










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.15 n.41 Murcia Jan. 2016
ADMINISTRACIÓN - GESTIÓN - CALIDAD
Burnout syndrome in nursing personnel of a referral hospital in Ibague, Colombia, 2014
Síndrome de Burnout en el personal de enfermería de un hospital de referencia Ibagué, Colombia, 2014
Grisales Romero, Hugo*; Muñoz, Yudi**; Osorio, Diana*** and Robles, Elena***
* Mathematician, Specialist in Statistics, Ph.D. in Epidemiology, Coordinator of the Universidad de Antioquia National School of Public Health Demography and Healthcare Research Group in Medellin. E-mail: hugo.grisalesr@gmail.com
** Specialist in Epidemiology
*** Nurse, Specialist in Epidemiology, Universidad del Tolima Colombia.
ABSTRACT
Objective: To determine the prevalence of the burnout syndrome (BS) in nursing personnel of a referral hospital in a Colombian city and their relation with demographic variables.
Materials and methods: a cross-sectional study was carried out on a random sample representative of 174 female and male nurses stratified based on if the nurse was a professional nurse or a nursing assistant in a referral hospital in the city of Ibague, Colombia. The MBI (Maslach Burnout Inventory) scale was used validated in Colombia. Tests of independence t were used for average differences and a one- way variance analysis. In the multivariate analysis, an explanatory binary logistic regression model was built with a measure of association; the OR is accompanied by its respective 95% confidence interval.
Results: The prevalence of the Burnout Syndrome was 20.1% (IC 95%: 13.9 26.4), and 52.3% are at risk of suffering from Burnout Syndrome, they were Nursing professionals who had a temporary job or who were supernumeraries, and personnel who worked in services including administration, oncology, orderlies and sterilization. Men and personnel who stated having more than one contract were the people who presented the highest Burnout indicator ratio of 20.1%. In the multivariate analysis, joint factors which perhaps have greater incidence in the presence of Burnout Syndrome include the number of children and the fact of being a man.
Conclusions: In comparison with other studies, this study reveals that the prevalence of the burnout syndrome in a referral hospital is greater.
Key words: Burnout Syndrome; nurses; prevalence; MBI (Maslach Burnout Inventory); Nurse Clinicians.
RESUMEN
Objetivo: Determinar la prevalência del Síndrome de Burnout (SB) en el personal de enfermería de un hospital de referencia de una ciudad colombiana y su relación con variables demográficas.
Materiales y métodos: Se llevó a cabo un estudio de corte transversal en una muestra aleatoria y representativa de 174 enfermeras(os), estratificada según si la enfermera era profesional o auxiliar, en un hospital de referencia de la ciudad de Ibagué, Colombia. Se utilizó la escala validada en Colombia del MBI (Maslach Burnout Inventory). Se utilizaron pruebas de independencia, t para diferencia de promedios y análisis de la varianza de una vía. En el análisis multivariado, se construyó un modelo de regresión logística binaria explicativo, con medida de la asociación el OR acompañado de su respectivo intervalo de confianza del 95%.
Resultados: La prevalencia de Burnout fue del 20.1% (IC 95%: 13,9 26,4) y además el 52,3% están a riesgo de padecerlo. Los profesionales de enfermería que tenían una vinculación temporal o de supernumerario, aquellos que laboraban en servicios administrativos/oncología/camillero/esterilización, los hombres y quienes afirmaron tener más de un contrato, fueron quienes presentaron indicadores de la proporción de Burnout mayores del 20,1%. En el análisis multivariado, los factores conjuntos que probablemente tienen mayor incidencia en la presencia del Burnout son el número de hijos y ser hombre.
Conclusiones: Con respecto a otros estudios, este revela que la prevalencia del síndrome de Burnout en el hospital de referencia es mayor.
Palabras clave: Síndrome de Burnout; Enfermería; Maslach Burnout Inventory; Enfermeras Clínicas.
