and perception of risks and errors that occur in the organization, both addressing the involvement and role of management bodies in safety culture were those who received the smallest means the descriptive analysis (3.28 and 2.62, respectively). Highlights in this direction, the questions: "professionals receive continuing education in service, necessary for safe patient care" (2.53), "the leadership of the hospital have a clear view of the risks associated with patient care" (2.83) and "the leadership of the hospital has a clear vision of the types of errors that actually occur in the institution" (2.23).
Discussion
The high means in dimensions related to patient care, by the individual or his co-workers, may suggest a difficulty of the professional in its self-assess and evaluate the attitudes of their peers that are not safe for the patient and can be related to the non-acceptance of human error, because of fear punishment and penalties(13). In this sense, to understand how mistakes happen and how can compromise patient safety, it is necessary to view them from two approaches: one centered on the person and another on the system, called systems approach. The first understands the unsafe acts as arising mainly from aberrant mental processes such that: forgetfulness, inattention, poor motivation, carelessness, negligence and recklessness. Thus, error prevention measures will drive up especially to reduce the undesirable variability of human behavior and includes disciplinary actions, censure and humiliation as a treatment. Followers of this approach tend to treat mistakes as moral issues, assuming that bad things happen to bad people(11).
In contrast to person-centered approach, the one that focuses on the system, has as basic premise that human beings are fallible and errors are expected, even in the best organizations. Mistakes are viewed as the consequence and not as the cause, having its origins not in the perversity of human nature, but on systemic factors. It is believed that although it is not possible to change the human condition, you can modify the conditions under which humans work(11).
Given the above, it is considered that the error verification and its prompt reporting are fundamental to the implementation of interventions in order to restore as soon as possible the conditions of the patient, minimizing or eliminating the losses caused14. Specifically in the ICU, according to the severity and instability presented by critical patients, the communication of a mistake can be crucial for the most satisfactory clinical outcome. Rules, regulations, sanctions and rewards can influence the definition / creation of a safety culture. Be rewarding for reporting a patient security problem increases the possibilities the professionals to do it sometimes, whereas being punished, reduces this possibility(15). In this perspective, a Brazilian study that aimed to characterize an ICU adverse event registration system, verifying its frequency and the existence of punishments, according to the perceptions of 70 nurses, showed that the majority (71.4%) perceived the existence of underreporting adverse events, and when asked about the presence of punishments at their place of work, the majority (74.3%) reported that it is "sometimes" and "always", with a predominance of verbal warning (49%) and writing (33%). However, 74.3% of nurses surveyed reported feeling safe, very safe and completely safe, against 21.4% who expressed little or no security for reporting adverse events. The results of this research allowed the authors to conclude that the punitive culture is present also in the ICU, contrary to the worldwide movement, focused on the need for adverse event reporting as a strategy to prevent its occurrence(16) in order to learn from mistakes and improve the management of safety culture in organizations.
In this conception, the data of this study suggest a more critical understanding of workers on management and organizational issues, given that the dimensions related to these issues received the lowest means in the descriptive analysis. Thus, it appears that the perception of respondents, organizations lack a clear understanding of the risks and errors to which patients are subjected, as well as investments in lifelong learning, necessary for the training of professionals are not effective.
Thus, it is necessary for the safety culture development that all participants of a system (in this case the hospital) understand the factors that determine patient safety as a whole. The organization shall maintain a state of vigilance for potential problems by acting in a timely manner to resolve them before an accident that could be avoided, takes place(10,17), preventing possible injury to patients.
The lack of ongoing support of the administration of health services has been identified in studies as a threat to patient safety(18-19). In this context, other actions need to be implemented to guarantee an approach with an adequate safety culture, and to list the promotion of internal reporting and discussion of the errors that can occur in the institution; the patient safety approach as a team and not as an individual problem; consistent allocation of human resources, paying attention to the working patterns can be submitted; the promotion of shared responsibility and coordination between units and services; and the proof of proactive attitudes on the part of management, with respect to patient safety(18-19).
Still, it is pertinent to consider that the continuing education of professionals, especially those involved in care is important, in view that the human factor is one of the most relevant for the appearance of iatrogenic occurrences / adverse events during the care, the professional knowledge may be incurred in significant barriers, able to interrupt a trajectory of opportunities triggering a serious failure in care.
Final Considerations
The results obtained in this study indicate that attitudes about safety culture, as perceived by respondents, can be viewed from the perspective of four dimensions: patient safety promotion at the organizational level; safety in patient care; error prevention as an organizational priority; and perception of risks and errors that occur in the organization.
In the perception of the studied professionals, the dimensions that discuss managerial and organizational issues had lower means scores than those who listed individual attitudes and peers, suggesting perhaps a difficulty to admit the possibility of error, for fear to further sanctions and punishments, which could compromise the strategies involving the implementation and consolidation of a safety culture. It also highlights the need for greater articulation of the organization involving issues about the recognition of risks and errors that occur in the institution, as well as the implementation of continuing education programs that promote the professionals updating and training.
