










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.16 no.47 Murcia jul. 2017 Epub 01-Jul-2017
https://dx.doi.org/10.6018/eglobal.16.3.256641
Originales
Study of job satisfaction in primary healthcare in an area of Asturias
1Family and Community specialist Nurse, El Coto Health Center, Area V, SESPA. Asturias. Spain.
2Family and Community Specialist Nurse, "Contrueces" Health Center, Area V, SESPA. Asturias. Spain.
3Doctor of Admission and Clinical Documentation, Central University Hospital of Asturias, SESPA. Astuirias. Spain.
Objective
Evaluate the level of job satisfaction of professionals working in Primary healthcare in Asturias and associated factors.
Methodology
Cross-sectional descriptive study.Study Population: professionals of any category working at Health Centers in the province of V (Asturias). Sample: Whole population. We used the validated Red Font AP “Roja Font” questionnaire and gathered it up with variables socio-demographic and work variables. The quantitative variables are described with average and standard deviation, the qualitative with frequency distribution percentage. Possible relationships are sought between job satisfaction and the remaining variables using chi-square, t-Student and ANOVA.
Results
Response rate: 57.22% (329 out of 575). 72.3% women. Average age: 50.8 years (From: 10.09). 83.9% self-reported as satisfied (95% CI: 83.5-91.2). Only 62.6% (95% CI: 57.4-68.2) were satisfied by calculating the Global Average Satisfaction (GAS) derived from “Font-Roja”. Dimensions of the “Font-Roja” with greater satisfaction: "relationship with coworkers" and "professional competence”. Lower satisfaction: "professional promotion" and "work-related tension". All the categories gave low score to the salary, being the worse administrative and hospital attendant (p <0,001). In the bivariate analysis between GAS and socio-demographic variables, there was a statistically significant association with teaching, 68.8% satisfied in the educational centers (p .039) and with professional category, remaining the most satisfied being MIR / EIR 88.9% and the least were doctors with 46.1% (w: 0.009).
Conclusions
The majority of professionals are satisfied occupationally. They present a higher self-reported satisfaction than that derived from the GAS measurement in Font-Roja.Areas of improvement: wages, professional promotion and development and tension at work.
Keywords: Job satisfaction; Primary health care; Health personnel
INTRODUCTION
The Work plays a prominent role in the life of human being. Most people spend a third of the day working, they do it during the middle of their life. However, it was not until the twentieth century when the work began to be studied from the scientific point of view, relating this issue to different aspects.
Frank Taylor, in 1911, assumed that job satisfaction was totally related to the salary received, which mean, with the rewards. Later, in the 1930s, industrial studies began to give importance to worker welfare. Happock considered that job satisfaction form a part of general satisfaction in life and was related to the individual's ability to adapt to situations and communicate with others, with the socioeconomic level and with the person's preparation for that type of work.1
In 1945, Elton Mayo asserted that the individual's interaction with the group was the most important determinant of job satisfaction and placed it above other factors that also influenced satisfaction. Such as safety, esteem, affiliation, intrinsic interest in work, achievements, etc. This study was the first that realized from a psychological perspective.2
The theories of motivation have been supposed another important influence in studies of job satisfaction. The humanist psychologist Maslow developed a hierarchy of human needs in 1954, placing in the most basic, needs that are vital to survive and in the highest place those which allow the intellectual development of the person. Based on this theory, satisfaction has been focused by researchers, mostly from the perspective of a need for personal fulfillment.3
Herzberg developed a theory of job satisfaction based on Maslow's hierarchy, in which he concluded that not all factors influence satisfaction. Corresponding to the most basic needs count if they are not covered, while other higher factors increase satisfaction in achieving them. This theory of hygiene and motivation has prevailed in studies of nature job satisfaction and has formed the basics of the development of the assessment of satisfaction.4
In 1976, Locke defined Job Satisfaction as "a positive or pleasurable emotional state of the subjective perception of the employee's work experiences." It would be an affective orientation what an employee has towards his work. Which could be considered as a global feeling about work, or a grouping of attitudes related to various aspects of work. In brief, it could be said that a person is satisfied with his work when he is comfortable with it, having a positive attitude towards the work and the conditions in which it is realized. (5
