










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkEnfermería Global
versão On-line ISSN 1695-6141
Enferm. glob. vol.16 no.45 Murcia Jan. 2017 Epub 14-Dez-2020
https://dx.doi.org/10.6018/eglobal.16.1.232221
Originales
Study on anxiety in intensive care nursing professionals facing the process of death
*Graduate in Nursing. E-mail: celiadtt@telefonica.net
**Bachelor of Nursing. Intensive Care Unit, Burgos University Hospital (HUBU). Spain.
Objective
Death in Intensive Care Units is a process often witnessed by nurses. Nurses are the group that spends more time with the patient and his or her family, and this spatial and temporal proximity leads to intense emotional reactions that, when not treated and channeled appropriately, end up in situations of anxiety and stress. For this reason, we decided to analyze with specific data the anxiety level of professionals facing this reality.
Material and methods
A cross-sectional descriptive study was carried out among ICU nurses in the Complejo Asistencial Universitario of Burgos (CAUB), using Templer's anxiety scale and a questionnaire with socio-demographic variables.
Results
More than 40% of the nurses in the ICU of CAUB showed scores above the values considered as normal anxiety levels. This anxiety is not related to any of the variables studied.
Keywords Anxiety; Death; Nursing
Introduction
In our times, death is no longer considered a necessary natural event, but it is understood as a failure, both in healthcare level and by the rest of society1. The result of this is a feeling of impotence, of not being able to do more to avoid it2.
Death is a process that nurses in Intensive Care Units (ICU) witness frequently. It is commonly accepted that patients hospitalized in ICU have some hopes to survive, but even administering high quality healthcare and modern technology, their situation can change either for the better or for the worse, including here the unavoidable: dying. In clinical practise, when we face the process of death it often emerges a feeling of failure and impotence. We cannot admit that science is unable to avoid this fatal event.
Nurses are the professional group that spends a larger amount of time with the patient and his or her family, and this proximity in space and time results in intense emotional reactions that, when not properly handled and channelled, can eventually lead to manifestations of anxiety and stress.
If we add to this ailment the healthcare stress, it can turn into emotional exhaustion, which may result in estrangement from the patient or identification with his or her problems3, two attitudes that are not correct because both of them may interfere in the good performance of nursing healthcare.
At present we are not trained to reflect about death and we are not educated in how to die4. The human being has the intrinsic need to find not an explanation to death, but a way to adapt to death 5. Most ill persons die in a hospital, and only a few of them know that they are going to die. This results in more stress over nursing professionals because they are usually the ones who have more contact with the patient6. It is very important to know the attitudes of the nursing professional towards death because they interfere in the interpersonal relation and in the healthcare provided to patients and relatives by nurses7). It is necessary for us to study the experience of nurses with more accuracy, in the environment of an ICU.
After a review of the literature related to the subject, we found a study that relates variables such as age, religiosity, occupation personality traits or gender to death anxiety. This research was conducted with people faced to the 'thought' of death1. However, there is a big difference between reflecting about a 'thought' and having to witness and deal with an event such as the end of a patient's life in ICU.
We have found articles about the attitude of nurses in various healthcare services towards death, and the social, environmental and demographic factors that affect this attitude7)(8), All the professionals, no matter in which service they work, are afraid to die9).
There are studies on the perception of the nurse about the death of terminally-ill patients like oncological patients 10)(11).
The perception of the nurse regarding the care administered during the patient's dying process in ICU is positive and this care is considered appropriate, although a significant percentage of the interviewed in the aforementioned study declare that the desires of the patient and his or her family are not taken into consideration, and that they die without the company of their relatives12) (13) (14) (15.
The perception of death in a group of nursing undergraduates was studied introducing training programs for a better response in coping with death16)(17. These programs can be useful for beginners in this profession, but they may not be so useful in more experienced professionals.
There are also studies on the different levels of anxiety among the different health-care professional groups that followed training courses, but it is surprising to see in the results that, after the courses, anxiety reduction was bigger in a group than in other18.
We have not found publications that study further the personal effect on nursing in ICU's.
Our goal is to deepen in the knowledge of what happens to us when a patient dies and to establish the degree of restlessness, fear, dissatisfaction, dread. The more we know about feelings and emotions in this process, the better we can, with emotional support, counteract its negative effects and avoid falling into indifference and identification towards the patient. For this reason, this study was undertaken with the aim of assessing the anxiety degree of nurses in charge of administering care to dying patients in ICU.
