










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.17 no.50 Murcia abr. 2018 Epub 14-Dic-2020
https://dx.doi.org/10.6018/eglobal.17.2.277821
Originals
Telephone support for adherence to healthy eating practices among people with type 2 diabetes mellitus
1 Nutricionista, Doctora en Ciencias por la Escuela de Enfermería de Ribeirão Preto - Universidad de São Paulo.Brasil.
2 Enfermera, Doctora en Ciencias por la Escuela de Enfermería de Ribeirão Preto - Universidad de São Paulo, Brasil.
3 Profesional de Educación Física, Doctoranda por la Escuela de Enfermería de Ribeirão Preto - Universidad de São Paulo. Brasil.
4 Profesora Concursada de la Escuela de Enfermería de Ribeirão Preto de la Universidad de São Paulo, Centro Colaborador de la OMS para el Desarrollo de la Investigación en Enfermería. Brasil.
Objective:
To verify the effects of telephone support on adherence to healthy eating practices among patients with type 2 diabetes mellitus.
Methods:
This was a clinical trial with 63 patients with type 2 diabetes mellitus; 36 patients were allocated to the intervention group (G1) and 27 patients to the control group (G2). For G1, telephone support was provided, consisting of four telephone calls addressing food planning, types and portions of food, and healthy foods. For G2, normal care was given in their health facility. The effects of telephone support on healthy eating were measured at baseline (T1) and at four months after the intervention (T2).
Results:
In G1, 16 (44.44%) patients joined at T1, which dropped to 14 (38.88%) by T2. In G2, 8 (29.62%) patients started at T1 and the number rose to 9 (33.33%) by T2. After the G1 intervention, there was an increase in the consumption of fruits and vegetables, a reduction in the consumption of fatty foods and foods high in sugar, and an increase in meal frequency. A significant difference was noted in reduced fasting blood glucose among non-adherent patients and reduced Hb1Ac among adherent patients from G1.
Conclusion:
The four-month intervention using telephone support proved insufficient to increase adherence to healthy eating. However, there was an increase in consumption of fruits and vegetables and a decrease in the consumption of fatty foods, foods high in sugar, and soft drinks.
Keywords: Diabetes mellitus; Food and nutritional education; Telephone
INTRODUCTION
In Brazil, the Ministry of Health created a document containing the Ten Steps for Healthy Eating in order to promote good eating habits in the country; the use of these recommendations has been explored in the literature1. A study conducted in Pelotas, in the state of Rio Grande do Sul, measured the frequency of the Ten Steps for Healthy Eating in 3,136 adults from the general population; it found that only 1.1% of the population studied adhered to the ten steps2.
In relation to diabetes mellitus (DM), a study that investigated 104 patients found that 37% did not adhere to the recommended nutritional plan3. Another study that examined the factors related to lack of glycemic control in 917 patients with type 2 DM indicated that 81% of the participants did not follow the food plan provided by nutritionists4.
It is recognized that DM treatment involves healthy eating, regular physical activity and drug therapy. However, the most challenging aspect for most people with diabetes is maintaining good eating habits, which are viewed as prohibitive and restrictive5 6-7.
This situation requires health professionals to provide adequate information about acquiring healthy food habits. To this end, professionals have used various educational resources, apart from face-to-face strategies. One resource that has been explored in the field of health is the use of the telephone as an intervention strategy, due to quick access by patients and health professionals, less waiting time for consultations, reduced patient transportation time, and the possibility of increasing frequency of contact with family members and facilitating the return of patients to health facilities8.
From this perspective, telephone support can become an expansion of health care, since it represents a potential intervention for providing comprehensive care. It is predicted that telephones will be used more in the coming years as an important means of communication between health professionals and patients9.
In this context, the objective of the present study was to verify the effects of telephone support on adherence to healthy eating practices among people with type 2 DM. Hopefully, the results of this study will serve to provide input for the adherence of DM patients to one of the pillars of treatment: maintenance of good eating habits.
