










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.15 no.44 Murcia oct. 2016
DOCENCIA-INVESTIGACIÓN
Influence of physical activity and nutritional habits on the risk of metabolic syndrome
Influencia de la actividad física y los hábitos nutricionales sobre el riesgo de síndrome metabólico
Morales, M.a Isabel Arandojo*; Pacheco Delgado, Valeriano** and Morales Bonilla, José Antonio***
*Nurse. PhD candidate by Nursing, Physiotherapy and Podiatry School of UCM. Medical service of Colegio de Guardias Jóvenes "Duque de Ahumada" of Guardia Civil. Valdemoro, Madrid. E-mail: maribelarandojo@gmail.com
**Nurse. Medical service of Traffic School of Guardia Civil. Merida. Badajoz.
***Nurse. Medical service of Colegio de Guardias Jóvenes "Duque de Ahumada" of Guardia Civil. Valdemoro, Madrid. Spain.
ABSTRACT
The combination of several risk factors caused by obesity, sedentary lifestyle or different genetic factors, leads to suffer "metabolic syndrome", which increases the chance of developing cardiovascular disease.
Objectives: Describe the risk of cardiovascular disease in members of Guardia Civil from a military complex in Madrid.
Material and Methods: Descriptive cross-sectional study carried out by a 30 questions-survey, analytics and anthropometric measurements to the Guardia Civil staff who came to the medical service of their quartering between September 1 and October 31, 2014.
Results: Sample of 76 subjects aged 20-62. 7'89% of individuals have three or more parameters related with metabolic syndrome diagnosis.
Conclusions: Sedentary lifestyle and poor nutritional habits act negatively in lipid profile, blood pressure and BMI, increasing the risk of metabolic syndrome and, therefore, cardiovascular diseases.
Keywords: Obesity; sedentary lifestyle; metabolic syndrome; cardiovascular disease.
RESUMEN
La conjunción de varios factores de riesgo originados por la obesidad, el sedentarismo o por diversos factores genéticos, lleva a padecer el llamado "Síndrome Metabólico", que incrementa la posibilidad de desarrollar enfermedades cardiovasculares.
Objetivos: Describir el riesgo de padecer enfermedades cardiovasculares que tienen los miembros de la Guardia Civil de un complejo militar de Madrid.
Material y método: Estudio descriptivo transversal, realizado mediante encuesta de 30 preguntas, analítica y medidas antropométricas al personal de la Guardia Civil que acudió al servicio médico de su acuartelamiento entre el 1 de septiembre y el 31 de octubre de 2014.
Resultados: Muestra de 76 sujetos de entre 20 y 62 años. El 7'89% de los individuos tiene tres o más parámetros para el diagnóstico del Síndrome Metabólico.
Conclusiones: El sedentarismo y los malos hábitos nutricionales actúan negativamente en el perfil lipídico, TA y el IMC de los individuos, haciendo que estos tengan más probabilidades de padecer SM y, por tanto, enfermedades cardiovasculares.
Palabras clave: Obesidad; sedentarismo; síndrome metabólico; enfermedad cardiovascular.
Introduction
In the last 50 years, there have been significant changes in our society. Today's man is more educated, scientific technical advances reach all places of the world and human knowledge has raised in every meanings, so that work is more intellectual and requires less physical effort in general. This has resulted in changes in the social life and in the activity of people, which has led to the population to have higher weight index and thus, associated diseases that constitute a serious future problem for public health1.
Health is a social value, which is related to the quality of human existence. And it is this quality, and the way of life of our society, which have led to the population to present higher rates of increasingly overweight and thereby associated pathologies appear, which constitute a challenge and a serious problem for future public health. Even some authors present the hypothesis that current children and teenagers may be the first generation with a lower life expectancy due to that cause, by the apparition of certain diseases at earlier ages than in previous generations1.
The percentage of overweight people is increasing at an alarming rate in industrialized countries. It is spent more time in front of the TV, the computer, the videogame platform or just sitting, and less time exercising. The problem is of such magnitude, that World Health Organization (WHO) provides the following data about obesity and overweight2:
• Since 1980, obesity rate has doubled worldwide.
• In 2008, 1400 million of adults (aged 20 and older) were overweight. Within this group, more than 200 million men and close to 300 million women were obese.