Objetives
To determine the death anxiety level in nursing professionals who work in a multipurpose adult ICU.
To examine whether the anxiety level is related to a series of socio-demographic variables.
Material and method
An observational descriptive cross-sectional study was carried out from May to July 2011 in the adults ICU of General Yagüe Hospital in Burgos. The target population under study is the 69 nurses working in that ICU.
In order to determine the death anxiety we used a validated scale: The Death Anxiety Scale (DAS), developed by Templer19 (1970) an adapted into Spanish by Joaquín Tomas Sábado (2002).
It is one of the most commonly used instruments to detect death anxiety and it is the indispensable reference in papers dealing with this topic. It is used as a direct measurement and it measures death anxiety expressed as feelings of fear and thoughts related to the possibility of dying20. This scale consists of 15 items with true or false answers. Every death anxiety indicator counts as one point. 9 items score in the true option and the remaining 6 in the false option. The possible total scores range from zero to 15, where the higher scores correspond to higher death anxiety levels. The foundations that guided its construction are detailed in Templer's works (1970, 1976). Reliability analysis of this scale shows an internal consistency with values that range between 0.76 and 0.87 (Kuder-Richardson Formula 20), and a temporal stability with and interval between 0.71 and 0.8421)(22), All of this allows us to establish that the scale can be used with reliability guarantees. (APPENDIX 1).
A survey with the following socio-demographic variables was also handed:
- Quantitative Variables: age, years of experience as a nurse, years of experience in ICU.
- Qualitative Variables: training received as a professional regarding preparation for death and if this training was appropriate, marital status and the impact of stress in your life. (APPENDIX 2).
Prior to handing the questionnaire, an authorisation from the research committee of the hospital was obtained.
The survey was directly handed to each person and when finished, it was delivered in the post-box of the unit. Along with the questionnaire, an information/consent letter was delivered.
Regarding the ethical aspects, anonymity of interviewees was respected, as well as their free participation in the research, according to current regulations.
For the data analysis, data was processed using IBM SPSS19 statistic software, with a confidence interval of 95 %, after collection and organization of the data with Excel 2010.
A descriptive analysis of the sample was carried out adding means (standard deviation), medians (interquartile range) and frequencies (percentages) according to characteristics and distribution of the variables. The potential relations between anxiety (values measured with the original scale as well as values grouped in a categorial variable that only indicated whether there was anxiety or not) and the different socio-demographic variables were evaluated using the chi-squared test (or Fisher) in the case of qualitative variables and using the T-Student test (only if it verified the application conditions of the test, otherwise the corresponding nonparametric test: Mann-Whitney U test) if one of the variables was quantitative. If both variables were quantitative a correlation (of Spearman because they do not match normality) was carried out.
Results
69 surveys were handed all of them were collected.
After an analysis of the socio-demographic variables we found that all the subjects were women between 21 and 55 years old, with an average age of 35.8. Of them, 37 (53.6%) were single, 30 (43.5%) were married or in a stable relationship, and 2 (2.9%) were separate/widows/divorced.
Regarding their professional profile, they had been working as nurses an average of 12.23 years (SD 9.03: minimum a month, maximum 37 years) and specifically in intensive care an average of 7.32 years (SD 8.32; minimum a month, maximum 32 years).
They were asked about their training in how to cope with death. 14 of the 69 nurses (20%) declared that they had received training whereas 55 (80%) declared that they had not, however 87% answered 'yes' to the question if they believed that the training received on this subject was inadequate.
When they were asked if stress affects easily their daily life, 71% ansewered 'yes'.
One of the objectives in our study was to establish the death anxiety levels in the IC nursing professionals. To measure these levels other studies have proposed Templer's scale as appropriate. Potential scores in this scale range from a minimum of zero points to a maximum of 15 points, where levels between 4.5 and 7 points are considered normal.
In our study scores ranged between a minimum of 3 and a maximum of 12 with an average of 7 (interquartile range: (6-8,50), exactly in the upper limit)
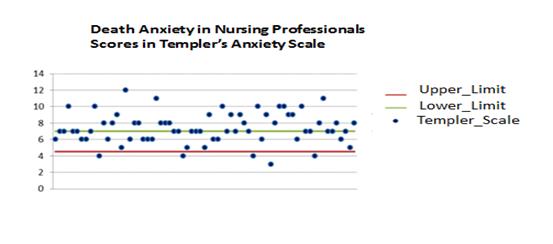
We can state that 42% (29) of the people taking part in the survey are above the upper limit of normal death anxiety levels, whereas only a 7.2% is below the lower limit.