Professional satisfaction constitutes is the first indicator of working life quality, and, as we have already seen, there are multiplicities of variables that may affect it. Regardly to the health field, analyzing the future of health care in our society, we observe a constant evolution of scientific knowledge, technical means, the health system itself, a modification of the epidemiological patterns, as well as an evolution of the pyramid of Population and the needs demanded by the citizens of the National Health System. All this, converges in the appearance of a new and complex model of care that has to give an effective and safe answer to the needs of our citizens.6
In Sanitary organizations, the human factor plays a fundamental role for the concession with "quality" of these services, since unlike other organizations; these are tightly related to the personal treatment. Several studies showed up that for users, quality is represented and defined by the characteristics of the care process, where the main factor of the process is the personal treatment that is offered.7)(8
The satisfaction of the client or user requires the commitment of the staff and it is considered that "employee satisfaction influences the customer's" (to greater job satisfaction, greater perception of user quality), recognizing that an internal atmosphere of quality Creates an environment leads to satisfy external clients or users in terms of high intervention effectiveness, suitable use of technique and technology, and interpersonal relationship with human warmth.9
Sanitary professionals, therefore, have been a well-studied group on satisfaction issues. They are considered to be particularly stressful professions because they have high levels of responsibility, interpersonal relationships and social demands, which affect personal health and well-being as well as job and collective satisfaction.10
Given that job satisfaction of sanitary professionals is one of the indicators that condition the quality of care assistance, the routine measurement of job satisfaction and the design of improvement actions to correct those aspects with worse results should be a mandatory practice for any management team.6)(11)(12
Professional job satisfaction can be equal in its importance to the scientific-technical preparation, that they own or to have at their disposal a certain technology.13
The implementation of a total quality model, therefore, requires knowledge of workers' satisfaction.14
Several research studies reveal that the satisfaction of sanitary professionals is tightly related to the level of autonomy, working conditions, respect and recognition of the work being done, adequate and sufficient staffing, good relationships among team members, Salary, commitment to the organization and professional involvement. Aspects all closely related to the style and management model established by the organization's directors.15
In our country there have been several investigations, respect to environment of the workers of the Health Services. In the area of Primary Care we can find two works done in the Community of Madrid.16), (17
In which they analyzed the personnel of all the categories that work in the Health Centers: Physicians, Nursing, other sanitary professions (Physiotherapists, Midwives, etc.) and administrative personnel too. In 2013 an investigation was carried out in Asturias that studied professionals from several professional categories, Primary care as well as Specialized Care who were developing their work in Clinical Management Units.18
Other studies studied the satisfaction of only one particular professional category, such as work carried out in Asturias19, Málaga20 or Barcelona21, which were limited to the medical staff, or others performed by some colleagues in Galicia 22 and in Soria 23 who were dedicated to nursing staff.
Our intention in the present work was to evaluate and analyze the whole set of workers of the Health Centers, so we include medical and nursing staff, other sanitary professions and administrative personnel. The Health Service of the Principality of Asturias (SESPA) is divided geographically into eight health areas and our work was carried out in the Health Area V (Gijón).The general objective of our work was to evaluate the level of job satisfaction of the different professionals working in Primary Care in Area V. As specific objectives we sought to know the socio-demographic characteristics of Primary Care workers in Area V and to analyze the aspects that they have Greater influence on job satisfaction.
MATERIAL AND METHOD
Design: Cross-sectional descriptive study.
Scope: Primary Care of Area V (Gijón) of the Health Service of the Principality of Asturias.
Population of study: Professionals of all categories (sanitary and non-sanitary) who carry out their work in the health centers of Area V.
Criteria for exclusion: A) Personnel who have worked less than 6 months in primary care at the time of data collection.B) Personnel who are in situations of work incapacity, vacations, etc. during the period of data collection.No sample is performed; the questionnaire is passed to all professionals.
Time of the study: September 15 to November 31, 2014.