• 65% of the world's population lives in countries where overweight and obesity cause more deaths than underweight (body mass index < 18.5).
• In 2010, about 40 million children under five years old were overweight.
In the same informative note, the WHO sets as fundamental cause of overweight and obesity the increase in the intake of energy-dense food and the descent in the physical activity by a way of life increasingly sedentary. Thus, body weight is based on energy balance: A positive energy balance leads to weight gain, while a negative energy balance has the opposite effect.
It is indisputable that we need to eat to live, but eating is not the same as nourishing. Eating is the action that allows you to introduce into the body the necessary food. Nourishing, however, is the combination of processes by which the human body incorporates, transforms and uses the nutrients supplied with food3. It happens unwittingly after ingestion of food, so it depends on its quality, which is very important to be healthy, sufficient, complete, harmonious and appropriate. It is considered sufficient the food that provides the optimum amounts of energy, essential nutrients for life and the amount of dietary fiber needed for proper bowel function3.
Energy and nutrients needs are different for each individual and depend on their basal metabolic rate (energy expenditure of an individual in complete physical and mental rest, 14 hours after having eaten, at a room temperature of 20 degrees), of daily activity (light, moderate or heavy) and sex, and can range from 1450 kcal / day for small sedentary women, to 4250 kcal / day for large and very active men2. An ideal diet provides enough calories to reach energy needs, but not excessively, since this would cause an increase of weight.
On the other hand, sedentary lifestyle can be defined as the action which is contrary to activities that involve the body movement and represent an energy expenditure greater than which would correspond to the basal metabolism4. A sedentary person is that one who invests less than a 10% of its daily energy expenditure in the realization of physical activities that require at least 4 MET. One MET is the energy consumption of an individual in a resting state (basal metabolic expenditure), which is equivalent to approximately 1 kcal per kilogram of weight and hour5. Duration, frequency, intensity or environment where the activity is carried out can be measure to calculate the METs, according to Ainsworth model6, which awards a number of METs to each activity. The intensity or effort required depends on how trained is each one and its physical form, and it can be divided into three intensity levels according to the METs needed to make it6,7.
• Light activity: less than 3 METs, in activities such as walking, elasticity exercises or exercises on the floor...
• Moderate activity: from 3 to 6 METs, in activities such as brisk walking, doing housework, gardening, weight training, dancing...
• Intense activity: more than 6 METs, in activities such as running, soccer and other competitive sports, aerobics...
The progressive decrease of the physical activity in the social life also has made the health disease-process change, because it is obvious that diseases as heart attack, alcoholism or accidents are more related with the life conditions of the individuals than with genetic and physiological factors8, so that sedentary lifestyle turns in an independent and modifiable risk factor for cardiovascular disease (CVD).
Obesity can be defined as the accumulation of fat in tissues, which is usually accompanied by an increase in body weight. This body weight is influenced by height and, therefore, to assess the nutritional status of an individual, it is necessary to consider this, so that from both measures the Body Mass Index (BMI) is calculated9, which is interpreted as a measure of how the mass of the individual is distributed per unit of body area.
The parameters used are simple and easy to obtain and its calculation is also simple, using the formula "weight kg /(height in meters)2", so that it becomes a very useful tool. The result obtained is compared within a few values, presented in the Table I10.This is highly correlated with body fat, so it is a widely used Method to describe the presence of obesity and classifying the individual according to their adiposity degree, but it is also a good descriptor of deficiency states. BMI alone cannot predict health risk, but most experts agree that more than 30 index (obesity) is unhealthy11 Being overweight overloads your heart and can lead to serious health problems such as heart diseases, hypertension, type 2 diabetes, etc., making obesity along with physical inactivity, another independent and modifiable risk factor for CVD.

CVD comprises a group of disorders related to the formation and development of atherosclerotic processes12. The variables that increase the odds that a person has a CVD are called risk factors, which are multiple, and most of them are modifiable and associated with lifestyles. Some of these cardiovascular risk factors occur together in certain people and this combination of factors is called "metabolic syndrome" (MS), also called "Reaven Syndrome" or "Insulin resistance syndrome"13. It is not a single disease, but the association of health problems that can occur simultaneously or sequentially in the same individual14 and which main elements are:
• Insulin resistance: increase of basal insulin to keep blood sugar within a normal range.
