










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.16 n.46 Murcia Apr. 2017 Epub Apr 01, 2017
https://dx.doi.org/10.6018/eglobal.16.2.248681
Originales
Physical appearance and repercussions on the quality of life and the autonomy of elderly people affected by leprosy
1Nurse. Oncologist and Stomatologist. Federal University of Ceara (UFC)
2PhD in Nursing. Professor at UFC.
3Nurse. PhD in Clinical Care and Health. Professor at the University of International Integration of Afro-Brazilian Lusophony (UNILAB). Redenção (CE)
4Nurse. Specialist in Public Health. PhD in Pathology. Adjunct Professor, Federal University of Maranhão (UFMA). São Luís (MA), Brasil.
Leprosy, coupled with aging process, brings physical changes, which interfere in dependency and autonomy. The objective was to evaluate the physical aspect and the impact on the quality of life and the autonomy of elderly people affected by leprosy. This is a descriptive study of a quantitative approach, conducted with 60 elderly people in two rehabilitation centers in São Luís (MA). We used the Physical Domain of the WHOQOL-Bref and facets "Sensory Skills" and "Autonomy" of WHOQOL-OLD, from the World Health Organization. There were observed problems with pain/discomfort (31.6 percent), fatigue (21.6%) and sleep/rest (23.3 percent), acting in the inability for locomotion (23.3%), carrying out daily activities (16.6%), and work (33.3 percent), as well as related to the dependency on drugs/treatments (56.6%). The quality of life has changed by loss of sensory (33.3%), as well as the ability to perform activities (28.3%) and interact with people (23.3%). Regarding autonomy, most seniors felt free to make decisions (53.3%) and respected by taking them (55.0%), although stated that do not perform all who desire (38.3%). Thus, it was concluded that the disease, before the process of senescence and/or senility, might have contributed negatively about the physical aspects and quality of life of the elderly.
Keywords Aged; Leprosy; Personal Autonomy
INTRODUCTION
Aging is a natural phenomenon, present and universal, which results from the decrease of mortality and fertility rates 1. According to the population census, exists in Brazil, approximately 20 million people aged 60 years old or over, which represents at least 10% of the Brazilian population. The projections statistics from the World Health Organization (WHO), in the period from 1950 to 2025, indicate that the elderly group in the country should have increased in 15 times, while the total population in five, in this way, Brazil occupies the sixth place on the quota of the elderly, reaching, in 2025, approximately 32 million people aged 60 years old or over 2.
Aging is a continuous process that promotes a progressive degeneration of physiological functions, which decreases the organic capacity, enables the development of diseases and culminates with the end of life 1. It is considered a process common to all, even if it varies between one person and another. This process is dependent and influenced by several factors, such as: physical, psychological, social and cultural, which attribute to each person peculiar characteristics 3.
On the other hand, under conditions of workload such as illness, accidents and emotional stress can cause a pathological condition that requires care: senility. Two major errors should be continuously avoided: the first is to consider that all changes that occur with the elderly are due to their natural aging, and the second is to treat natural aging as a disease 4.
While Brazil is undergoing the process of population aging and consequent inversion in the population pyramid, Brazilian society has not yet learned to value the elderly. These already suffer prejudice due to the changes resulting from aging, a situation that is aggravated when the individual is affected by a stigmatizing disease and of pejorative connotation, such as leprosy 5, which causes lesions of the skin and peripheral nerves, forms incapacities and can bring limitations to the life of this individual.
Leprosy is caused by Mycobacterium leprae, or Hansen's bacillus, which is an obligate intracellular parasite, with affinity for cutaneous cells and peripheral nerve cells, which are installed in the body of the infected person in addition to multiply. It has the capacity to infect large numbers of people (high infectivity), even if few become ill (low pathogenicity) 6. It is an infectious disease and of long incubation time. It is considered as a pertinent health problem in most Brazilian states, due to its scale and incapacitating power.
Leprosy manifests itself through dermatological and neurological signs and symptoms that may lead to diagnostic suspicion of the disease. Neurological changes, if not diagnosed and treated appropriately, can cause physical disabilities that may lead to deformities 6, an aggravated condition in aging, which is often followed by other pathologies.