Information sources: Self-elaborated questionnaire was for the collection of socio-demographic variables and questionnaire of Font Roja AP to evaluate job satisfaction. The questionnaire is anonymous and self-administered in private. The deliveries and collection was done through the Coordinators of the Centers. The questionnaires were deposited in an opaque box located in the Administrative Unit of the Health Center. Participation was voluntary. Prior to the consultation, authorization was requested in writing to the Nursing Management and Direction of the sanitary, providing a copy of our questionnaire.
Variables collected in a questionnaire of own elaboration: Socio-demographic variables: sex, age, marital status, number of children. Work variables: health center, type of contract, time worked in primary care and in the health center, average number of patients attended per day. Variables on job satisfaction: "Self-declared satisfaction" by introducing a direct question formulated as follows: "In general, are you satisfied with the work you do?” with valid option yes / no.
“Font-Roja” Questionnaire: This validated questionnaire, which determines the satisfaction of professionals in hospital centers, was adapted to the working conditions of Primary Care, being renamed “Font Roja AP” questionnaire by J. Aranaz 24.It consists of 24 items and explores 9 dimensions that determine the professionals’ satisfaction. Each of the items is valued using a Likert scale, whose values range from 1 (totally disagree) to 5 (totally agree). There are items with higher scores indicating greater satisfaction (7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17 and 19), and others with a higher score indicate lower satisfaction , 3, 4, 5, 6, 18, 20, 21, 22, 23 and 24).
The overall result of this questionnaire is expressed in an index called Global Average Satisfaction (GAS), which results from calculating the difference between the items of the Red Font Questionnaire that are part of the dimensions that increase satisfaction less those belonging to those that decrease it, then dividing the result by the total of 24 items. From this calculation results in a score ranging from -2 to 2 points, allowing people to be differentiated into satisfied (> 0), indifferent or neutral (= 0) or unsatisfied (<0). The GAS is constituted as the work-dependent variable.
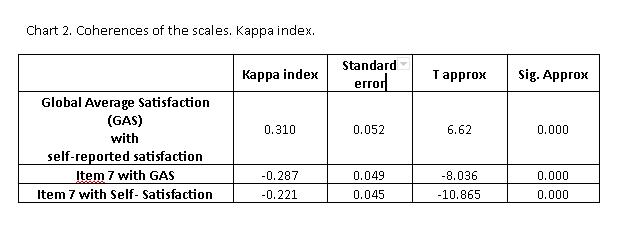
Statistic analysis: The sample is described using the mean and standard deviation for the quantitative variables and the qualitative variables the percentage distribution of frequencies. A first analysis was carried out to verify the degree of agreement between the different ways of measuring satisfaction (Global Average Satisfaction, item number 7 of the questionnaire and self-reported satisfaction by the professional) using the Kappa Index.
A univariate analysis was conducted looking for the influence of the independent variables on job satisfaction (Result of “ Roja Font AP” Questionnaire (GAS) with Chi-square test for qualitative variables and Student's test, ANOVA or other non-parametric tests for quantitative variables.
To verify that variables are independently associated with the job satisfaction variable (GAS), a binary logistic regression analysis was performed (method of introducing); The variables selected for the model were those that in the univariate analysis reached a statistical significance of p <0.2. 5% is defined as level of statistical significance. The 95% confidence intervals of the most relevant results are presented. The analysis was performed with the statistical package SPSS v.15.0.
RESULTS
Descriptive analysis of participants group
The survey was distributed among all the professionals of the Primary Care teams, a total of 575 people in the study period. The response rate was 57.22%.
-
Socio-demographic variables
They were mostly women (72.3%), average age 50.8 years and 64.4% were married or had a stable partner. The majority have children (65.3%).

-
Work variables
They were mostly women (72.3%), average age 50.8 years and 64.4% were married or had a stable partner. The majority have children (65.3%).
The majority were fixed statutory staff (69.6%). They have had an average of 25 years working, of which 17.3 years have exercised in Primary Care.
The average pressure on healthcare (patients treated per day) is 50.42. There is a great variability in the number of patients / day among the different professional categories, thus the medical assistance pressure is 37.53, compared to 21.85 for nurses, 29.83 for MIR / EIR and 205.45 for administrative staff.