• Impaired glucose tolerance: defects of the insulin action cause hormone inability to suppress the production of glucose by the liver and kidney, as well as alterations in the metabolism of glucose.
• Abdominal obesity, associated to accumulation of adipose tissue in the abdominal viscera.
• Atherogenic dyslipidemia: increase in the synthesis of triglycerides (TG) and lowering cholesterol HDL.
• Arterial hypertension: according to the WHO, so that a patient is considered hypertensive blood pressure must be equal to or greater than 140-90 mmHg and according to the NCEP-ATP III (National Cholesterol Education Program Adult Treatment Panel III) it must be greater than or equal to 135-85 mmHg. If a patient has a blood pressure lower than this figure but with treatment antihypertensive, that person will also be considered hypertensive.
There are several criteria for the diagnosis of the MS proposed by international expert bodies, which differ in their components and cutoffs 14.16 (Table II). There is no internationally agreed definition of MS, but the most widely used criterion for population studies is the NCEP-ATP III 13, that considers that a person has MS when that individual has at least three of the problems described previously, so that will be the criterion to be followed for this study.

In short, MS is the name given to a group of risk factors that increase the likelihood of developing heart disease and other health problems such as diabetes and stroke17. It is considered nowadays a clinical and public health problem. It is estimated that 1/4 of the world's population has it, causing them twice as likely to die and three more to have a myocardial infarction or stroke and five more of developing type 2 diabetes mellitus, in addition to increasing the frequency of arterial hardening, left ventricular hypertrophy and diastolic dysfunction, regardless of present arterial hypertension18. The patients do not feel any symptom, but there are signs that can shed light on their diagnosis as a conjunction of abdominal obesity, impaired glucose tolerance or type 2 diabetes, high levels of LDL and TG in the blood, low levels of HDL and high blood pressure 13.
The pathogenesis of this syndrome has many origins, but obesity and sedentary lifestyle, coupled with inadequate diet and not well-known genetic factors, favor its appearance and its increasing incidence and prevalence. In fact, it is due to different causes acting together. Some can be controlled and others not and the probabilities of developing MS increase with age.
Objectives
General
Describe the risk of suffering from CVD, through the diagnosis of the MS, that the members of the Guardia Civil serving in a quartering of Madrid have.
Specific
1. Describe the structure of the group in terms of their eating habits and physical exercise.
2. Describe the prevalence of MS in the study group, as well as the average values of the variables involved.
Material and Methods
Cross-sectional study with members of the Guardia Civil serving in Madrid, in a quartering where various operating and non-operating units are located.
The study was conducted among individuals who attended the medical service between September 1 and October 31, 2014 in order to make an analytic, each one for their particular reasons. No exclusion criteria were considered, the only inclusion criterion was their willingness to participate in the study. All participants agreed to offer their analytics to obtain the necessary data (glucose, cholesterol, HDL, LDL and triglycerides) and to complete a survey of 30 questions about eating habits and physical activity, previously validated and subjected to a pilot study. We measured their blood pressure (BP), weight, height and waist circumference. All individuals who were asked agreed to participate, but subsequently 7 were refused due to mistakes in the completion of the survey. In the end, a sample of 76 individuals, 58 men and 18 women, aged between 20 and 62 years was achieved.
For the diagnosis of MS, we have used the NCEP-ATP III criteria. Analytical samples were obtained after 8-10 hours of fasting and were processed in the same laboratory, where they have as normal reference values in mg / dl: glucose 75-115, cholesterol 50-220, HDL 35-120, LDL 45-150 and triglycerides 50-130.
Weight and height were measured on a calibrated scale with a measuring rod, BMI is calculated using the formula weight in kg/(height in meters)2, the waist circumference was measured at the navel, standing and with bare belly and for the blood pressure we used a digital sphygmomanometer.
As for physical activity, we have obtained data on the type and frequency, duration and environment in which it is performed and we have used metabolic equivalents or METs to measure its intensity, whether it is physical activity or sedentary activity.
Those data have been processed through the programs Excel 2010 and SPSS 20. Quantitative variables are presented as mean ± standard deviation and as statistical we have used Student t test to compare measures and Pearson correlation coefficient (r) to relate variables, both with a significance level ≤5% (p-value ≤0'05). Due to the descriptive nature of the study, they have not been used to infer other statistical Results.