Introduction
The first author to refer to the term burnout was Freudenberger in 1974, and he defined it as "a state of fatigue or frustration that occurs as a result of the devotion to a cause, or a form of life which does not produce enough gratification or effort" (1) nevertheless, the term burnout has been delimited and accepted by almost all of the scientific community based on the conceptualization Maslach and Jackson established in 1981. They defined the syndrome as a response to chronic stress formed by three fundamental factors: emotional fatigue, depersonalization and low personal fulfillment (2). The first factor refers to a feeling of fatigue which evidences a lack of interest for one's job; the second is defined as rejecting patients, and the third factor is perceived as a negative attitude towards oneself and one's job, a loss of interest for the job, irritability, low productivity and low self-esteem.
In this setting, it is important to bear in mind the emotional, physical professional repercussions of the presence of the syndrome in Nurses. The most known are depression, anxiety, alcoholism, drug dependence, trouble with group work and low productivity; hence, Burnout Syndrome is deemed to be an occupational disease. In addition to the above factors, there are others as: the stress generated by medical and paramedical personnel's work contract situations in Colombia. The situation in the country has harshened as a result of policies which have been in detrimental of healthcare workers' guarantees including restructuring to decrease patient care costs, contracting service provisions, changing work conditions, and implementing a new higher retirement age. The presence of Burnout Syndrome affects Nurses' quality of life, and this goes against the criteria of seeking users' satisfaction via a continued upgrading of quality, suitable technology, humanized care, qualified personnel, and personnel highly committed to the institution in accordance with the mission of the hospital where the data had been collected. In view of the importance of nursing personnel in any healthcare institution, and bearing in mind that it is one of the sectors which is most exposed to psychosocial diseases, it is essential to study their workplace conditions. Thus, there are many studies which have found high burnout prevalence in Nurses, and that this situation puts their health and their living conditions at risk, as well as the quality of the service they provide. Hence, Burnout Syndrome has been considered a public health problem in Nurses, not just because health is the most important asset people have, but also because of the repercussions, it may have on society and on the quality of patient care. These are issues that cannot be disregarded in the institutions where they work, and which have an unavoidable commitment to society. This is how the importance of conducting periodic studies regarding said phenomenon on hospital personnel is supported bearing in mind that important information from those studies may enrich a set of inputs necessary to foster Nurses' quality of work life.
The situation previously proposed merits determining the prevalence of Burnout Syndrome and its relation with the nursing personnel's characteristics in a hospital in the city of Ibague, Colombia. The aim is to contribute information to management to allow them to draw up strategies focused on upgrading healthcare personnel's wellbeing in the situations which are revealed.
Methodology
A cross-sectional study was conducted with information supplied by female and male nurses at a referral hospital in the city of Ibague, Colombia in 2014 from January to February. A questionnaire form the researchers designed was implemented. First, it asked for the nurses' demographic characteristics, and then, for Burnout Syndrome-related aspects based on Maslach (1982). Maslach, Schaufeli and Leiter's (1982) Maslach Burnout Inventory (MBI) is the most frequently used scale to measure Burnout Syndrome independent of the sample's occupational characteristics and origin. It is a questionnaire which consists of 22 items which uses three factors to evaluate including emotional fatigue, depersonalization and low personal fulfillment. The first factor consists of 9 questions with a score of 54, and it assesses the experience of being emotionally exhausted because of the personnel's demanding work; the second factor includes 5 items with a maximum score of 30, and it assesses the degree to which each person recognizes attitudes of coldness and aloofness. The third factor is comprised of 8 items with a maximum score of 48, and it evaluates personal feelings of self-efficacy and fulfillment at work. MBI scores between 1 and 33 are deemed low. High scores in the first two, and low in the third, define the syndrome. The above items presented as affirmative statements refer to professional feelings and attitudes at the workplace and towards patients, and its function is to measure professional burnout. People had to answer each one of the items indicated by a seven grade scale; it was the approximate number of times that the fact that the text describes took place. It presents seven alternate answers ranging from 0 (never) to 6 (everyday). A group of Universidad de Antioquia's psychologists and professors validated this instrument for Colombia in 2004(3).
The study population was formed by 831 nursing personnel (186 professionals and 642 nursing assistants). A sample of 174 female and male nurses was obtained from the above population, based on an absolute error of 5%, a 95 confidence index and an estimated 26.6% prevalence, taken from a study on Nurses' professional burnout in the city of Cartagena. The sample was stratified proportionately by type of Nurse, and obtained 131 nursing assistants and 41 professionals.