Variability also exists within each category, so we see that patients attended daily by a doctor range from a minimum of 10 to a maximum of 70, and those attended by nursing range from a minimum of 12 to a maximum of 40, or In the case of the MIR / EIR of 15 to 40.
Analysis of Job Satisfaction: Concordance
In the present study, job satisfaction has been assessed through three instruments:
Firstly and fundamentally, the overall score of the “Roja Font” AP Questionnaire (GAS) that classifies the professionals into three categories (satisfied, unsatisfied, indifferent) and that is the final result of the score obtained in the 24 items of the same. Secondly, the result of the answer to item number 7 of the aforementioned questionnaire ("In my work, I am satisfied"). Thirdly and lastly, with a closed question that was introduced in the collection questionnaire that seeks to reflect the "self-declared satisfaction" and asks directly the professionals if they are generally satisfied with their work or not.
In the first place we evaluated the concordance between the three instruments, for which we calculate the Kappa index. We observed that there is a discrepancy between self-reported satisfaction and the result of item number 7, as well as between item number 7 and the overall result of the questionnaire (GAS). There is an agreement between self-reported satisfaction and the overall questionnaire score (GAS), although the degree of agreement is low (Kappa between 0.2 and 0.4)
Analysis of Job Satisfaction: Results
Regarding "self-reported satisfaction", we observed that 83.9% of participants answered that they were satisfied with their work compared to 12.2% who were not satisfied.
According to the score of item 7 of the Questionnaire, 66.5% were satisfied, 19.6% were indifferent and 14% were not satisfied. And finally, following the GAS, 62.4% of our professionals studied are satisfied, 2.1% are indifferent, and 35.5% are dissatisfied.


If we proceed to analyze the results obtained in the nine dimensions of the “Font Roja” AP questionnaire, we find that the dimensions with the highest percentage of satisfied professionals are dimension 1 "Satisfaction for work" and dimension 7 "Interpersonal relationship with the coworkers, "in which 84.8% and 81.8% of professionals are satisfied respectively.
The dimensions with the highest percentage of unsatisfied professionals are: dimension 2 "Work-related stress", dimension 5 "Professional promotion" and dimension 4 "work Pressure", where 66.3%, 52.9% and 50.5 % of professionals are dissatisfied respectively.
Analysis of the relationship between GAS and the rest of the variables
We analyzed the relationship between the GAS grouped in categories (Satisfied, indifferent and unsatisfied) with the independent variables.

We found statistically significant differences between the global satisfaction and the years that have been working in primary care, the number of patients attended per day, the type of contract, the professional category and the healthcare center (educational/ non-educational).
Regarding to the number of years working in Primary Care, we found that unsatisfied professionals have been working in primary care (19.82) for more years than those who were satisfied (15.88). Regarding the type of contract, we can observe that the percentage of professionals dissatisfied in interim or fixed is 35.8% compared to 45.2% of the contingent.
The percentage of dissatisfied in professionals working in healthcare centers without teaching is 40.9% compared to 29.9% of those working in teaching centers. If we take into account the pressure of medical healthcare, we observe that the average medical care pressure for unsatisfied professionals is 70.03, compared to 49.4 for satisfied professionals.
Finally, the professional categories with the highest percentage of dissatisfied are doctors (50.4%) and administrative (42.3%), compared to 25.2% of nurses or 11.1% of MIR / EIR. In the rest of the variables we did not observe statistically significant differences.
To evaluate the effect of the age or years worked in primary care, professional category, teaching assist health center or not, type of contract and number of patients cared for on job satisfaction (GAS), we performed a binary logistic regression. The regression model was statistically significant (X2=42.834, p<0.001).
The model explains 19.9% of the variance in job satisfaction (Nagelkerke R2 = 0.199) and correctly classifies 68.9% of the cases. The sensitivity was 83.23%, the specificity was 45.63%, the positive predictive value was 71.28%, and the negative predictive value was 62.66%. Of the six independent variables, only two were statistically significant, the professional (OR=3.833; IC95%=1.334-11.012) and the number of patients attended per day (OR= 1.014; IC95%: 1.003-1.025).