Results
The sample obtained consists of 76'32% men and 23' 68% women. This disproportion between the sexes is due to the environment in which the study was conducted, a military cantonment where the male dominated. The average age is 45'34 ± 10'66 years in men and 33'00 ± 11'52 years for women.
Anthropometry and analytical data
The men have significantly more high values than the women in weight, height, BMI and waist circumference, but also in LDL and triglycerides and the women who have any alteration, is in glucose and BP values.
Only in males, a significant increase is observed in the lipid profile. 65'71% has high values of LDL, 31'03% cholesterol and 10'34% triglycerides. 20'69% has BP above 135 / 85 mmHg.
BMI and diet
BMI average is 27'46 ± 2'48 in men and 21'44 ± 2'11 in women and that is related to the age (r = 0'402, p = 0'012), so that in the range of 50 to 59 years, 26'31% were overweight people, men all of them. 52'63% of the total were overweight, which added to 7.89% of obese, gives us the information that a total of 60'52% of subjects have problems with their weight, although 71'05% believe that takes a proper diet.
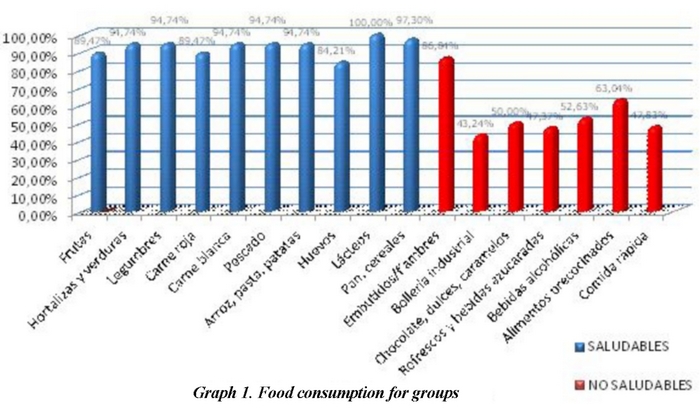
Consumed food was distributed in two groups: healthy (daily intake recommendation)20 and not healthy (occasional recommendation) finding they consume a greater quantity of those considered healthy and less of occasional consumption (graph 1). Comparing the frequency of consumption in days a week with BMI of individuals, as BMI increases, decreases the consumption of healthy foods and subjects who have 3 or 4 parameters for the diagnosis of MS significantly increase consumption of unhealthy foods.
Metabolic syndrome
5'26% of individuals have 3 parameters for the diagnosis of MS and 2'63% have 4 parameters, making 7'89% of subjects have a greater cardiovascular risk, all them men. 31'58% of participants has two parameters, so that these people are not diagnosed of MS but have high glucose, waist circumference, and blood pressure rates.
The risk of SM also has been linked to the consumed foods, according to the distribution of these in healthy and non-healthy and it can be seen that, just as happened with BMI, while healthy foods are consumed several times a week and with a more or less constant frequency in all individuals, subjects who have 3 or 4 parameters increase considerably the consumption of unhealthy foods.
Individuals who were up to 29 years old only have a parameter for the diagnosis of MS or have none, but the number of risk factors increases with age (r = 0'403, p = 0'000), so that in the range of 50 to 59 years, individuals have between 0 and 3 parameters and the only ones who have 4 parameters are in the age range of 40-49 years.
Physical exercise
44'74% goes to work in a motor vehicle and 28'95% go by walk. 47'37% usually have a nap and 84'21% said they do physical exercise to keep fit (33'33%) or because they like (31'75%) mostly. However, an average of 72'81% never or almost never does any of the activities proposed in the survey. The activity remains not usually higher than the activity percentages. Part of their free time use it to watch TV (100%) or connect to the Internet (97'37%) and 73'68% to read. 81'58% work with their computer.
Although there is an increase of moderate physical activity measured in METs in those individuals with two parameters, both light and intense activity will decline as individuals have more cardiovascular risk parameters (graph 2).

Discussion
We have analyzed a pilot sample of 76 individuals, which can serve to describe how the situation of the MS is in the studied group and makes us consider the possibility to go deeper in a further work. However, in an overall assessment, the Results show that the studied population presents many factors related to the MS and therefore have a higher risk for CVD.