For the sample selection, a list of all the Nurses depending on type was input into a SPSS 20 statistical program, and then the nurses were chosen using simple random selection. Nurses who refused to participate or who did not have working relationships with the hospital were excluded. Information was systematized using Excel 2007 and SPSS 20 (SPSS®, Chicago). The tabular pictorial and textual presentation was done using a Word text processor and Windows XP. The tool was implemented after getting a written informed consent. The project which cleared the way to conduct this study was evaluated as not being a risk by the Referral Hospital's Ethics Committee's minutes 028 of 2013.
Results
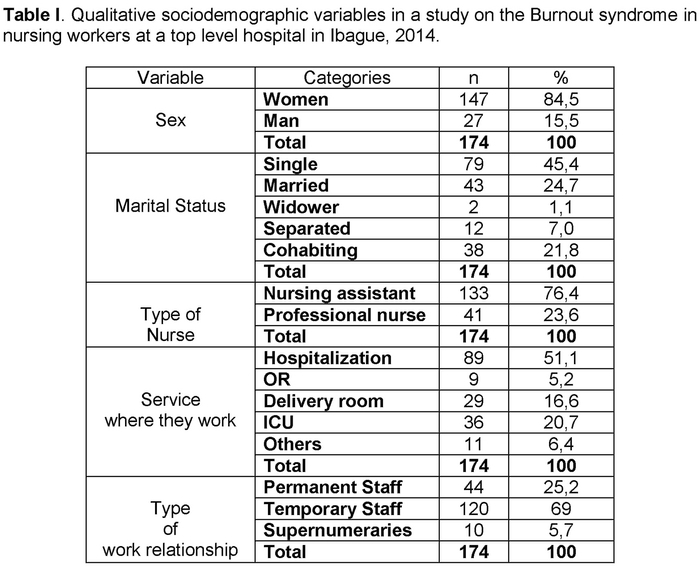
Women's greater participation (84.5%) was evidenced among respondents; regarding personnel's marital status, 46.5% of the personnel had some sort of a personal relationship of affection. According to the services interviewed, researchers observed that the greatest participation was that of the nursing personnel working in the hospitalization service (51.1%) followed by personnel assigned to ICUs (20.7%) and delivery rooms (16.6%); the people who least participated were administrative personnel, central sterilization personnel, orderlies and oncology personnel (6.4%). 69% of the nursing personnel were temporary workers followed by permanent staff workers and just (5.7%) were supernumeraries. (Table I).
Nursing professionals and assistants in the referral hospital were in average 33.7 years old (SD: 9.2); the average number of the target personnel's children of the analysis was 1.1 (SD: 1.1); 50% were 32 years old or younger. Furthermore, 75% of the personnel interviewed were 38 years old or younger, and the most frequent age was 24. 50% of the respondents said they had just one child, and the highest frequency of personnel without children was outstanding. In average, the nursing personnel have worked in the hospital 9.7 years (SD: 8 years), and 50% of the personnel interviewed have worked 8 years in the hospital since they graduated. The female and male nurse who had worked the longest in the institution had been there for 40 years when the survey was implemented, and the one who had worked the least had been there one year. The hours worked were presented with a maximum 24-hour shift and a minimum 6-hour shift. On the month when the survey was implemented, most of the nursing personnel had worked 184 hours, and 75% of the respondents stated that they had only one job.
Types of Burnout Syndrome
In the original MBI manual, Maslasch and Jackson used a tripartite classification of the variability of the results on the tool. Thus, three possible values were established including High, Medium and Low in accordance to what was found on the superior third, medium or lower thirds of the possible values (4). With this purpose, the value segment in the three zones high, medium and low was divided taking as cutoff points percentiles 33 and 66. For the purpose of this research, the values proposed on the general sample and in each one of samples were calculated depending on type of labor relationship with the Hospital to proceed as previously described. The implementation of this classification of nursing personnel is presented in table II. In general, of the three categories of Burnout Syndrome, the low level predominated, bearing in mind that the first two correspond to positive indicators while the last is a negative indicator.