If we proceed to analyze the different dimensions that make up the questionnaire of “Font Roja” AP in relation to the rest of independent variables, we find the following statistically significant relations:
The "work monotony" dimension is related to the professional category (p = 0.026), 48.15% of the administrative staff score high (they consider the work very monotonous), compared to 27% for family doctors.
The "Professional status" dimension is related to the professional category (p <0.001) and 75% of the administrative staff are dissatisfied with the professional dimension, compared to 14.7% of the nurses; this dimension is also related to having or not having children (p = 0.016), being more dissatisfied (37.7%) those who have children compared to those who do not (27.4%).
The dimension "Interpersonal relationship with coworkers" is associated with the professional category (p = 0.03) and with the type of contract (p = 0.036). Thus, 7.7% of administrative staff and 1.8% of family doctors are dissatisfied and 5.2% of those with a stable contract and 0% of those who are temporary.
The dimension "Interpersonal relationship with the bosses" we observed an association with the professional category (p = 0.007), 29.5% of the doctors were dissatisfied, compared to 12.7% of the nurses.
"Professional promotion" is related to the professional category (p <0.001), type of contract (p <0.001) and gender (p = 0.03). Thus, 80.8% of the administrative staff is dissatisfied, compared to 43.1% of the nurses, 56.3% of those with a stable contract, 54.8% of the contingents, 11.1% of the MIR / EIR, and 49.4% of the Men compared to 55.6% of women.
"Pressure at work" is related to the professional category (p <0.001), with 31.3% of the doctors being dissatisfied, compared to 14.7% of the nurses or 7.7% of the administrative staff.
"Professional competence" is related to the type of contract (p = 0.026), 32.3% of which are unsatisfied, compared to 17.8% of the stable ones.
"Work-related stress" was related to the professional category (p <0.001), with 85.7% being unsatisfied doctors, compared to 53.8% of the administrative ones.
"Work satisfaction" is related to the professional category (p <0.001) and to the type of contract (p = 0.041); 95.1% of the nurses, 100% of the MIR / EIR compared to 61.5% of the administrative staff, and 86.3% of the proprietary and interim compared to 74.2% of the eventual ones.
Analysis of the behavior of variables in the nursing staff
The average age of nursing professionals was 52.6 years (Standard deviation: 11.1). 80.6% are women, 61.2% are married or have a stable partner, and 64.1% have children. 74.8% are permanent statutory, with an average of 15.3 years working in primary care. 52.4% work in non-teaching health centers. The average healthcare pressure they had was 21.85 patients per day. 91.3% of the nurses, declared they generally satisfied with the work; and according to the “Font-Roja” Questionnaire 70.9% are satisfied.
The most satisfied dimensions are: "Interpersonal relationship with coworkers" (79.6%), "interpersonal relationship with bosses" (73.8%), "professional competence" (71.8%) and professional status (61.2%). The most dissatisfied dimensions are: "professional promotion" (42.7%), "pressure at work" (35%) and "work monotony" (29.1%).
If we perform a univariate analysis for each of the dimensions, we find that the monotony dimension at work generates greater dissatisfaction at an older age (56.5 vs. 49.32, p = 0.02).
The professional promotion dimension generates greater dissatisfaction at an older age (56 vs. 47.95, p = 0.004), with more years worked in primary care although it does not become statistically significant (17.7 vs. 12.54, p = 0.07), and have a stable contract Compared to eventual (46.7% vs. 10%, p = 0.048).
The work pressure dimension generated greater dissatisfaction with the greater number of patients treated per day (24.34 vs. 19.92, p = 0.001). The dimension of tension in the work generates more dissatisfaction at a higher age (54.49 vs. 52.03, p = 0.006), to a greater number of patients (22.34 vs. 19.58, p = 0.027), and to have a stable contract (62.2% vs. 40% P = 0.028).
The professional status dimension generated higher satisfaction at younger age (50,019 vs. 57.57, p = 0.024). In the other dimensions (interpersonal relationship with peers and bosses, professional competence) no statistically significant differences were observed.