According to one of the latest studies carried out in our country about Spanish working population21, the prevalence of the MS is 14'4% for men and 5'5% for women. Our study has shown that 7.89% of the individuals who have participated have MS and we have not obtained any positive result among women, although these differences are related to the limitations of the sample in terms of size and sex distribution. The cases found with MS differ especially from those who do not have an increase in systolic BP and in cholesterol levels, although the prevalence of hypertension and hypercholesterolemia has been lower than in other studies22.
It is important to draw attention to the situation in which there are individuals who, without being officially diagnosed of MS, also present cardiovascular risk factors. These are those who have two high parameters, 31'58% of the participants. Only a slight variation in another parameter is enough to increase their risk for CVD. It is in this group of individuals where there will be a greater need for prevention and health education.
The lipid profile of the participants is obviously high, especially in terms of LDL values, just in males, and their levels are very similar to those of other studies23. Cholesterol levels are also worthy of consideration. This is a fact to evaluate because, even if LDL levels are not used as a parameter to measure MS, individuals with high cardiovascular risk due to this syndrome will further increase their risk by atherogenic LDL abilty13,24.
As for the food, 71'05% says their diet is adequate and the consumption of healthy foods is greater than the unhealthy ones. In addition, only a third of individuals recognize being overweight (31'58%), while the rest think their weight is normal. However, the reality of the data collected confirms that these proportions are practically exchanged, as 36'84% is within normal weight and 52'63% are overweight. Nobody recognized in the survey to have obesity, but 7.89% of them were obese. If we compare these data with those of the National Health Survey 2011-12 (ENSE)25, the prevalence of overweight and obesity (63'2%) is almost the same as that one of this study (60'52%). Therefore, the apparently increased consumption of healthy food regarding the least recommended is not reflected in weight, especially in men, because they have a mean BMI of 27'46. It must be kept in mind that, in the estimation of food consumption, the respondents could not remember what they ate and in some cases, unconsciously, omit the consumption of certain foods (like sweets) or think they eat other foods more than they actually do (such as milk). This is a kind of error, voluntary or involuntary, by the respondent, who can answer what is socially acceptable for him, or in some cases lie26. In addition, in general they eat fast (65'79% in less than 30 minutes) and many do not make the five recommended meals17, indicating that their eating habits are not the most appropriate.
Whatever the causes, the reality indicates that the higher the weight is, the lower intake of healthy food they do, and, the more parameters are in favor of MS, the higher frequency of consumption of not-recommended food, contributing to the weight increasing and raising their analytical values. The ignorance, therefore, of what should be a good diet, is perhaps what makes 71'05% of individuals consider that their diet is adequate.
We observed a significant level of sedentary lifestyle. The association of the sedentary lifestyle with the increase of the MS is known and widely studied 27,28, and the vast majority of participants have limited activity. 81'58% spend long time sitting in a chair and using a computer, use their free time watching television or connecting to Internet and almost the half of them usually nap. If they go to exercise, they choose mostly to walk. Even to go to work, 28'95% said they go by walk, but this fact has a peculiarity in this place, due to the fact that this is a quartering where there are homes within its enclosure, where most of the people stationed there live, so practically all those who come to work by foot just walk 300-400 m., so this fact cannot be considered as physical activity. We also noticed that the higher the risk of CVD is, the less intensity and amount of exercise they do.
There is a significant number of people with overweight and with an insufficient energy expenditure. It is important to ensure that these people get maintain an adequate level of physical activity and good nutrition to achieve an acceptable weight and thus reduce the risk factors for CVD and get a healthier future.
Conclusions
In the group of people we have studied, the research indicates that 7'89% of them have MS, all men; 31'58% has two parameters in diagnosis of MS, in other words, they are future candidates to increase their risk of developing CVD if any of the parameters they have now in a normal range change; more than 60% of men are above the normal weight; the greater the weight is, the highest consumption of unhealthy foods and, in general, they keep a rather low level of activity, which also decreases as they increase the cardiovascular risk factors. All that facts lead us to say that the lack of physical activity and poor nutritional habits act negatively in the lipid profile, BP and BMI of the Guardia Civil staff who participated in the study, which increases the prevalence of MS and, therefore, the risk of CVD.