One time diagnosed, leprosy case should be classified operationally. It should be emphasized that the diagnosis of leprosy is clinical-epidemiological. Operative classification is important so that the proper chemotherapy regimen can be selected. This classification is based on the signs and symptoms of the disease in: 1) Paucibacillary (PB): cases with up to 5 skin lesions and 2) Multibacillary (MB): cases with more than 5 skin lesions 7.
There are also the classification of Madrid, in which patients are classified giving the type of response, based on clinical and baciloscopy characteristics, dividing the Hansen's disease into two groups: unstable-indeterminate and dimorphic-stable-tuberculoid and two guys and virchowiana 8.
Relating to the incapacity caused by leprosy, the WHO, in 1961, standardized an instrument to assess them, considering as incapacity only the lesions in the hands, feet and eyes, since they are more severe for daily activities and for simpler diagnosis. Consequently, the incapacitating lesions of these anatomical regions are scaled according to their severity in: level 0 - No problem; level 1 - Decreased or lost sensation in the eyes, hands and / or feet; and level 2 - Eyes: lagophthalmos and / or ectropion, trichiasis, central corneal opacity, visual acuity less than 0.1 - or do not count fingers at 6m distance; Hands: trophic lesions and / or traumatic lesions; Claws; Reabsorption; "Fallen hand"; Feet: trophic and / or traumatic lesions; Claws; Reabsorption; "Fallen foot"; Ankle contracture 6. In consequence, the greater the level of incapacity, the greater the risk of installing deformities, that act in the loss of functional capacity.
Moreover, the biological aging process determines physical changes, such as loss of balance, bone fragility, joint pain, decreased function 9, as well as sensory-perceptual alterations. These changes can lead the elderly to a state of fragility, dependency and often even the loss of autonomy.
Consequently, it is concluded that leprosy is a complex disease, where physical changes certainly influence psychological, social and cultural aspects in these individuals, bringing consequences to their quality of life. This is an image that must be recovered soon, as the number of elderly people has been increasing exponentially in Brazil and leprosy is a serious public health problem in many regions of the country. Faced with this problem, the objective was to evaluate the physical aspect and the consequences on the quality of life and autonomy of the elderly affected by leprosy.
METHODS
This is a descriptive study of a quantitative approach, carried out at the Leprosy Rehabilitation Center attached to the Dr. Genésio Rêgo Health Center building and at the Achilles Lisboa Hospital, originally called “Sanatorium Achilles Lisboa” or, as it was known by the local population, “Colony of Bonfim”, located in the city of São Luís - MA, both in first and second position, respectively, in relation to the care of people affected by leprosy in that State 10.
Data collection was performed from December 2012 to June 2013. The study sample included 60 elderly with leprosy diagnosis. A person aged 60 years old and over, based on the definition of the World Health Organization, was considered elderly 11. It was used as inclusion criterion: elderly, with clinical diagnosis of leprosy and in outpatient treatment, who sought care at the research sites at the moment of data collection. Also as a criterion of exclusion: there were psychiatric, neurological, audiovisual and communication problems that prevented the application of the questionnaire. These problems were identified from the records in the medical record.
For the calculation of the sample there was used the StatCalc program 7 version of titles of Center for Disease Control and Prevention (DCP) in Atlanta, based on 71 cases of Hansen's disease in the elderly (notified in 2012 by the health units of the city of São Luís), 18.1% expected frequency, level of trust equal to 95% and a minimum error of 5%. After the calculation, the sample was fixed in a minimum number of 54 cases.
Initially, the elderly were identified in the book of new cases of leprosy and from this information there was found the designation of date card that contains information about the attendance day of the elderly. That day and after the nursing consultation, individually were clear concerning the goals and methods of participation in the study, and to those who agreed to participate were asked to sign the Free, Prior and Informed Consent (FPIC).
For data collection, an Elderly Identity Card was used, containing the variables: sex, age, race, as well as clinical data, and later the World Health Organization Quality of Life questionnaire (WHOQOL - bref) and World Health Organization Quality of Life - older adults (WHOQOL - OLD), which were completed in a single meeting. For the application of the questionnaires, the instructions of The Whoqol Group 12 were submitted.
The WHOQOL - bref consists of 26 questions, the first two of which refer to the General Index of Quality of Life (GIQL), and the other 24 represent each of the aspects, which are within the following domains: Physical, Psychological, Social Relations and Environment 12.