Urges the need that issues involving patient safety be further elaborated by health services. Safety culture cannot be an external element to the individual, only a standard or routine that needs to adapt, but something that builds in everyday life, along with administrative provisions, at different levels of the organization. It represents the transition from a culture of silence, of punishment, which focuses on the individual and their failures to a culture of change that seeks to make the system safer. The study presents as a limitation the fact that it was carried out exclusively with nursing professionals who work in the ICU and has not been extended to other categories active in different sectors of the hospital, which could create comparisons about the safety culture of perception among managers and professionals involved in patient care. Moreover, our findings deserve attention about its generalizability, especially because the study was developed in a regional context, limited to only seven ICUs located in three municipalities in Southern Brazil.
For nursing and other areas that have an interest in the safety patient topic, this study has important contributions regarding the validation of an instrument for the Brazilian context that can assess the current safety culture in healthcare institutions.
Received: October 2, 2014
Accepted: October 31, 2014
References
1. Pedreira LC, Brandão AS, Reis AM. Evento adverso em idoso na Unidade de Terapia Intensiva. Rev Bras Enf. 2013; 66(3): 429-36. [ Links ]
2. Kohn LT, Corrigan JM, Donaldson MS. To err is human: building a safer health system. Washington: National Academy of Sciences, 2000. [ Links ]
3. World Health Organization. Patient Safety: A world alliance for safer health care. 2009. Disponível em: <http://www.who.int/patientsafety>. Acesso em: 5 fev. 2013. [ Links ]
4. Brasil. Ministério da Saúde. Portaria No529, de 1o de abril de 2013. Institui o Programa Nacional de Segurança do Paciente. Brasília, 2013. [ Links ]
5. Singer SJ, Gaba DM, Geppert JJ, Sinaiko AD, Howard SK, Park KC. The Culture of safety: results of an organization-wide survey in 15 California Hospital. Qual Saf Health Care (internet). 2003 (acesso 2 jan 2012); 12: 112-8. Disponível em: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1743680/pdf/v012p00112.pdf. [ Links ]
6. Ishman M. Measuring information sucess at the individual level im cross-cultural environments. Information Resources Management Journal. 1996; 9(4): 16-28. [ Links ]
7. Polit DF, Beck CT, Hungle BP. Fundamentos de pesquisa em enfermagem. Métodos, avaliação e utilização. 5 ed. Porto Alegre (RS): Artmed; 2004. [ Links ]
8. Gaya A. (col). Ciências do movimento humano: introdução à metodologia da pesquisa. Porto Alegre (RS): Artmed; 2008. [ Links ]
9. Hair JF. Multivariate data analysis. New Jersey (US): Prentice-Hall; 1995. [ Links ]
10. Reason J. Managing the Risks of Organizational Accidents. Aldershot (UK): Ashgate; 1997. [ Links ]
11. Reason J. Human Error: model and management. West J Med (internet). 2000 jun (acesso 10 dez 2011); 172(6): 393-6. Disponível em: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1070929/pdf/wjm17200393.pdf. [ Links ]
12. Harada MJCS. A prevenção do erro humano. In: Harada MJCS, Pedreira MLG, Pertelini MAS, et al. O erro humano e a segurança do paciente. São Paulo (SP): Atheneu; 2006. p. 27-42. [ Links ]
13. Ques AAM, Montoro CH, Gonzales, MG. Strengths and Threats Regarding the Patient's Safety: Nursing Professionals' Opinion. Rev Latino-Am Enfermagem (internet). 2010 mai-jun (acesso 18 abr 2012); 18(3): (08 telas). Disponível em: http://www.scielo.br/pdf/rlae/v18n3/pt_07.pdf. [ Links ]
14. Coli RCP, Anjos MF, Pereira LL. The Attitudes of Nurses from an Intensive Care Unit in the Face of Errors: an Approach in Light of Bioethics. Rev Latino-Am Enfermagem (internet). 2010 mai-jun (acesso 18 abr 2012); 18(3): (07 telas). Disponível em: http://www.scielo.br/pdf/rlae/v18n3/pt_05.pdf. [ Links ]
15. Vicent C. Segurança do Paciente: Orientações para evitar eventos adversos. São Caetano do Sul (SP): Yendis; 2009. [ Links ]
16. Claro CM, Krocockz DVC, Toffolleto MC , Padilha KG. Eventos adversos em Unidade de Terapia Intensiva: percepção dos enfermeiros sobre a cultura não punitiva. Rev Esc Enferm USP. 2011; 45(1): 167-72. [ Links ]
17. Dain S. Normal Accidents: Human Error and Medical Equipment Design. Heart Surg Forum. 2002; 5(3): 254-7. [ Links ]
18. Saturno PJ, Da Silva Gama ZA, Oliveira-Sousa SL, Fonseca YA, De Souza-Oliveira AC, Grupo Proyecto ISEP. Análisis de la cultura sobre seguridad del paciente en los hospitales del Sistema Nacional de Salud español. Med Clin (Barc). 2008; 131(Supl 3): 18-25. [ Links ]
19. Ministerio de Sanidad y Política Social (Espanha). Análisis de la cultura sobre seguridad del paciente en el ámbito hospitalario del Sistema Nacional de Salud español. Madrid: Ministerio de Sanidad y Política Social, 2009. [ Links ]