The limitations of the study in terms of gender distribution must be considered, although this imbalance is inherent in this group, but the Results make us think about the repetition of this study in other quarterings and launch a health education plan aimed to change their exercise habits and eating habits.
Received: September 2, 2015
Accepted: October 2, 2015
References
1. Alimentación saludable y actividad física en la infancia y adolescencia. (Internet) Cantabria: Dirección General de Salud Pública. Gobierno de Cantabria; 2010. (Acceso: 30/08/20125). Disponible en:http://www.saludcantabria.es/uploads/pdf/consejeria/Programa%20Alimentacion.pdf. [ Links ]
2. O.M.S. Obesidad y sobrepeso. (Internet) Nota descriptiva 311. Mayo 2012 (Actualizado 15/01/2015; Acceso 30/08/2015). Disponible en: http://www.who.int/mediacentre/factsheets/fs311/es/index.html. [ Links ]
3. Yanett Palencia M. Alimentación y salud. Claves para una buena alimentación. (Internet) (Acceso: 30/08/2015). Disponible en:http://www.unizar.es/med_naturista/Alimentacion%20y%20Salud.pdf. [ Links ]
4. Moral García J, Redecillas Peiro M, Martínez López E. Hábitos sedentarios de los adolescentes andaluces. J Sport Health Res. 2012;4(1):67-82. [ Links ]
5. Leal E, Aparicio D, Luti Y, Acosta L, Finol F, Rojas E, et al. Actividad física y enfermedad cardiovascular. Revista Latinoamericana de Hipertensión. 2009;4(1). [ Links ]
6. Ainsworth BE, HaskelL WL, Herrmann SD, Meckes N, Bassett DR, Tudor-Locke C, et al. 2011 Compendium of physical activities: a second update of codes and met values. Medicine and science in sports and exercise. 2011;43(8):1575-81. [ Links ]
7. OMS. Estrategia mundial sobre régimen alimentario, actividad física y salud ¿qué se entiende por actividad moderada y actividad vigorosa? who (internet). 2011 (acceso: 30/08/2015). disponible en:http://www.who.int/dietphysicalactivity/physical_activity_intensity/es/index.html. [ Links ]
8. Barrera Chuquiarque DE. Factores de riesgo para enfermedades cardiovasculares según los determinantes de la salud presentes en los choferes de transporte público 2014 (Tesis). Lima-Perú: Universidad Nacional Mayor de San Marcos; 2015. [ Links ]
9. Gallego Gómez AM, Hita Contreras F, Lomas-Vega R, Martínez-Amat A. Estudio comparativo del índice de masa corporal y el equilibrio postural en estudiantes universitarios sanos. Fisioterapia (Internet). 2011 (Acceso 31/08/2015); 33(3):93-7. Disponible en: http://www.elsevier.es/es-revista-fisioterapia-146-articulo-estudio-comparativo-del-indice-masa-90024471. [ Links ]
10. Campillo Alameda FJ, López Ruiz P. La relación entre la obesidad y el ejercicio físico. EFDeportes.com (Internet). 2010 (Acceso 29/08/2015); 150. Disponible en: http://www.efdeportes.com/efd150/la-relacion-entre-la-obesidad-y-el-ejercicio-fisico.htm. [ Links ]
11. Índice de masa corporal. MedlinePlus (Internet). 2010. (Acceso: 31/08/2015). Disponible en: http://www.nlm.nih.gov/medlineplus/spanish/ency/article/007196.htm. [ Links ]
12. Sánchez-Contreras M, Moreno-Gómez G, Marín-Grisales M, García-Ortiz L. Factores de riesgo cardiovascular en poblaciones jóvenes. Rev Salud pública. 2009;11(1):2-11. [ Links ]
13 Síndrome metabólico. Instituto del Corazón de Texas (Texas Heart Institute) (Internet). 2012 (Actualizado 12/2014; Acceso 30/08/2015). Disponible en: http://www.texasheartinstitute.org/HIC/Topics_Esp/Cond/metabolic_sp.cfm. [ Links ]