MATERIALS AND METHOD
This was a pragmatic clinical trial conducted in the state of São Paulo, Brazil, in 2013. The base population was 1,298 patients/insulin users registered in electronic systems of the Municipal Department of Health. The inclusion criteria were: being at least 18 years old; both genders; having the ability to hear and respond to questions; having a residential phone; and being diagnosed with type 2 DM.
A total of 1,298 patients were invited to participate by phone; of these, 98 agreed to participate in the study. The patients were randomly selected and divided into two groups: G1, the intervention group (49 patients); and G2, the control group (49 patients). The data was collected at the baseline of the study (T1) and four months later (T2). Of the 98 participants, only 63 completed the two stages of the study: 36 from G1 and 27 from G2.
For G1, the intervention, called telephone support in diabetes monitoring (ATEMDIMEL), was performed by three nurses, one nutritionist and one physical educator, and its objective was to increase metabolic control. A manual based on the Guidelines of the Brazilian Diabetes Society9 and a guide with key aspects for DM education, recognized by the American Diabetes Association10,11, were used for this intervention. The total number of calls and intervention time were based on studies from ATEMDIMEL12,13.
The content of the intervention consisted of four themes: general concepts, use of medication, food planning, and engaging in regular physical activity. Each theme corresponded to four calls a month, with an average call time of 20 minutes, totaling 16 weekly calls. In relation to food planning, the following aspects were addressed: food planning concepts (importance for controlling DM); types of nutrients (carbohydrates, proteins, fats); meal frequency; and inclusion of healthy foods. At the end of each call, a personal goal was established that was reviewed in the next call.
In G2, the patients received normal care in their health facilities. Letters with the results of the lab tests were sent by mail, along with a suggestion to show them in their next medical and/or nutritional consultation.
A questionnaire to characterize the sociodemographic, anthropometric and clinical variables of the patients was used to obtain that data. The anthropometric variables were weight and height. Body mass index (BMI) was calculated.
The clinical variables were fasting blood glucose and glycated hemoglobin (HbA1c). Fasting blood glucose (mg/dl) was considered adequate if it was lower than 130 mg/dl and higher than 70 mg/dl10. As for HbA1c, it was considered adequate when it was below 7% for patients less than 65 years of age, and below 8% for patients over 65 years old10.
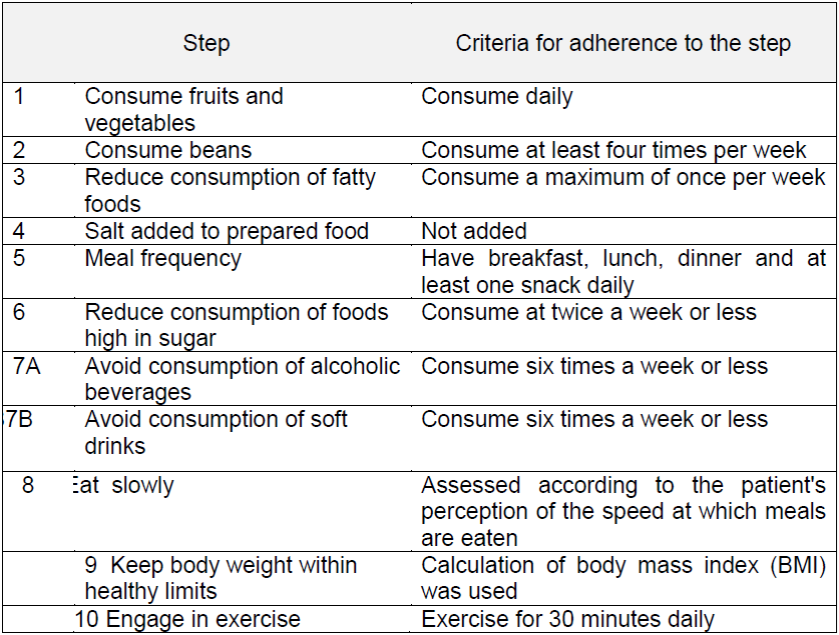
The Ten Steps for Healthy Eating questionnaire was also used, which was adapted for this study, i.e., Step 7 was subdivided into Step 7A and Step 7B2. Adherence to healthy eating was assessed individually and compliance was defined as adherence by patients to six steps: 1, 2, 3, 5, 6 and 7b. This criterion was adopted as being directly related to the metabolic control of people with DM, in accordance with the recommendation of the Brazilian Diabetes Society10.