DISCUSSION
The participation rate is similar to other studies conducted in our Autonomous Community18),(19 which achieved response rates of 61.35% and 54%, respectively; Similar to the 57.7% achieved by our study. This participation rate is somewhat lower than studies conducted elsewhere in our country14), (16), (17),(20)(21. Nevertheless, we understand that it is sufficient for the results to be representative of the population studied.
It is practically impossible to compare the results of the different studies with a large variability in the way the “Font-Roja” AP questionnaire was analyzed.
The low degree of agreement between the result of the questionnaire (GAS) and the self-declared satisfaction by the professional in closed question leads us to think that, perhaps, since job satisfaction is so subjective and personal, ended-questions with only two options are not Suitable as a valuation tool and we should use questionnaires that investigate in a greater number of dimensions or nuances and with a certain gradation of possibilities (Likert scales).
From the results obtained we can draw a profile of the unsatisfied professional:
Male doctor, with older age, separated and with children, who has an eventual contract in a non-teaching health center and who has been working for more years in primary care and with high care pressure in consultation.
On the contrary, the profile of the satisfied professional would be that of a female, nurse, young, single and without children, with a place in property that works in a teaching health center, who has been working in primary care for a few years and with low assistance pressure in the consultation.
These profiles are in great agreement with those presented in previously published studies, and in our community a work was published19, where age was a relevant variable in self-reported satisfaction, with young people showing the greatest sense of possibility of improvement, expectations and possibilities To learn new things.
Still of all the variables we have observed that the ones that have a greater weight are the number of patients attended to the day, and the professional category; Generating greater dissatisfaction with a greater number of patients; And the professional category being 3.8 times more likely to be unsatisfied if you are a doctor.
In relation with the dimensions assessed in the “Font-Roja” questionnaire, we can observe that the worst-valued dimensions are "Tension at work", "Professional promotion" and "Work pressure", dimensions that largely coincide with what was found in previous studies 5) (16),(17),(18)(22.
It is known that work stress can be a source of stress in the individual, and may be caused by multiple factors such as workload, coping with patient expectations, illness-related death status, etc. In our case, one of the reasons for this poor assessment by doctors could be the pressure on healthcare and responsibility in clinical decision making, among others.
In relation to the "Professional Promotion" we have to take into account that our study is carried out in public healthcare centers, and professionals are statutory; Taking into account this, professional promotion has been a concern for the healthcare administration for a long time, with career and professional development being the biggest bet to improve this dimension in fixed statutory personnel (who are the ones who reach the worst score in this dimension), But as we see it seems to be unsuccessful.
In relation to professional promotion, it call us the intention that the fact that there is a worse evaluation (with significant differences) in females than in males, and this in a sector with a large majority of women. We understand that this difference in perception would merit a greater number of studies to assess whether promotion policies are being implemented that marginalize the future development of female in public healthcare centers.
The dimensions that have reached a higher score in the degree of satisfaction have been "job satisfaction" and "interpersonal relationship with coworkers". This last dimension agrees with what was seen in the work carried out in Asturias in the year 2013 18.
The researchers used another questionnaire that was different from ours but included an item that could be similar to "Conflicts with other people from my work", to which the participants gave a low score (3.23 out of 10).
This fact is important, because it is known that a good relationship between coworkers is a factor of protection against the work stress, increases the degree of satisfaction and the illusion for the work. On the other hand, a poor relationship in primary care teams has also been described as a risk factor for attrition 21.
In relation to the dimension "work satisfaction" if we look at the items that compose the two that score higher are "I am interested in the things I do" and "I have the feeling that what I do is worth" we might think, The work carried out in healthcare centers has a motivating component for its professionals; And perhaps are confirmed as key elements to reinforce to increase the satisfaction, relevance and significance of work for citizens.
In relation to the evaluation that the professionals realize of their training we find that they obtain positive scores. Thus the item "I often feel I am not qualified for my work" has an average score of 1.97 (1 being totally disagree with the affirmation); this data coincides with previous research 5),(17),(18),(22.