For this study, the procedure used by Manassero and Guerrero to assess the levels of the Burnout Syndrome was replicated establishing five different levels based on the possible calculated combinations of percentiles 33 and 66 which were used as cutoff points. According to the above, Burnout levels were classified as follows: none, a little, medium, a lot and extreme (5,6), and according to the above, the distribution of the frequencies of the different levels of Burnout (Table III) was analyzed, and it was observed that 43.1% was located between levels "none" and "little". 20.1% of the nursing personnel was located in the "extreme" level, and 36 % was found to be above the medium levels of Burnout.

To calculate the Burnout prevalence, some levels were grouped for a new tripartite classification formed by: without Burnout, at risk of Burnout and with Burnout. In figure 1, the distribution of Burnout Syndrome in three categories is observed. In general, the Burnout prevalence for this research was 20.1%, and in the hospital's nurse population, it was found between 13.9 and 26.4%. It is important to highlight that 52.3% are at risk of suffering from the syndrome.

When linking the levels of Burnout Syndrome with type of Nurse, it was found that 19.5% of the nursing assistants and 24.4% of the professionals presented the syndrome. Furthermore, it is worth noting that 31.5% of the nursing assistants and 53.7% of the professionals were at risk ranking between medium and a lot.
Regarding MBI dimensions, the range of scores varied from 0 to 43 in the emotional fatigue dimension for the hospital's nursing personnel in which the median was 14.4 points (DE: 9.3). 50% of the personal had 10 or less points in this dimension, and 50% of professional nursing personnel scored 15 or less. For assistant personnel, the average was 12, and the maximum score was 33. The average for permanent staff was 12 points based on type of work relationship. Temporary personnel had an average score of 15 and a maximum of 38 while supernumeraries had an average score of 18 and a maximum of 28. For the dimension of depersonalization for the general sample, a 4.1 point (DE 4.9) average was obtained. 50% of the personnel scored 2 or less. Depending on the type of nurse, nursing assistants' average score was 1, and the average score for professionals was 6; depending on the type of work relationship with the hospital, the permanent staff had an average score of 1 in the depersonalization category, and temporary workers had an average score of 3; finally, supernumeraries had an average score of 7 points, and a maximum of 18. In the dimension of personal fulfillment, the score was the inverse of the two previous dimensions. In the sample, a 40.3 point (DE: 8,1) average was obtained for assistants and professionals, and had a 41 point average; depending on the type of work relationship, the average in this dimension behaved similarly for the three groups; it had a 42 point average, and a maximum score of 48.
The presence of Burnout Syndrome in men (44.4%) was more prevalent with a statistically significant association (p = 0,002). Even though the Burnout ratio was higher in 24.7% who did not have a formal partner relationship at the time of the study, in professional nurses 22.0%, and 21.5% in personnel who stated they had a work relationship different from permanent staff, and in those who stated they had two contracts, the differences regarding the Burnout ratio of married/cohabiting assistant nurses compared with permanent staff and people who had a contract were not significant respectively (p > 0,05 in all cases) (a chi square test of independence and a likelihood-ratio test). Note that even when the type of service where the Nurses worked was considered, it was in the Administrative/Oncology/Sterilization/Orderlycategory where the highest presence of Burnout Syndrome was found. This finding has to be carefully analyzed, for the frequency of having female and male nurses in these services is very small. From this point of view, 20.2% Burnout prevalence at the hospitalization service is more relevant although the set of differences found were not significant.
Except for age in years people actually have which was distributed normally in the Burnout Syndrome categories of "none" and "extreme", the other variables in consideration did not fulfill this assumption. Then, it was determined if there were any statistic differences in age averages/medians in Burnout Syndrome categories. Only the differences of medians were significant regarding the number of children in Burnout Syndrome categories (Kruskal Wallis H test). 50% of the nursing personnel who presented Burnout were 32 years old (D.E=7.3 years). Furthermore, it was observed that as the number of children increased, the risk of the syndrome increased; even if the differences were not significant when it was compared to other Burnout Syndrome categories (p > 0.05) (figure 2).

In brief, when the 20.1% burnout prevalence found was considered the cutoff point, it was the men who stated they were single/widowers/separated, nursing professionals who had a temporary work relationship or were supernumeraries, who worked in administrative/oncology/orderly/sterilization services and those who stated they had more than one contract were the ones who presented prevalence values higher than general hospital values in nursing personnel (figure 2).