The WHOQOL - OLD module consists of 24 questions, credited to six aspects: Sensory Functioning, Autonomy, Past Activities, Gifts and Future, Social Participation, Death and Dying, and Intimacy. Each aspect has 4 questions 13. This should be used as a complement to the WHOQOL-bref and is exclusive to the elderly population.
To reach the aims outlined in the study, the Physical Domain of the WHOQOL - bref instrument was analyzed, consisting of the following aspects: “Pain and discomfort”, “Energy and fatigue”, “Sleep and rest”, “Mobility”, “Life activities of everyday life”, “Dependence on medications or treatments” and “Working capacity”, as well as the “Sensorial Function” and “Autonomy” aspects of the WHOQOL - OLD instrument.
The analysis of the identification data was conducted in the EpiInfo program, version 7 of the Atlanta CDC. In the case of descriptive statistics, the results were analyzed in absolute numbers and percentage.
Responses by the WHOQOL - bref and WHOQOL - OLD aspects are obtained by a five - scores Likert scale (1 to 5). These extremes represent 0% and 100%, in that order. For the analysis of the Likert scale, the frequency distribution takes place, where 1 and 2 represent a negative evaluation signaling dissatisfaction (0 to 40%), 3 an intermediate or neutral stance (41% to 60%), 4 and 5 a positive evaluation, indicating satisfaction (61% to 100%). Researchers have developed tools based on the Microsoft Excel software used to carry out the calculation of the scores and descriptive statistics of the WHOQOL-bref and the WHOQOL-OLD 14.
The study was approved by the Research Ethics Committee (REC) of the University Hospital of the Federal University of Maranhão (HUUFMA) under the title “Quality of life of elderly people with leprosy”, for opinion 135.873. After the approval of the REC, the State Department of Health (SDH) of São Luís - MA, authorized the research in the places of data collection.
The ethical observances were contemplated in Resolution N 466/12, which regulates human research in the country, were taken into account, emphasizing the guarantee of confidentiality of the participants’ identity and the absence of any burden for the interviewee. The research did not receive funding for its achievement.
RESULTS
The results revealed that among the 60 elderly affected by leprosy who participated in the study, 53.3% were aged between 60 and 69 years old, which represented the highest percentage studied, followed by 35.0% of elderly between 70 and 79, 10.0% between 80 and 89 and only one elderly over the age of 90 years old (1.6%). In the middle of them, a higher frequency of male (58.3%) compared to female (41.6%). Most were found of race/color brown (66.6%); however, the white (26.6%) and black (6.6%) were also present.
Concerning operational classification, there was an almost total multibacillary frequency (95.0%) in relation to the paucibacillary (5.0%). Moreover, the prevalence of Dimorph (60.0%) and Virchowiana (25.0%) was observed; no elderly individuals were found to be undetermined and only 3.3% had tuberculoid forms, which were considered the initial forms of the disease.
Regarding the disabilities caused by leprosy, level 1 was found to be prevalent (45.0%), followed by level 0 (28.0%) and level 2 (17.0%). There was a higher frequency of multidrug / multibacillary therapy (MDT / MB) with 12 doses (93.0%) compared to the multidrug / paucibacillary (MDT / PB) group with 6 doses (5.0%), considering that the majority of the elderly in this study were classified as multibacillary, with only one elderly being observed using the alternative scheme (2.0%).