50.8% of the surveyed are in the established limits (scoring between 4.5 and 7). However, more than a half of them scored a value of 7, the upper limit of normal death anxiety according to Templer's scale.
Following with our second objective, to associate anxiety levels with the different socio-demographic variables proposed, we studied the variables age, years of professional experience and years of professional experience in ICU, with the scores obtained in Templer's scale using Spearman Rho correlation, because both of them were quantitative variables. We did not find statistically significant values in any of the cases; therefore, we can state that there is no relationship between these variables.
With respect to marital status and dismissing the category 'others' as it only included two cases, we analyzed the relationship by means of the t-test, and we saw that there is no relationship between marital status and value in Templer's scale (P-value=0.254 greater than p<0.05).
The rest of the variables, influence of stress, specific training in how to cope with death and the belief of being adequately trained were also analyzed with respect to the scoring in Templer's scale using Mann-Whitney U test of independent samples. We did not find in any of the cases a relationship between variables statistically significant (p-value= 0.467; 0.363; 0.469 respectively greater than p<0.05), therefore we kept the null hypothesis.
After analyzing relations between scores in Templer's scale and socio-demographic variables with these statistics, we decided to reconvert the scores obtained into a dichotomous categorical variable:
1) People with a score greater than 7 (8 or more points) that we labelled as 'anxious'
2) People with scores of 7 points or less, that we labelled as 'non-anxious'.
After that we faced them again to the socio-demographic variables checking the relationships with the Mann-Whitney U test for independent samples in the case of numeric variables (age, years as a nurse and years in ICU) and with Chi2) in the case of categorical variables (marital status, influence of stress, specific training and belief of being adequately trained).
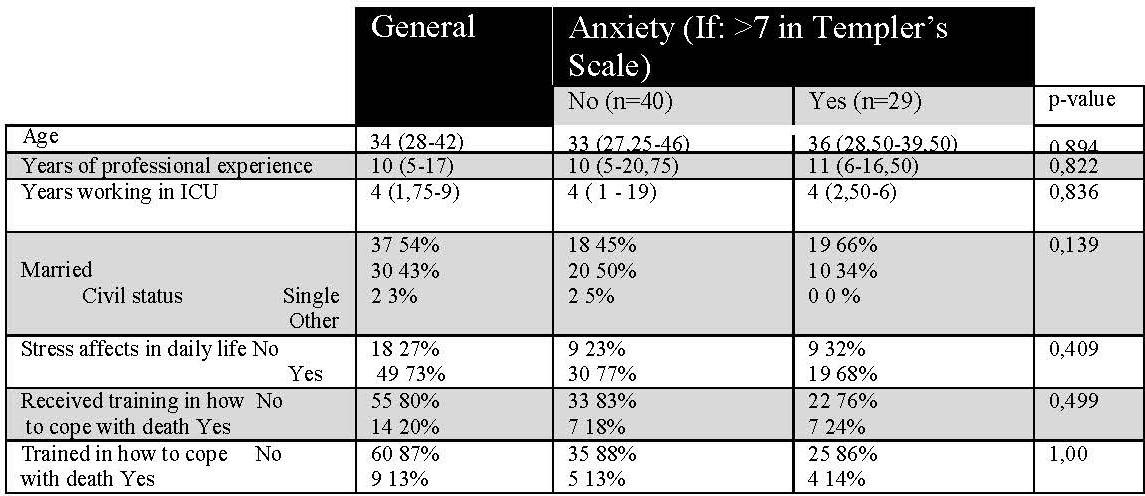
Considering statistically significative the value P<0,05 we observe that there is no relationship between the values obtained in Templer's scale categorized in 'anxious' and 'non-anxious' and the rest of socio-demographic variables included in the study, because p-value is in all cases greater than 0.05. Therefore we can admit that there is no statistically significative relationship between any of the socio-demographic variables and the anxiety produced.
Discussion
1) A very high percentage (42%) of nurses working in ICU in CAUB were above the values considered as normal regarding anxiety felt towards death in their work.
2) Anxiety is not related to age, nor to years in the profession, nor to years working in ICU, and nor to marital status, influence of stress, specific training received or the feeling of being poorly trained. Similar results were obtained by Tomás Sábado J et al1, in one of his studies that analyses the probable influence in the anxiety level of variables such as religion or health, but he did not find significant relationship either.