In view of the measuring level of the dependent Burnout variable (None - at risk-with Burnout), we proceeded to construct an ordinal regression model (7) which did not yield significant results for any of the independent variables considered on the association tests with Burnout Syndrome. Hence, we proceeded to construct an exploratory logistic regression model which is detailed as follows. It is worth noting that even if the study is a prevalence study, it is pertinent from an epidemiological point of view to form two groups in the analysis. One group was one that had the event and another which did not. Then, we proceed with the analysis as if this were a case-control study. In accordance with Hosmer-Lemeshow criteria, those who presented a p < 0.25 in association tests with each one of the independent variables in the bivariate analysis were considered candidates to form an exploratory logistic regression model for Burnout Syndrome (0: No 1:Yes). That is number of children, age, sex, marital status, type of service where a nurse works and the type of work relationship of female and male nurses. The study warns that in the construction of said model, the category of "at risk" of burnout was omitted, for it was deemed irrelevant to coordinate this category to one of the two remaining ones (8).
In this model, said variables were input to assess their meaning jointly with the presence or non-presence of Burnout Syndrome; also, it was found that the risk of Burnout Syndrome in men, in professional nurses, in single men/widowers/separated men, and people who worked in the hospitalization service or at the ICU, and people who had a temporary job or supernumerary job, that the risk of Burnout Syndrome was higher in men (OR's more than 1 in all cases yet they were not significant). The model above was revaluated so that only the variables that had an important effect on the dependent variable would form it. To do so, we proceeded to apply a method of selection by steps or stepwise which leaves in the model only those variables that met the input criteria which was elected from p less than 0.10. It was found that the risk of Burnout in nurses with children was 2.5 times in comparison with those that did not have any children (CI: 95%; OR: 1.3, 5.0). Likewise, the risk of Burnout in men is 2.9 times more compared with female nurses. It is worth noting that these two variables explain the variability of Burnout Syndrome as 10.3%. The other independent variable did not have joint meaning in its association with Burnout Syndrome. In conclusion, the model suggests that being a man and having children possibly increases the risk of acquiring the syndrome.
Discussion
This study presents the burnout syndrome experience in nursing personnel at a Hospital in the city of Ibague, Colombia. In Colombia, there are few studies on Burnout syndrome in nursing personnel despite the fact that it constitutes an emerging problem because of the high levels of physical, psychological and social demands that nurses are submitted to in their workplace in addition to wrongful hiring laws that regulate them. The complexity of the syndrome implies an analysis with a large number of variables. They can influence the presence of the syndrome, so in recent years, studies on this matter have been increasing, and they have been studying in-depth the identification and evaluation of the possible causes, determinants and adjacent process to the syndrome. Furthermore, the idea is to know clearly why people respond differently to stress, what type of interaction may occur between organizational and personal variables (9).
Bearing in mind what was proposed above and complying with the objectives of this study, the scores obtained were analyzed, and certain similarities were found between the variables proposed, and related to other studies conducted on an identical population group and/or health sector.
This study evidenced greater female participation (84.5%) which followed the trend observed in studies as the one Romero(10) conducted on the same population group of a third level hospital in 2013 (86.4%). Raftopoulos'(11) study rendered 80.4% which suggests women's important role in the sample selection, and this was something to be expected because nursing is a predominantly female profession.
To evaluate Burnout Syndrome at work, a short version of Maslach was used; the questions with the highest mean scores corresponded to the personal fulfillment dimension, and the highlights were: "I feel I can easily create a pleasant environment with my patients", "I feel I can communicate easily with the people I have to interact with at work" and "I feel I have great energy at work". This made the prevalence of syndrome increase considerably, for it was evaluated negatively. These results were similar to the ones Ortega and Ortiz (12) obtained and to the ones in Vinaccia and Alvaran's study (9).