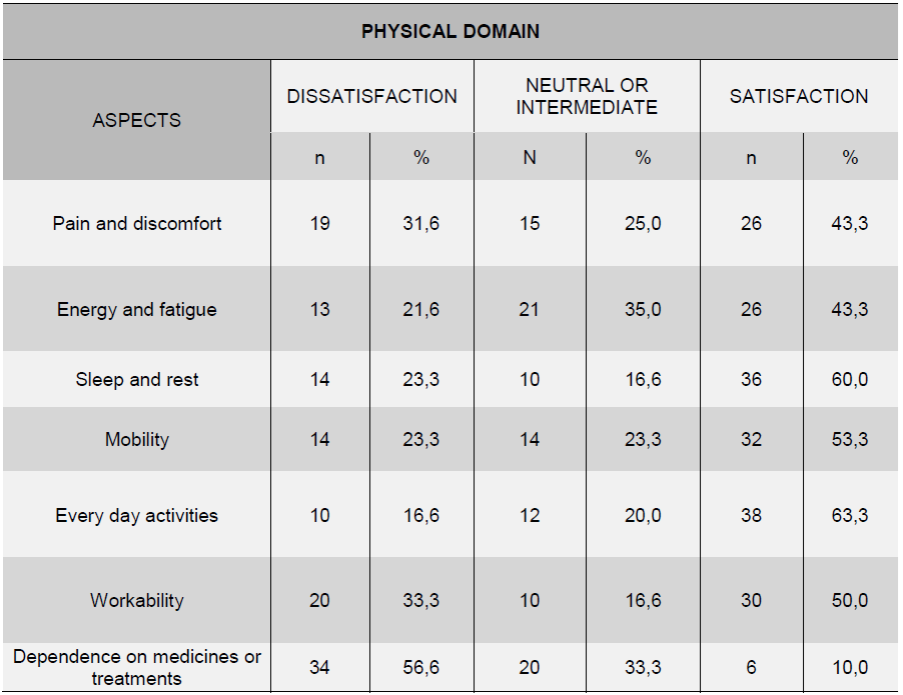
The analysis of the Physical Domain “quality of life” of the WHOQOL-bref indicated average score for quality of life of 55.6%, representing a “neutral or intermediate”. When the elderly were evaluated about how much physical pain and discomfort prevented them to do what they needed, a level of satisfaction of most of them (43.3%), even if dissatisfaction has been referred to by a high number of elderly (31.6%). When asked if they had enough energy for daily activities, most demonstrated satisfaction (43.3%); however, there was also dissatisfaction (21.6%) and a large percentage with a neutral posture (35.0%). When evaluated, the majority showed satisfaction (60.0%); however some people were dissatisfied (23.3%) with their sleep.
About their locomotion capacity, the majority of the elderly were satisfied (53.3%), but some differed, responding in a neutral way (23.3%) or unsatisfied (23.3%) with mobility. Regarding the ability to perform daily activities, the majority of the elderly were satisfied (63.3%); however, some showed neutral (20.0%) and even dissatisfied (16, 6%). In terms of capacity for work, those who considered themselves satisfied (50.0%) with this capacity predominated among the elderly; however, there were also very dissatisfied (33.3%).
On the subject of the need for some medical treatment that the elderly should do to lead their daily lives, a large part said that they need enough, which leaves them in a state of dissatisfaction (56.6%) in relation to this dimension of their lives, getting the highest index of dissatisfaction in the Physical Domain (Table 1).
Table 1 Distribution of the answers of the elderly affected by leprosy, according to aspects of the Physical Domain of the WHOQOL-bref. São Luís - MA, 2013
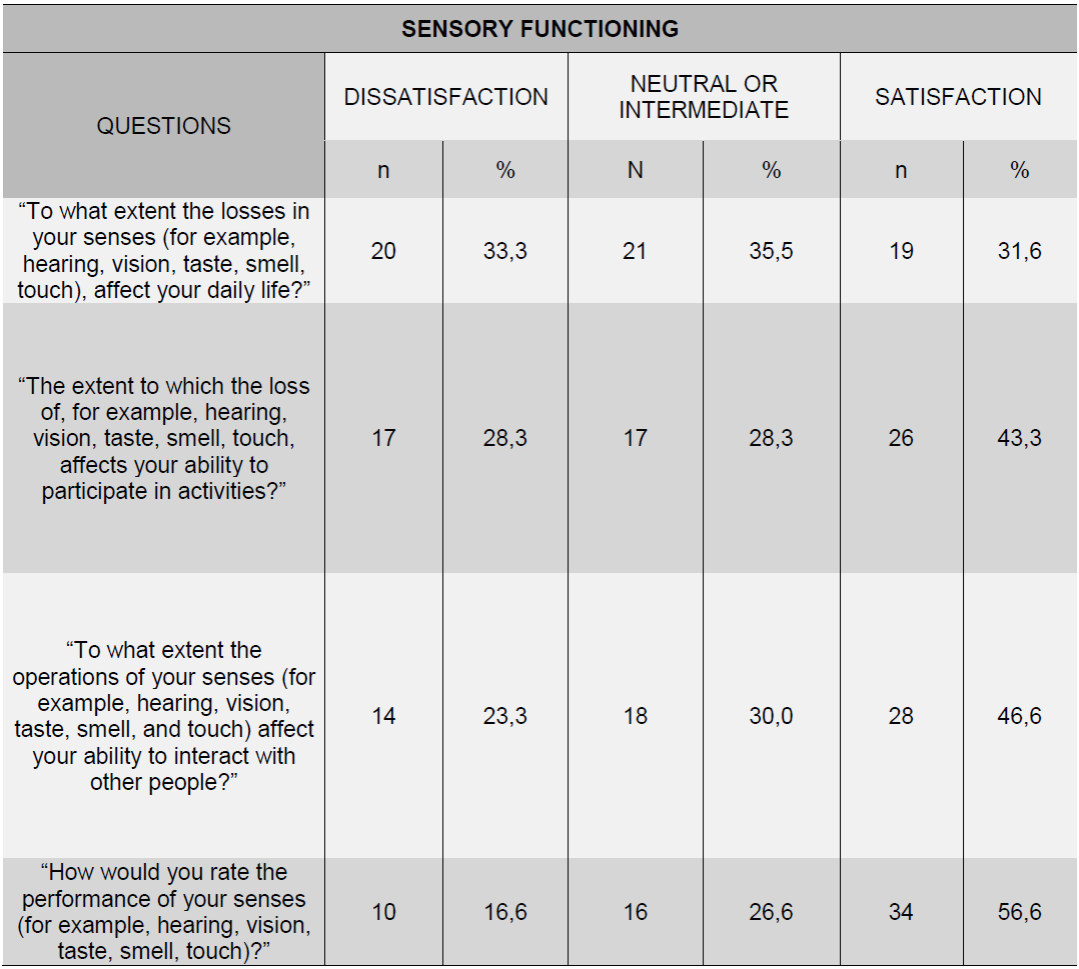
The analysis of the Sensory Function Aspect of the WHOQOL - OLD instrument showed an average score of 58.8%, what demonstrates a neutral or intermediate position in relation to this parameter. The results revealed that the most of the elderly also had a neutral attitude (35.5%) regarding the loss of their senses (eg hearing, vision, taste, smell, touch) affecting their daily lives, with a considerable number of dissatisfied elderly (33.3%).