Adherence by patients with type 2 DM to each of the steps was assessed according to the pre-established criteria, and is shown in Table 1.
Descriptive statistics were prepared for the data analysis and Fisher's exact test was used to determine the associations between the qualitative variables14. The study was approved by the Research and Ethics Committee of the School of Nursing of Ribeirão Preto-USP, under Protocol No. 324098, and the database for clinical research with human subject at ClinicalTrials.gov, under Protocol No. NCT01972412.
RESULTS
Of the 63 (100%) patients, 36 (57.14%) from G1 received the educational intervention via telephone support and 27 (42.85%) in G2 received normal care in their health facilities and letters with the lab test results.
In relation to the sociodemographic variables, in G1, 16 (44.4%) patients were men and 20 (55.5%) women; 1 (2.7%) was single, 23 (63.8%) were married, 7 (19.4%) were widows, and 5 (13.8 %) were separated. With respect to the length of time of DM diagnosis, 3 (8.3 %) patients had been diagnosed up to 5 years ago, 8 (22.2 %) from 6 to 10 years ago, 14 (38.8 %) from 11 to 20 years ago, and 11 (30.5%) more than 25 years ago.
As for the clinical variables, at the baseline of the study, the mean BMI was 31.5 kg/m² (±5.5) for patients from G1 and 32.6 kg/m² (±6.3) for patients from G2; mean fasting blood glucose was 162.6 mg/dl (±96.3) for G1 and 128.5 mg/dl (±55.4) for G2; and mean HbA1c was 9.3% (±2.2) for G1 and 8.0% (±1.8) for G2.
Adherence to each of the ten healthy eating steps before and after the intervention (T1-T2) is presented in Table 1. The steps with the highest frequency of adherence in G1 were reduced alcohol consumption, followed by reduced salt consumption. Besides these steps, G2 adhered to reduced soft drink consumption.
Table 1 Adherence of patients with type 2 DM to the Ten Steps of Healthy Eating before and after an educational phone intervention. Ribeirão Preto, Brazil, 2014.