Regarding the prevalence of the burnout syndrome, it is important to notice that it is difficult to compare it with other studies because of the diversity of tools used, the samples and cutoff point. In this study, prevalence was 20.1% which indicates an increase in people suffering from Burnout Syndrome, for in the studies reviewed, the highest prevalence presented in nursing personnel in Colombia had been 26.6%(13) in the city of Cartagena; while in Contreras, Avalos and Romero in México,(14) prevalence was 74.6%. This increase is perhaps due to an accelerated lifestyle currently evidenced in the world; time seems reduced to being able to perform activities specific to a profession. Furthermore, the situation the healthcare system is going through in Colombia affects patients' treatment plan and employee's guarantees (salary, incentives, and work stability). Likewise, it is worth highlighting that 52.3% of the personnel interviewed in the referral hospital are at risk of developing a Burnout Syndrome, so it is of vital importance that the referral hospital's management conduct a prevention program and create intervention strategies throughout the general workplace risk system at that institution to reduce workplace-related stress, and through which they seek to establish strategies focused on avoiding work overload, improving work environment, and granting real importance to the need to have time to do leisure activities which allow the strengthening of interpersonal relations and healthy lifestyles which become protective factors.
When the association between the presence of Burnout Syndrome with age, marital status, type of nurse, the service where people worked, time worked since they finished their studies, daily hours on the job, monthly hours on the job and number of contracts was explored, the risk of presenting the syndrome was higher in men, in professional nurses, in single men/widowers/separated men, in people who worked in hospitalization or in the ICU when the survey was implemented at the hospitalization services or at the ICU services, and in people who were temporary workers/supernumeraries even though the differences were not statistically significant (p > 0,05). These results are consistent with the theoretical basis of the origins of the syndrome which states that it mainly occurs in a workplace environment and in workplace conditions. The non-statistical relation of the variables mentioned before with the event of interest could be explained because the tool implemented mainly focused on dealing with psychological aspects before dealing with workplace conditions. This suggests that an observational study on nurses' satisfaction on the job had to be conducted beforehand to enable a more in-depth closeness with the roots that unleash the syndrome.
Working more in-depth the origins of Burnout Syndrome, nursing is a profession with a high degree of contact with people, excess work schedules and extended work schedules. Furthermore, it has workplace environment related situations, and there is financial remuneration, so it may become a risk factor for the presence of the syndrome. In healthcare personnel, there is a risk for the personnel's mental health; for it may generate changes in the way the usefulness of the job is perceived. Gil Monte argues that Burnout Syndrome is a response to chronic work stressors, and that it comes with negative feelings and attitudes that cause psychophysiological alterations in a person's body. These are facts that can be mitigated in the population studied channeling energies in external activities and in a suitable work relationship (15). One of the classical manifestations of work fatigue and stress, according to Lazauro and Folkman, it is the result of an individual and setting ratio, which when it is chronic, it originates in people as an unbalance in their biopsychosocial homeostasis. It comes prior to the onset of the syndrome at a future time, and it may be positive or negative. The first is a trend for personal fulfillment and the second as a self-destruct mechanism (16); in this sense, Hans Seyle defined positive stress as a body toner while negative stress consumes body strength causing disease. Based on what was proposed, we evidenced that part of the nursing personnel population in the study have positive stress because even if they interact with their stressor they keep an open mind and are willing to work, and this may minimize mental health problems and unsatisfactory experiences (17).
Therefore, we reiterate the proposal indicated to study in-depth the knowledge of the hospital's work environment, for the MBI per se does not ask about this crucial aspect for the appropriate functioning of every institution in general and this particular hospital.
It is noticeable that Burnout Syndrome was more prevalent in men (44.4%); this can be explained because men generally present feelings of low personal fulfillment on the job, and this is an agent triggering stress, specially, because of a lack of social support or at the level of Leiter's professional fulfillment (18); In Vinaccia's(9) study, the syndrome was more prevalent in women.
People who had the highest number of children presented an extreme Burnout Syndrome, and this could be explained by nursing personnel's duties at work along with the personnel's role as father/mother and spouse. This may have a negative effect on their overall quality of life, and on their emotional burnout which is the opposite of Rodríguez Paipilla's study in Bogota (2011) [38,] in which a lack of Burnout was related to the number of children.
It is worth highlighting that there is a relation between Burnout Syndrome and the various hospital services because depending on the level of complexity, people require aptitudes that not all workers have including vocation, devotion, psychological and emotional stability, also physical health and capability to work. These are components which enable workers to face the burden of care and the emotional burden in these services.