14. Bello Rodríguez B, Sánchez Cruz G, Campos Ferreira Pinto A, Báez Pérez EG, Fernández Morín J, Achiong Estupiñán F. Síndrome metabólico: un problema de salud con múltiples definiciones. Rev Méd Electrón (internet). 2012 mar-abr (acceso 29/08/2015); 34(2). Disponible en: http://scielo.sld.cu/pdf/rme/v34n2/tema09.pdf. [ Links ]
15. Cabezas G, Lares M, Velasco M, Rodríguez H, Albiarez I, Castro J, et al. Evaluación de marcadores antropométricos, bioquímicos y endoteliales de riesgo cardiovascular en individuos con síndrome metabólico, comparados con grupo control. síndrome cardiometabólico. 2012; II(1):P.6. [ Links ]
16. Fernández Ramos N. Prevalencia y caracterización bioquímica del síndrome metabólico en Canarias (tesis). La Laguna: universidad de La Laguna; 2009. [ Links ]
17. Síndrome Metabólico. CardioSmart (Internet). 2012 (Actualizado 22/05/2012; Acceso 30/08/2015). Disponible en: https://www.cardiosmart.org/healthwise/tm63/39sp/ec/tm6339spec. [ Links ]
18. Villalobos Sánchez C, Mosquera Chacón J, Tovar Cortés H. Prevalencia del síndrome metabólico en consulta de medicina interna. Repert med CIR. 2011;20(2):93-102. [ Links ]
19. Cañón Barroso L, Díaz Herrera N, Calvo Hueros JI, Cruces Muro E, Nieto Hernández T, Buitrago Ramírez F. Incidencia de enfermedad cardiovascular y validez de las tablas de riesgo coronario en pacientes diabéticos con síndrome metabólico. Med Clin (Bar). 2007; 128(14):529-35. [ Links ]
20. Dapcich V, Salvador Castell G, Ribas Barba L, Pérez Rodrigo C, Aranceta Bartrina J, Serra Majem L. Guía de la alimentación saludable. Madrid: Sociedad Española de Nutrición Comunitaria; 2004. [ Links ]
21. López-González ÁA, Angullo Martínez E, Miguel Román Rodríguez M, Vicente-Herrero MT, Tomás Salvá M, Ricci-Cabello I. Prevalencia de factores de riesgo cardiovascular en trabajadores aparentemente sanos. Gaceta Médica de México. 2012;148:430-7. [ Links ]
22. Gomis R, Artola S, Conthe P, Vidal J, Casamor R, Font B. Prevalencia en consultas de diabetes mellitus tipo 2 en pacientes con sobrepeso u obesidad en España. Estudio OBEDIA. Medicina clinica. 2013. [ Links ]
23. Pérez de Isla L, Saltijeral A, Vitale G, González B, Torres A, Álvarez-Sala L. Prevalencia de colesterol LDL inadecuado en pacientes con enfermedad coronaria y/o diabetes mellitus tipo 2. Rev Clin Esp. (Internet). 2012 (Acceso 22/08/2015); 212(10):475-81. Disponible en: http://www.revclinesp.es/es/prevalencia-colesterol-ldl-inadecuado-pacientes/articulo/S0014256512003050/. [ Links ]
24. Giacopini MI. LDL Pequeñas y Densas: Importancia de su Determinación. Tribuna del Investigador. 2010;11(1-2):20-6. [ Links ]
25. Ministerio de Sanidad, Servicios Sociales e Igualdad. Presentación de la encuesta nacional de salud: ense 2011-2012 (internet); 2013. (acceso 30/08/2015). disponible en: http://www.msssi.gob.es/estadEstudios/estadisticas/encuestaNacional/encuestaNac2011/PresentacionENSE2012.pdf. [ Links ]
26. Ferrari MA. Metodología de investigación aplicada a encuestas nutricionales. Estimación de la ingesta de alimentos y/o nutrientes. Buenos Aires: Universidad de Buenos Aires, Escuela de Nutrición, Cátedra de Evaluación Nutricional; 2012. p. 33-44. [ Links ]
27. Wijndaele K, Duvigneaud N, Matton L, Duquet W, Delecluse C, Thomis M, et al. Sedentary behaviour, physical activity and a continuous metabolic syndrome risk score in adults. European Journal of Clinical Nutrition. 2009;63:421-9. [ Links ]
28. Edwardson CL, Gorely T, Davies MJ, Gray LJ, Khunti K, Wilmot EG, et al. Association of Sedentary Behaviour with Metabolic Syndrome: A Meta-Analysis. PLoS ONE. 2012;7(4): e34916. [ Links ]