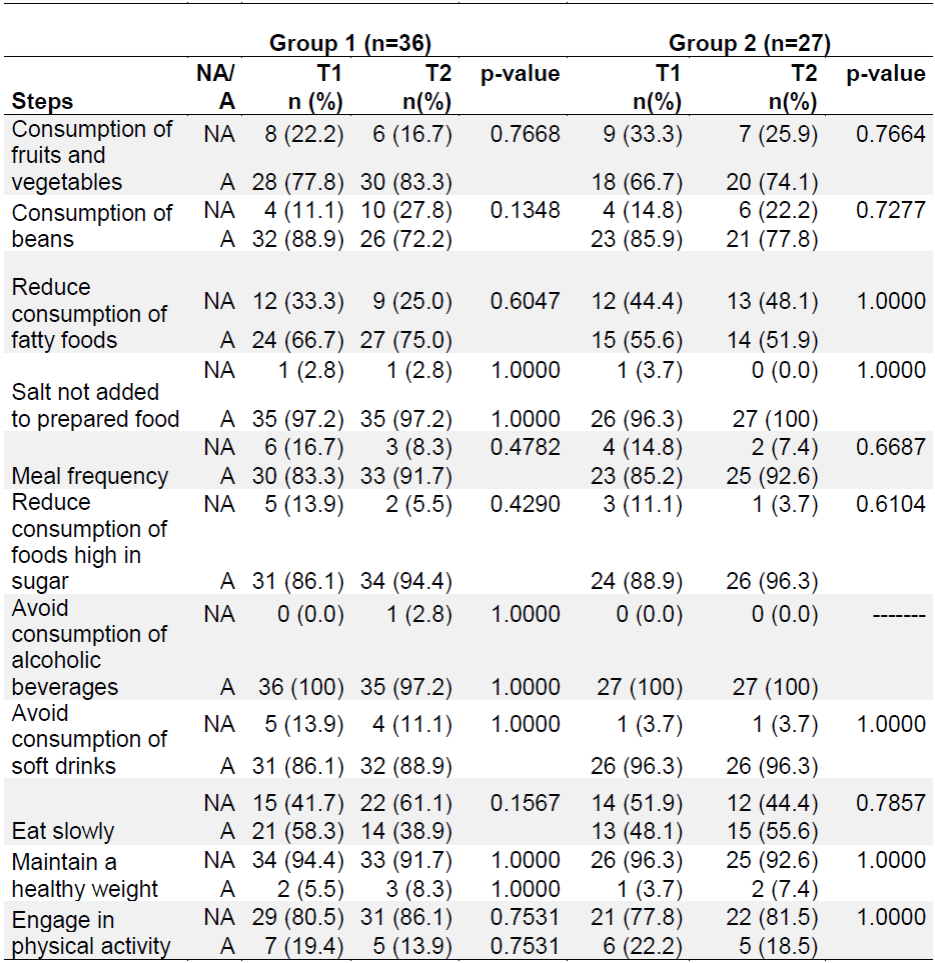
p-value = refers to Fisher's exact test; NA = Non-adherence; A = Adherence.
When analyzing the outcome of adherence to healthy eating according to the criteria chosen for the present study on people with DM, it was noted that 16 (44.4%) patients from G1 adhered at T1, which dropped to 14 (38.8%) by T2. In G2, 8 (29.6%) patients started at T1 and this number rose to 9 (33.3%) by T2.
Table 2 shows the distribution of the G1 and G2 groups in relation to adherence to healthy eating before and after the intervention, in terms of BMI, fasting blood glucose and HbA1c.
Table 2 Adherence to healthy eating and metabolic control before and after an educational intervention with telephone support. Ribeirão Preto, Brazil, 2014.

NA = Non-adherence; A = Adherence; SD = Standard deviation; T1 = Time 1; T2 = Time 2; BMI = Body mass index; Glucose = Fasting blood glucose; HbA1c = Glycated hemoglobin.
There was a statistically significant difference in reduction of fasting blood glucose among non-adherent patients from G1 (Table 3).
Table 3 Fasting blood glucose before and after an educational phone intervention in relation to adherence to healthy eating. Ribeirão Preto, Brazil, 2014.
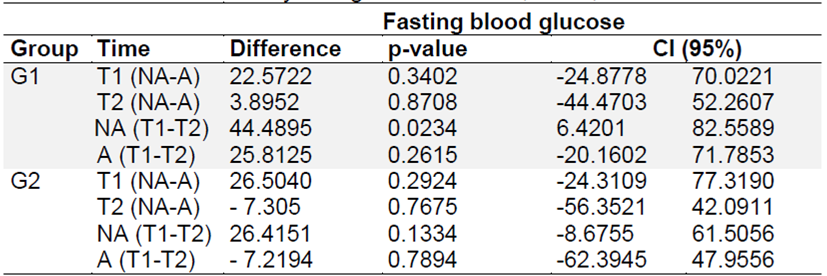
G1 = Group 1; G2 = Group 2; T1 = Time 1; T2 = Time 2; NA = Non-adherence; A = Adherence
There was also a statistically significant decrease in Hb1Ac among adherent patients from G1 and a statistically significant increase in HbA1c among non-adherent patients from G2 in relation to healthy eating (Table 4).

DISCUSSION
With regard to sociodemographic variables, it was found that most patients with type 2 DM were women, were over sixty years of age, and were married, which is consistent with findings from other national and international studies3,4,12,13,15.