According to Gil Monte and Peiro(15), the role of nursing generates a great deal of uncertainty, for professionals have doubts quite frequently regarding how much they have gotten involved with their patients, regarding how to deal with their problems and with the insecurity concerning if they are doing things adequately. On the other hand, patients, just like family, are usually anxious and worried, and interacting with them is not gratifying. Along with these situations, there is also a series of variables that the Nurses cannot control including patients' cooperation and their recovery or death, medical and administrative decisions, bureaucratic procedures, a lack of social support and conflicts with doctors and coworkers.
We recommend the hospital management to draw up an intervention program for the factors that this research unveils which can be intervened and whose indicators are still far from being the best. In this sense, specialists on the topic recommend simple actions like forgetting work problems outside work, doing relaxation techniques, like stopping to take small breaks during the work shift. These interventions must be directed by the institution's occupational health office with the support of a professional in psychology.
It is indispensable for the referral hospital to implement plans within its general workplace risk system (Ley 1562 de 2012) (19) so that they may tend towards the improvement of the company's environment. It is also necessary to monitor the cases of Burnout Syndrome which have been detected and to seek mechanisms via a preventive medicine program.
Conclusions
• Women's participation was higher (84.5%) among respondents. Nursing professionals and assistants of the referral hospital presented an average age of 33.6 years old (DE: 9.1), in which 75% were 38 years old or younger, and the most frequent age was 24 years old.
• The Burnout prevalence was 20.1 %, (IC 95%: 13.9 - 26.4%). 52.3% are at risk of suffering from the syndrome.
• The prevalence of the Burnout Syndrome in nursing assistants was 19.5% and in professionals 24.4%.
• Male nursing professionals who stated that they were single men/widowers/separated men, when the survey was implemented had a temporary work relationship or were supernumeraries who worked in administrative/oncology/orderlies/sterilization services and those who stated that they had one contract, and they presented prevalence values of more than 20.1%.
• The nurses who stated that they were single and who had a temporary work relationship preferably presented Burnout Syndrome.
• Being a man and being a father may possibly increase the risk of acquiring the syndrome (OR's of 2.9 and 2.5 respectively).
Acknowledgements
The researchers thank the Management of the referral hospital for their availability to authorize the implementation of this tool.
Also, they thank all the nurses of the referral hospital for their participation in the study.
Finally, they also thank Universidad del Tolima University's Epidemiology Coordination for facilitating the process through their intermediation with the Management of the referral hospital to facilitate the information collection process.
Received: November 21, 2014
Accepted: December 20, 2014
References
1. Freudenberger M. Staff Burn-out. Journal of Social Issues. En: Illera D. Síndrome de Burnout, aproximaciones teóricas. Resultado de algunos estudios en Popayán. Revista Facultad Ciencias de la Salud 2006; 8 (3). [ Links ]
2. Moriana J, Herruzo J. Estrés y Burnout en profesores. IJCHP 2004; 4 (3): 597-621. [ Links ]
3. Restrepo N, Colorado G. Desgaste profesional (Burnout) y su asociación con factores de riesgo psicosocial en docentes oficiales de Medellín, Colombia, 2005. (Tesis de Maestría en salud ocupacional). Medellín: Universidad de Antioquia; 2005. [ Links ]
4. Maslach, C., & Jackson, S. E.. Burnout in the health professions: A social psychological analysis. En: Sanders G, Suls J, editors. Social psychology of health and illness. Hillsdale, NJ: Erlbaum; 1982. Pp 227-251. [ Links ]