On the other hand, many participants reported satisfaction with their ability to participate in activities (43.3%) and in interaction with people (46.6%), even though the level of dissatisfaction observed in these two variables could not be neglected (28.3% and 23.3%, respectively). Nevertheless, in the last item, in which the elderly evaluate the functioning of their senses, the most showed satisfaction (56.6%) (Table 2).
Table 2 Distribution of the answers of the elderly affected by leprosy, according to questions about Sensory Functioning of WHOQOL-OLD. São Luís - MA, 2013.
In the evaluation of the Aspect Autonomy, there was found an average score of 53.8%. The first two questions investigated how much the elderly person was free to make his own decisions and how much the people around him respected this freedom, being observed that the majority was satisfied, with 53.3% and 55.0%, respectively.
On the topic of the extent to which the elderly thought they controlled their future, most answered that they controlled more or less, thus presenting a neutral posture (48.3%) in this parameter of their lives. Also, when asked if they do everything they would like to do, most said they were dissatisfied (38.3%) (Table 3).

DISCUSSION
It is known that leprosy is manifested, besides to skin lesions, through peripheral nerve lesions 7. These lesions are caused by inflammation of the peripheral nerves, what causes pain. Such involvement manifests itself through an acute process, followed by severe pain and swelling. There is also the type for leprosy Reactions 1 and 2, which can arise during and/or after curing of the sick, and that between the signs and symptoms include pain. The pain, regarded as the fifth vital sign, interfered in 31.6% quality of life of older people affected by leprosy. Higher percentage was found in a study on the life quality of patients with leprosy reactional states, which noted that the pain stopped “very” and “extremely” the majority of patients (50%) to fulfill their usual activities 15.