All the groups reflect that they feel competent in their work, which could be related to the fact that these are generally highly qualified groups, where people with higher education levels and, in many cases, specialized training predominate. This feeling of high training may also be related to the fact that most of our workers are fixed with extensive experience in the field of Primary Care; Or with a self-assessment bias.
Finally, it seems interesting to reflect that when crossing the different dimensions with the rest of independent variables, we observe that each dimension is related to different variables and with different categories. This can give us a clue about the nuances of dissatisfaction according to the professional profile. For example we observe that the monotony is related to the professional category, but they punctuate well with the doctors and very bad the administrative ones, and nevertheless, in the work pressure is the opposite. This leads us to think that the strategies to increase the satisfaction of the professional must contemplate different profiles.
It seems essential and urgent for our organization to begin designing strategies that, first, value the satisfaction of the professional and associated variables and then, establish improvement actions that should be dynamic, continuous over time and multiple to fit the different current professionals, and different vital moments. Generic policies for all professionals will not serve to improve overall satisfaction in the organization most likely.
Looking at the most affected dimensions, it seems that the strategies should be aimed at improving career development, reducing job monotony and pressure and tension at work, perhaps designing job positions that, after years of experience, begin to combine assistance tasks with Other tasks (research, teaching, management, planning and community intervention) by reducing the time spent on care and replacing it with tasks related to those areas could help increase nurses' job satisfaction. Also reflect on the possibility of introducing days of leave linked to pressure at work, and not just the antiquity as it is now.
CONCLUSIONS
Job satisfaction is a personal dimension that requires the approach through questionnaires that gradually value different dimensions.
The majority of professionals is satisfied; Even so, there is a high percentage of dissatisfaction and constitutes a relevant problem for the organization.
It would be necessary if management analyze the professional’s satisfaction, valuing both aspects that generate dissatisfaction and satisfaction (such as the relevance of work) by professional category and contemplating other variables of a social nature.
In the professional promotion we must pay attention to the gender variable, carrying out specific studies in the first place and establishing corrective mechanisms if necessary.
We understand that job satisfaction is a dynamic issue which changing as other factors change; we must establish valuation mechanisms on an ongoing basis throughout the professional’s life.
Strategies should be derived from this analysis to increase satisfaction; But personalized, at least if by profiles.
The general aspects that most influence dissatisfaction are the professional category and the pressure on healthcare.
The categories that most satisfy are the professionals in training and the nursing staff. The most unsatisfied, doctors and administrative staff, albeit for different motives.
Strategies must be found that allow professional development by varying the functions and tasks, reducing the burden from healthcare and introducing other areas of interest such as research, management and planning, teaching and community intervention for professionals.
Other possibilities would include the design of working days in which more days are permitted associated with work pressure, and not only the seniority, are allowed.
REFERENCIAS
1. Fernández MI, Villagrasa JR, Gamo MF, Vázquez J, Cruz E, Aguirre MV, et al. Estudio de la satisfacción laboral y sus determinantes en los trabajadores sanitarios de un área de Madrid. Rev Esp Salud Pública. 1995; 69(6): 487-497. [ Links ]