5. Manassero M, Vázquez A, Ferrer V, Fornés J y Fernández, M. Estrés y burnout en la enseñanza. Palma de Mallorca: Ediciones UIB; 2003. [ Links ]
6. Guerrero E, Rubio JC. Fuentes de estrés y síndrome de "burnout" en orientadores de institutos de Enseñanza Secundaria. Revista de Educación 2008; 347: 229-254. [ Links ]
7. McCullagh P. Regression models for ordinal data. Journal of the Royal Statistical Society. Series B (Methodological) 1980; 42 (2): 109-142. [ Links ]
8. Hosmer DW, Lemeshow S. Applied Logistic Regression. New York: Wiley; 2000. [ Links ]
9. Vinaccia S, Alvaran L. El síndrome del Burnout en una muestra de auxiliares de enfermería: un estudio exploratorio TERAPIA PSICOLÓGICA (revista en internet) 2004 (Acceso 14 de julio de 2014); 22(1). Disponible en http://teps.cl/XpTQV/files/2011/06/art-1-.pdf. [ Links ]
10. Romero J. Diseño de un programa para disminuir los síntomas del burnout en los profesionales sanitarios. (Tesis de grado) España: Universidad de Almería; 2013. [ Links ]
11. Raftopoulos V, Charalambous A y Talias M. The factors associated with the burnout syndrome and fatigue in Cypriot nurses: a census report. 2012. BMC Public Health (revista en internet) 2012 (Acceso 20 de Agosto de2014); 12(457). Disponible en: http://www.biomedcentral.com/1471-2458/12/457. [ Links ]
12. Ortega ME, Ortiz GR y Coronel PG. Burnout en médicos y enfermeras y su relación con el constructo de personalidad resistente. 2007. Psicología y Salud (revista en internet) 2007 (Acceso 18 de agosto de 2014); 17(1). Disponible en: http://revistas.uv.mx/index.php/psicysalud/article/viewFile/730/1287. [ Links ]
13. Cogollo-Milanés Zuleima, Batista Edith, Cantillo Chanelly, Jaramillo Alicia, Rodelo Dalys, Merina Gary. Burnout e fatores associados em trabalhadores de enfermagem em serviços de emergência em Cartagena (Colômbia). Aquichán (serial on the Internet). 2010 Apr (cited 2014 Apr 16) ; 10(1): 43-51. Disponible en: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S1657-59972010000100005&lng=en. [ Links ]
14. Contreras-Palacios SC, Ávalos-García MI, Priego Álvarez HR, Morales-García MH, Córdova Hernández JA. Síndrome de Burnout, funcionalidad familiar y factores relacionados en personal médico y de enfermería de un hospital de Villahermosa, Tabasco, México. 2013. Horizonte sanitario (revista en internet) 2013 (Acceso 20 de julio de 2014); 12(2). Disponible en http://www.publicaciones.ujat.mx/publicaciones/horizontes_anitario/ediciones/2013_mayo-agosto/REVISTA_HS_mayo-agosto2013.pdf#page=16. [ Links ]
15. Gil-Monte PR, Peiró JM. Desgaste psíquico en el trabajo: el síndrome de quemarse. Madrid: Editorial Síntesis; 1997. [ Links ]
16. G. Hernández L, Olmedo E, Ibáñez I. Estar quemado (burnout) y su relación con el afrontamiento. International Journal of Clinical and Health Psychology (revista en internet) 2004 (Acceso 13 de julio de 2014); 4(2). Disponible en: http://dialnet.unirioja.es/servlet/articulo?codigo=854282. [ Links ]
17. Alvarado Calderon. Validez factorial de maslach burnout inventory (versión castellana) en educadores costarricenses. Actualidades Investigativas en Educación (revista en internet) 2009 (Acceso 10 de julio de 2014); 9(1). Disponible en http://revista.inie.ucr.ac.cr/uploads/tx_magazine/validez.pdf. [ Links ]
18. Gascón S, Olmedo M, Ciccotelli H. La prevención del Burnout en las organizaciones: el chequeo preventivo de Leiter y Maslach. Revista de Psicopatologia y Psicología Clínica (revista en internet) 2003 (Acceso 12 de junio de 2014); 8(1). Disponible en http://e-spacio.uned.es/revistasuned/index.php/RPPC/article/view/3942. [ Links ]
19. República de Colombia, Ministerio de trabajo. Ley 1562 del 11 de julio de 2012: Por la cual se modifica el Sistema de Riesgos Laborales y se dictan otras disposiciones en materia de salud ocupacional. Bogotá: El Ministerio; 2012. Disponible en http://mintrabajo.gov.co/normatividad-julio-leyes-2012/712-ley-1562-del-11-de-julio-de-2012.html. [ Links ]