In this study, there were also observed the existence of 21.6% of elderly dissatisfied with energy for their day-to-day; they were found to be fatigued. Unlike energy, fatigue is conceptualized as a “self-recognized state in which an individual experiences a sustained and overwhelming feeling of exhaustion and reduced physical and mental effort”. It is different from tiredness, which is a “temporary, transitory state caused by lack of sleep, improper nutrition, sedentary lifestyle, etc.” 16. This lack of energy is a symptom caused by many situations, diseases, treatments, etc., such as leprosy.
There was also 23.3% dissatisfaction with sleep. In a study with elderly community members, 49.9% of the study population complained of one or more symptoms of insomnia 17. Changes in the sleep associated with aging may correspond to sleep disturbances or impairment of sleep quality. Among them, we focus: Quantitative reduction of the stages of deep sleep; Reduction of the verge for awakening due to noise, associated to the quantitative increase of superficial sleep; Greater latency to the beginning of sleep; Increased naps during the day; Reduction of total nighttime sleep duration; Greater number of transitions from one stage to another and to wakefulness; Greater frequency of respiratory disorders during sleep 18.
There is still that the majority of elderly with level 1 and 2 of physical disability in this study (45% and 17.0%, respectively), and that most of them presented the clinical forms Dimorph (60.0%) and Virchowiana ( 25.0%), which are the most advanced, extremely contagious and with great disabling potential. These factors may be contributing to impairment in their mobility, given that 23.3% of the elderly were dissatisfied with mobility.
Regarding everyday activities, it was observed that only 16.6% of elderly people affected by leprosy were dissatisfied with the performance of everyday activities, but the dissatisfaction index increased to 33.3% when capacity. Researchers report that 50% of reactive patients in leprosy are dissatisfied with their ability to work, and leprosy is still responsible for decreasing the workforce and increasing the isolation of social life and community participation due to their incapacitating potential, keeping alive the stigma of the disease and compromising quality of life 15.
Relating to the use of medicines, the elderly represent, perhaps, the age group most medicalized in society 19. In this study, the multidrug therapy (MDT) for the treatment of leprosy was mentioned, as well as medications for Suppression of reactional frames, hypertension, diabetes, arthritis, etc. Therefore, reliance on medicines or treatments was cited by 56.6% among seniors affected by leprosy. It is valid to mention that any medication can introduce side effects. Those used in MDT and treatment of reactional states can also cause those effects, which can be liver, gastrointestinal, cutaneous, hemolytic, etc 7.
The scores of life quality of the Physical Domain presented an average score of 55.6%, differing from a study carried out in Taiwan with community-dwelling elderly leprosy patients, which showed an average of 60.01, increasing to 69.35 after intervention with physical activity 20.
It is important to note that the change in sensory functioning was also stated as a reason for dissatisfaction. Depending on the level of disability, there may be a decrease or loss of sensation in the eyes, hands and / or feet, to severe conditions such as corneal opacity, resorption, hand and foot loss, etc. In a study with 107 leprosy patients, it was observed that patients with a higher level of disability caused by the disease had a greater loss in the level of life quality; and that the incapacity was still directly proportional to the prejudice suffered, being greater the greater the level of affection 21. This may have led to a considerable number of elderly people to declare that the loss of their senses affected their daily lives (33.3%), as well as their ability to participate in activities (28.3%) and interaction with other people (23.3%).
In this sense, the discussion about the autonomy of the elderly is relatable, in the meantime it is very frequent to observe that, in the life of situations of dependence, and the autonomy of the elderly tends not to be taken into account. In this study, however, many said they were able to make their own decisions (53.3%) and that people around them respected their freedom (55.0%). It is cost mentioning that most of the elderly in this research were between 60 and 69 years old (53.3%), some still not retired, which leads them to occupy themselves in some way and feel more independent.
Despite this, the quality of life scores in the autonomy (53.8%) and sensory functioning (58.8%) factors obtained in the leprosy-affected elderly group were lower when compared to the values in another study performed with elderly registered in a Unit of Basic Attention, participants of a health promotion group, who presented an average score of 58.4% in the autonomy aspect and 70.0% in the sensory functioning 22.
This condition is reinforced by the large percentage of elderly people who are dissatisfied with what they would like to do and do not (38.3%), which may be a consequence of dependence of any kind - physical, financial, transportation, etc., or by simply losing the autonomy brought about by aging. It is understood that the ability to make decisions and that of self-government can be compromised by physical and mental illnesses or by economic and educational limitations 4.