2. Mayo E. The social problems of an industrial civilization. Cambridge, Mass: Harvard University Press. 1945 [ Links ]
3. Maslow AH. Motivation and personality. 2nd ed. Nueva York: Harper and Bros. Publishers, 1970. [ Links ]
4. Herzberg F. The motivation to work. 2nd ed. Nueva York: John Wiley and Sons, 1959. [ Links ]
5. López-Soriano F, Bernal L, Cánovas A. Satisfacción laboral de los profesionales en un Hospital Comarcal de Murcia. Rev Calidad Asistencial. 2001;16:243-246. [ Links ]
6. Evolución de la enfermería hacia la satisfacción profesional [editorial].Rev Esp Sanid Penit. 2009; 11:65-67. [ Links ]
7. Ramírez-Sánchez TS, Nájera-Aguilar P, Nigenda-López G. Percepción de la calidad de la atención de los servicios de salud en México: perspectiva de los usuarios. Salud Pública de Méx 1998;40(1):3-12. [ Links ]
8. Hernández LB, García PC, et al. Satisfacción de usuarios en unidades de medicina familiar. Rev Med IMSS. 2002; 40(5):373-378. [ Links ]
9. Ponce-Gómez J, Reyes-Morales H, Ponce-Gómez G. Satisfacción laboral y calidad de atención en enfermería en una unidad médica de alta especialidad. Rev Enferm IMSS 2006;14(2):65-73. [ Links ]
10. Parada ME, Moreno R, Mejías Z, Rivas A, Rivas F, Cerrada J, et al. Satisfacción laboral y síndrome de burnout en el personal de enfermería del Instituto Autónomo Hospital Universitario Los Andes, Mérida, Venezuela. Revista Facultad Nacional de Salud Pública 2005. 23(1):33-45. [ Links ]
11. Ibern P. La medida de la satisfacción en los servicios sanitarios. Gac Sanit. 1992;6:176-85. [ Links ]
12. Hyrkas K, Appelqvist-Schmidlechner K, Haataja R. Efficacy of clinical supervision: influence on job satisfaction, burnout and quality of care. J Adv Nurs. 2006; 55(4): 521-35. [ Links ]
13. Fernández G. Satisfacción laboral y salud psíquica en el mundo sanitario, ¿un lujo?. Todo Hospital. 1995;118:29-36. [ Links ]
14. Vera-Remartínez EJ, Mora LM, González JA, García J, Garcés E, Domínguez JA, et al. Satisfacción laboral de la enfermería en las prisiones españolas. Rev Esp Sanid Penit. 2009; 11:80-86. [ Links ]
15. Peya M. Satisfacción laboral: una breve revisión bibliográfica. Nursing. 2008; 26(2): 62-65. [ Links ]
16. Fernández MI, Villagrassa JR, Gamo MF, Vázquez J, Cruz E, Aguirre MV, et al. Estudio de la satisfacción laboral y sus determinantes en los trabajadores sanitarios de un Área de Madrid. Rev Esp Salud Pública. 1995; 69(6): 487-497. [ Links ]
17. Fernández MI, Moinelo A, Villanueva A, Andrade C, Rivera M, Gómez JM, et al. Satisfacción laboral de los profesionales de Atención Primaria del Área 10 del Insalud de Madrid. Rev Esp Salud Pública. 2000; 74(2): 139-147. [ Links ]
18. Díaz C, Suárez O, Fueyo A, Mola P, Rancaño I, Sánchez AM, et al. Calidad de vida de los profesionales en el modelo de Gestión Clínica de Asturias. Gac Sanit. 2013; 27(6): 502-507. [ Links ]
19. Olivar C, González S, Martínez MM. Factores relacionados con la satisfacción laboral y el desgaste profesional en los médicos de Atención Primaria de Asturias. Aten Primaria. 1999; 24: 352-9. [ Links ]
20. Lomeña JA, Campaña FM, Nuevo G, Rosas D, Berrocal A, García F. Burnout y satisfacción laboral en Atención primaria. Medicina de Familia. 2004; 5(3): 147-155. [ Links ]
21. Sobrequés J, Cebriá J, Segura J, Rodríguez C, García M, Juncosa S. La satisfacción laboral y el desgaste profesional de los médicos de atención primaria. Aten Primaria 2003; 31(4):227-33. [ Links ]
22. Pérez MT, Díaz C. Satisfacción laboral en enfermeros/as de Atención Primaria del Servicio Gallego de Salud. Metasdeenfermería 2007; 10(10):6-10. [ Links ]
23. Fernández AM, Santa Clotilde E, Casado MI. Calidad de vida profesional de los profesionales de enfermería en Atención Primaria de Soria. Biblioteca Lascasas 2007; 3(1). Disponible en http://www.indexf.com/lascasas/documentos/lc0213.php [ Links ]
24. Aranaz J, Mira J. Cuestionario Font Roja. Un instrumento de medida de la satisfacción en el medio hospitalario. Todo Hosp. 1988; 52: 63-66. [ Links ]
Received: April 15, 2016; Accepted: July 19, 2016
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