In terms of the outcome related to adherence to healthy eating, there was no increase after the participation of patients in the study. Low adherence to food plans has also been observed in international and national studies, although with different methodologies2,3,4,16,17.
However, there has been evidence over the history of treating DM that nutritional therapy is essential for maintaining metabolic control. Therefore, striving to motivate patients to adhere to healthy eating practices is an essential aspect for health professionals5,10,18,19. It is worth noting that after the educational telephone intervention, there was increased adherence to certain steps in both groups, particularly increased consumption of fruits and vegetables and decreased consumption of fatty foods, foods high in sugar and soft drinks, which results in improved nutritional quality.
Although not the main focus of the present study, it was observed that, after the educational phone intervention, BMI rose among patients from G1 who adhered to healthy eating practices. There is a recommendation in the literature that people with DM maintain proper weight to promote metabolic control and prevent the appearance of complications 5,10. However, weight loss depends on engaging in regular physical activity and healthy eating practices, among other factors. It should be pointed out that the findings of the study showed that physical activity was the step with the lowest level of adherence among both groups, which could explain the increase in BMI after the educational telephone intervention, in addition to the complexity involved in the weight loss process.
In terms of metabolic control, there was a statistically significant difference in reduction of fasting blood glucose among non-adherent patients and reduction of Hb1Ac among adherent patients from G1, whereas there was a statistically significant increase in HbA1c among non-adherent patients from G2 in relation to healthy eating. Another study obtained similar results, i.e., although no decrease in BMI was noted, metabolic control improved in the telephone intervention group, with reduced fasting blood glucose and HbA1c20.
The results also suggest that the four-month intervention period may have been insufficient for achieving weight loss, but there was an effect in terms of fasting blood glucose and HbA1c, which is clinically relevant in treating DM.
It is also possible that four telephone calls per week to patients with type 2 DM were insufficient for addressing a complex theme such as eating and nutrition, even though a total of 16 weekly calls were made. Therefore, other studies are needed with longer follow-up periods and higher numbers of phone calls with a specific focus on aspects related to eating and nutrition in diabetes.
CONCLUSIONS
The results obtained demonstrated that four months of educational intervention by phone were not effective in increasing adherence to healthy eating practices among people with type 2 DM. However, there was a slight reduction in fasting blood glucose and HbA1c. There was also increased adherence to consumption of fruits and vegetables and decreased consumption of fatty foods, foods high in sugar, and soft drinks, although these differences were not statistically significant.
Analyzing adherence by people with type 2 DM to a food plan that follows the ten steps of healthy eating is a challenging task, particularly since the goal is changes in behavior resulting from the use of an educational telephone strategy. Even though telephone support is an easily accessible and low-cost strategy, it requires the preparation of specific, updated protocols and effective communication on the part of researchers. It should be noted that in this study, the instrument created for the general population was adapted for patients with diabetes. Therefore, future studies are recommended for comparison purposes.