Dependence is one of the situations that most alarm the elderly, negatively affecting their quality of life by bringing costs to their autonomy as a human being. In a study with institutionalized elderly people, regarding sequelae due to leprosy, the authors found that the elderly feel stigmatized in relation to leprosy, but mostly in relation to their aging. Thus, it can be concluded that this condition would affect their quality of life5.
Evaluative studies about quality of life in the elderly in various clinical conditions and, especially, about leprosy are important to subsidize educational actions aimed at optimizing their quality of life and changing their perception to aging. However, there is still fragility in the use of studies to direct interventions.
CONCLUSION
It was observed that the elderly through the process of aging and affected by leprosy, in this study, were affected intensely by the clinical forms most incapacitating of leprosy - unclear lepromatous and -, and with levels more severe than physical disabilities - levels 1 and 2. All these attached with the process of senescence and/or senility, may have contributed negatively on the physical aspects of those elderly.
It is obvious also, problems with pain/discomfort, fatigue and sleep/rest, which acts including the inability of some to be around, or even perform daily activities and, mainly, at work, as well as issues related to the dependence of drugs/treatments.
A considerable number of elderly people have experienced interference in their daily lives, their ability to perform activities and interact with people, possibly due to sensory losses. This analysis becomes essential to understand why most of the elderly, while having the freedom to make decisions and be respected for taking them, stated that they did not accomplish everything they wanted. It seems to be erroneously acceptable that, since they are not partially or wholly capable of performing an action (in physical terms), they are also unable to decide on it, which translates into lack of autonomy and may lead to a decrease in their quality of life.
REFERENCIAS
1. Zenevicz IL, Moriguchi Y, Madureira VSF. A religiosidade no processo de viver envelhecendo. Rev esc enferm USP. 2013; 47(2): 433-9. [ Links ]
2. Ministério da Saúde [Internet]. Atenção à Saúde da Pessoa Idosa e Envelhecimento. Brasília; 2010 [cited 2014 Jun 14]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/atencao_saude_pessoa_idosa_envelhecimento_v12.pdf [ Links ]
3. Degani GD. Trauma em idosos: características e evolução [dissertação]. Ribeirão Preto: Escola de Enfermagem de Ribeirão Preto, Universidade de São Paulo; 2011 [cited 2014 Jun 5]. Available from: http://www.teses.usp.br/teses/disponiveis/22/22132/tde-28112011-164940/en.php [ Links ]
4. Ministério da Saúde [Internet]. Envelhecimento e saúde da pessoa idosa. Cadernos de Atenção Básica, n.º19. Brasília: Secretaria de Atenção à Saúde, Departamento de Atenção Básica; 2006 [cited 2014 Jun 6]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/abcad19.pdf [ Links ]
5. Souza JFM, Sena TCCB. O envelhecer institucionalizado de sujeitos sequelados pela Hanseníase da U/E Abrigo João Paulo II. Revista Kairós Gerontol [Internet]. 2014 [cited 2015 Mar 09]; 17(1):103-23. Available from: http://revistas.pucsp.br/index.php/kairos/article/view/19879 [ Links ]
6. Ministério da Saúde [Internet]. Guia de Vigilância em Saúde.1ª ed. Brasília: Secretaria de Vigilância em Saúde; 2014 [cited 2016 Jan 12]. Available from: http://portalsaude.saude.gov.br/images/pdf/2014/novembro/27/guia-vigilancia-saude-linkado-27-11-14.pdf [ Links ]