In contrast to the results obtained in our study, we must mention the study carried out by Lonetto. R and Templer.DI23 in which they indeed found a positive correlation between the demographic variables studied and the anxiety level. It is also worth mentioning the study by Tomás Sábado J8 in which this correlation was also proved but introducing a new variable not studied in our paper, which is the professional category of the health workers.
There is a study18 that suggests that health workers with training in how to cope with death show a lesser degree of anxiety, but in our case the results are similar in people with prior training. However, given the high percentage of nurses without training in this field and the even higher percentage (87%) of nurses that, regardless if they had or had not received training, didn't feel adequately trained, we consider that this fact must make us reflect about the need for quality training in how to cope with death.
3) A high percentage of the total sample (24.6%) is in the upper limit of normal.
ICU professionals show high death anxiety levels that bear no relation to the socio-demographic variables included in this study. The data obtained allow us to confirm the anxiety that nursing professionals show towards the phenomenon of death. Mallet et al24 point out that intensive care nurses show higher death anxiety levels than nurses in other specialities.
After reviewing the study by Lara Olivera KP, et al25) we found that it introduces the analysis of the variable being or not being a healthcare professional, and here they also found differences between the anxiety level in healthcare and non-healthcare subjects. However in the study by Hernández JM. et al 26) death anxiety in healthcare professionals is equivalent in its results to death anxiety in non-healthcare professionals.
After reviewing the results of the aforementioned studies, we can attribute the possible cause of the lack of significant relationship between the analysed variables and the anxiety level in our profession to the fact that those studies have taken into account socio-demographic variables different to those analysed in our study. The addition of those variables may have altered our results.
Conclusion
Nurses in our unit show levels of death anxiety above the limits considered as normal, or they are in the upper limit of 'normal'.
In this research, we have observed a high degree of participation. This can be due to the interest that professionals in these units show in a subject like the death of critically ill patients.
In closing, we would like to add that the research in the role of nursing on this subject makes us aware of our limitations and capacities and of the need for emotional support in professionals working in intensive care units.
REFERENCES
1. Tomás Sábado J, et al. Variables relacionadas con la ansiedad ante la muerte. Rev. de Psicología gral y aplic. 2003; 56(3): 257-279. [ Links ]
2. Uribe Ortiz M.T, et al. La enfermera ante la muerte terminal. Desarrollo Cientif Enferm-Mex. 2006; 14(8):326-329. [ Links ]
3. Colell Brunet R. Análisis de las actitudes ante la muerte y el enfermo al final de la vida en estudiantes de enfermería de Andalucía y Cataluña. Tesis doctoral dirigida por Limonero García J. 2005. [ Links ]
4. Benbunan Bentata B, et al. Afrontamiento del dolor y la muerte en estudiantes de Enfermería: una propuesta de intervención. Int J Clin Health Psychol.2007; 7 (1): 197-205 [ Links ]
5. González Gil, T. Estrategias culturales para el afrontamiento de la muerte infantil en una Unidad de Cuidados Intensivos Pediátricos. Enfermería Intensiva. 2008; 19(3): 113-122 [ Links ]
6. Gala León FJ, et al. Actitudes psicológicas ante la muerte y el duelo. Una revisión conceptual. Cuadernos de Medicina Forense. 2002; 30: 39-50. [ Links ]
7. Maza Cabrera M, et al. Actitud del profesional de enfermería ante la muerte de paciente. Ciencia y Enfermería. 2008; XV (1): 39-48. [ Links ]
8. Tomás Sábado J. La medida de la ansiedad ante la muerte en profesionales de enfermería. Enfermería Científ. 2002: 246-247; 42-47. [ Links ]
9. Alonso Díaz M, et al. Nos asusta la muerte. Enfermería Oncológica. 2006; 9(2): 6-15. [ Links ]
10. Vargas Daza E.R, et al. Percepción de la enfermería en torno a la muerte de pacientes en etapa terminal. Rev Enferm Ins Mex Seguro Soc 2008; 16(1): 37-44. [ Links ]