REFERENCES
1. Brasil. Ministério da Saúde. Guia alimentar para a população brasileira. Disponível em: http://portalsaude.saude.gov.br/images/pdf/2014/novembro/05/Guia-Alimentar-para-a-pop-brasiliera-Miolo-PDF-Internet.pdf. Acesso em: 06/01/2015. [ Links ]
2. Vinholes DB, Assunção MCF, Neutzling MB. Frequência de hábitos saudáveis de alimentação medidos a partir dos 10 Passos da Alimentação Saudável do Ministério da Saúde: Pelotas, Rio Grande do Sul, Brasil. Cad. Saúde Pública. 2009;25(4):791-799. [ Links ]
3. Ganiyu AB, Mabuza LH, Malete NH, Govender I, Ogunbanjo GA. Nonadherence to diet and exercise recommendations amongst patients with type 2 diabetes mellitus attending Extension II Clinic in Botswana. Afr J Prm Health Care Fam Med. 2013;5(1):457. [ Links ]
4. Khattab M, Khader YS, Al-khawaldeh A, Ajlouni K. Factors associated with poor glycemic control among patients with Type 2 diabetes. J Diabetes Complications. 2010; 24(2):84-89. [ Links ]
5. American Diabetes Association. Nutrition Therapy Recommendations for the Management of Adults With Diabetes. Diabetes Care. 2014; 37(Suppl 1):120S-143S. Disponível em: http://care.diabetesjournals.org/content/37/Supplement_1/S120.full.pdf+html. Acesso em:10/01/2016. [ Links ]
6. Inzucchi SE, Bergenstal RM, Buse JB, Diamant M, Ferrannini E, Nauck M, at al. Management of hyperglycemia in type 2 diabetes: a patient-centered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2012; 35(6):1364 -1379. [ Links ]
7. Pontieri FM, Bachion MM. Crenças de pacientes diabéticos acerca da terapia nutricional e sua influência na adesão ao tratamento. Ciênc saúde coletiva. 2010; 15(1): 151-160. [ Links ]
8. Car J, Sheikh A. Telephone consultations. BMJ. 2003;326 (7396): 966-969. [ Links ]
9. Moss EL. “Just a telephome call away”: transforming the nursing profession with telecare and telefone nursing triage. Nurs Forum. 2014;49(4):233-9. [ Links ]
10. Sociedade Brasileira de Diabetes (SBD). Diretrizes da Sociedade Brasileira de Diabetes: 2014-2015. São Paulo: AC Farmacêutica; 2015. [ Links ]
11. Wark PA, Car J. Systematic review: Review suggests mobile phone interventions improve medication adherence; rigorous longer term studies are needed to confirm effects. Evid Based Nurs. 2015;18(4):120. [ Links ]
12. Becker TAC, Teixeira CRS, Zanetti ML. Intervenção de enfermagem na aplicação de insulina: acompanhamento por telefone. Acta paul Enferm. 2012;25(1):67-73. [ Links ]
13. Zanetti, GG, Hodniki PP, de Moraes C et al. Investigating telephone support as a strategy to increase the physical activity levels of people with diabetes. Journal of Diabetes Nursing. 2013:18(1):32-6. [ Links ]
14. Fisher RA. The logic inductive inference. J R Statist Soc 1935;98(1):39-82. [ Links ]
15. Zanetti ML, Arrelias CCA, Franco RC, Santos MA, Rodrigues FFL; Faria, HTG. Adesão às recomendações nutricionais e variáveis sociodemográficas em pacientes com diabetes mellitus. Rev esc Enfem. 2015;49(4):619-625. [ Links ]
16. Hernández-Ronquillo L, Téllez-Zenteno JF, Garduño-Espinosa J, González-Acevez E. Factors associated with therapy noncompliance in type-2 diabetes patients. Salud Publica Mex. 2003;45(3):191-197. [ Links ]
17. Assunção MCF, Santos IS, Costa J. Avaliação do processo da atenção médica: adequação do tratamento de pacientes com diabetes mellitus, Pelotas, Rio Grande do Sul, Brasil. Cad Saúde Pública. 2002;18(1):205-211. [ Links ]
18. Diabetes Control And Complications Trial (DCCT). Research Group: the effect of intensive treatment of diabetes on the development and progression of the long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993,329(14):977-986. [ Links ]
19. United Kingdom Prospective Diabetes Study Group (UKPDS). Intensive blood-glucose control with sulfonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes. Lancet. 1988; 352(9131):837-853. [ Links ]
20. Çevik AB, Özcan S, Satman I. Reducing The Modifiable Risks of Cardiovascular Disease in Turkish Patients With Type 2 Diabetes: The Effectiveness of Training. Clin Nurs Res. 2015;24(3):299-317. [ Links ]
Acknowledgments:
Funding agency: National Council for Scientific and Technological Development (CNPq), Process No. 563598/2010- 7.
Received: December 14, 2016; Accepted: April 07, 2017
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