7. Ministério da Saúde [Internet]. Gabinete do Ministro. Portaria no 3.125, de 7 de outubro de 2010. Aprova as diretrizes para vigilância, atenção e controle da hanseníase. 2010 [cited 2015 Feb 20]. Available from: http://portal.saude.gov.br/portal/arquivos/pdf/portaria_n_3125_hanseniase_2010.pdf. [ Links ]
8. Lastória JC, Abreu MAMM. Hanseníase: diagnóstico e tratamento. Diagn Tratamento [Internet]. 2012 [cited 2015 Mar 09]; 17(4):173-9. Available from: http://files.bvs.br/upload/S/1413-9979/2012/v17n4/a3329.pdf [ Links ]
9. Pedrinelli A, Garcez-leme LE, Nobre RSA. O efeito da atividade física no aparelho locomotor do idoso. Rev Bras Ortop [Internet]. 2009 [cited 2014 Jul 5]; 44 (2):96-101. Available from: http://www.scielo.br/pdf/rbort/v44n2/a02v44n2.pdf [ Links ]
10. Secretaria de Estado da Saúde. Casos de Hanseníase do Município de São Luís por Faixa Etária em 2012. São Luís: SINANNET/TABWIN; 2012. [ Links ]
11. Organização Mundial da Saúde. Guia global: Cidade amiga do idoso. Genebra: World Health Organization [Internet]. 2008 [cited 2013 Nov 04]. Available from: http://www.who.int/ageing/GuiaAFCPortuguese.pdf. [ Links ]
12. The Whoqol Group. Development of the Word Health Organization WHOQOL - bref. Quality of Life Assesment. Psychol Med. 1998; 28 (3):551-8. [ Links ]
13. Fleck MPA, Chachamomovich E, Trentini C. Projeto WHOQOL - OLD: método e resultados de grupos focais no Brasil. Rev Saúde Pública [Internet]. 2003 [cited 2014 Jun 8]; 37(6):793-9. Available from: http://www.scielo.br/pdf/rsp/v37n6/18024.pdf [ Links ]
14. Pedroso B, Pilatti LA, Gutierrez GL, Picinin CT. Cálculo dos escores e estatística descritiva do WHOQOL-bref utilizando o Microsoft Excel. Rev Bras Qual Vida [Internet]. 2010 [cited 2014 Jun 15]; 2(1):31-6. Available from: http://revistas.utfpr.edu.br/pg/index.php/rbqv/article/view/687/505 [ Links ]
15. Costa MD, Terra FS, Costa RD, Lyon S, Costa AMDD, Antunes CMF. Avaliação da qualidade de vida de pacientes com estados reacionais da hanseníase atendidos em um centro de referência dermatologia. An Bras Dermatol. 2012; 87(1):26-35. [ Links ]
16. Carpenito-Moyet LJ. Manual de diagnósticos de enfermagem. 13 ed. Porto Alegre: Artmed; 2011. [ Links ]
17. Pereira AA, Ceolim MF, Neri AL. Associação entre sintomas de insônia, cochilo diurno e quedas em idosos da comunidade. Cad Saúde Pública [Internet]. 2013 [cited 2014 Jul 7]; 29 (3) :535-46. Available from: http://www.scielo.br/pdf/csp/v29n3/a11v29n3.pdf [ Links ]
18. Costa SV, Ceolim MF, Neri AL. Problemas de sono e suporte social: estudo multicêntrico fragilidade em idosos Brasileiros. Rev Latino Am Enferm [Internet]. 2011 [cited 2014 Jun 5]; 19 (4):920-7. Available from: http://www.scielo.br/pdf/rlae/v19n4/pt_10.pdf [ Links ]
19. Balduino E, Jacopetti SR. Levantamento da qualidade de vida de um grupo de idosos. Boletim de Enfermagem. 2009; 2 (5):31-47. [ Links ]
20. Cheng SP, Wang TF, Tang FI, Chu NK, Chen IJ. The influence of high-rise residence on physical activity and quality of life among older people with leprosy in a retirement community. Ageing and Society [Internet]. 2014 [cited 2016 Jan 15]; 34(1):90-105. Available from: http://dx.doi.org/10.1017/S0144686X12000840 [ Links ]
21. Lustosa AA, Nogueira LT, Pedrosa JIS, Teles JBM, Campelo V. The impact of leprosy on health-related quality of life. Rev Soc Bras Med Trop [Internet]. 2011 [cited 2014 Jun 10]; 44(5):621-6. Available from: http://www.scielo.br/pdf/rsbmt/v44n5/19.pdf [ Links ]
22. Santos LF, Oliveira LMAC, Barbosa MA, Nunes DP, Brasil VV. Calidad de vida de los mayores que participan en el grupo de promoción de la salud. Enfermería Global [Internet]. 2015 [cited 2016 Jan 19];14(4):1-11. Available from: http://revistas.um.es/eglobal/article/view/201431/181371 [ Links ]
Received: January 22, 2016; Accepted: March 26, 2016
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