11. Sousa D, et al. La vivencia del enfermero en el proceso de la muerte y el morir de los pacientes oncológicos. Texto Contexto Enferm. 2009; 18(1): 41-47. [ Links ]
12. Santana Cabrera L, et al. Calidad del morir y de la muerte en una unidad de cuidados intensivos: percepción de la enfermería. Enfermería Clínica. 2008; 18(3): 172. [ Links ]
13. Del Barrio Linares M, et al. Cuidados del paciente al final de la vida: ayudas y obstáculos que perciben las enfermeras de Cuidados Intensivos. Enfermería Intensiva 2007; 18(1): 3-14. [ Links ]
14. Falco Pegueroles A. La enfermera frente a la limitación del tratamiento de soporte vital en las Unidades de Cuidados Intensivos. Aspectos técnicos y prácticos a considerar. Enfermería Intensiva. 2009; 20(3): 104-109. [ Links ]
15. Santana Cabrera L, et al. Percepción de las actitudes éticas de la enfermería de cuidados intensivos ante la limitación del tratamiento. Enfermería Intensiva. 2010; 21(4): 142-149 [ Links ]
16. Bernieri J, et al. La preparación de los estudiantes de enfermería para vivir el proceso muerte-morir. Texto Contexto Enferm. 2007; 16(1): 89-96. [ Links ]
17. Aradilla Herrero A, et al. Efectos de un programa de educación emocional sobre la ansiedad ante la muerte en estudiantes de enfermería. Enfermería Clínica. 2006; 16(6): 321-326. [ Links ]
18. Tomás Sábado J, et al. Ansiedad ante la muerte: efectos de un curso de formación en enfermeras y auxiliares de enfermería. Enfermería Clínica. 2001; 11 (3): 104-109 [ Links ]
19. Templer, D.I. The construction and validation of a Death Anxiety Scale. Journal of General Psycholog. 1970; 82:165-177. [ Links ]
20. Rivera-Ledesma, A, Montero-López Lena, M. Variables con alto valor adaptativo en el desajuste psicológico del adulto mayor.Revista de Conducta, Salud y Temas sociales 2009; 1(may): 59-67 [ Links ]
21. López Castedo A, Calle Santos I. Características psicométricas de la escala de ansiedad ante la muerte en pacientes VIH/ SIDA. Psycotema. 2008; 20(4): 958-963. [ Links ]
22. Rivera-Ledesma, A, Montero-López Lena, M. Propiedades psicométricas de la escala de ansiedad ante la muerte de Templer en sujetos mexicanos. Diversitas Perspective Psicolog. 2010; 6(1): 135-140 [ Links ]
23. Lonetto R,Templer DI. La ansiedad ante la muerte.1988. Ediciones Temis [ Links ]
24. Mallet K, Price JH, Jurs SG, Slenker S. Relationship among burnout, death anxiety and social support in hospice and critical care nurses. Psychol Rep.1992; 68: 1347-1359. [ Links ]
25. Lara Olivera KP, et al. Ansiedad ante la muerte en adultos de población general y personal, que trabaja en el sector de salud. Revista científica electrónica de psicología; 8 [ Links ]
26. Hernández JM, et al. Estudio descriptivo/comparativo entre profesionales sanitarios y no sanitarios sobre la ansiedad ante la muerte. Trab Soc y Sálud-Esp. 2002; 42: 119-149. [ Links ]
APPENDIX I
SOCIO-DEMOGRAPHIC SURVEY
| Age in years | |
| Years of professional experience | |
| Years of professional experience in ICU | |
| Marital status: a) single b) married/stable partner c)Widow/separated/divorced | a b c |
| Do stress situations easily affect your daily life? a) Yes b) No | a b |
| Have you ever received training in how to cope with death? (Courses, conferences, talks...) a) Yes b) No | a b |
| Do you believe you are sufficiently trained in how to cope with death? a) Yes b) No | a b |
APPENDIX 2
TEMPLER DEATH ANXIETY SCALE. TRUE - FALSE
I am very much afraid to die.
The thought of death seldom enters my mind.
It doesn’t make me nervous when people talk about death.
I dread to think about having to have an operation.
I am not at all afraid to die.
I am not particularly afraid of getting cancer.
The thought of death never bothers me.
I am often distressed by the way time flies so very rapidly.
I fear dying a painful death.
The subject of life after death troubles me greatly.
I am really scared of having a heart-attack.
I often think about how short life really is.
I shudder when I hear people talking about a World War III.
The sight of a dead body is horrifying to me.
I feel that the future holds nothing for me to fear.
Received: July 13, 2015; Accepted: September 07, 2015
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
