










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.17 no.50 Murcia abr. 2018 Epub 14-Dic-2020
https://dx.doi.org/10.6018/eglobal.17.2.284131
Originals
Adhesion to hand hygiene by nursing team in intensive care unit
1 Universidad Estadual do Oeste do Paraná. Brasil.
Objective
To identify adherence to Hand Hygiene (HH) of the nursing professionals of an Intensive Care Unit for adults of a public university hospital.
Methodology
Descriptive, cross-sectional, observational study with a quantitative approach, carried out with 68 professionals in a university hospital in the state of Paraná, Brazil. Data collection occurred from May to October of 2016 for 100 hours of direct observation. A form was developed for characterization of the participants and the Adapted Instrument of the Handbook for Observers - Multimodal Strategy of the World Health Organization for the Improvement of Hand Hygiene was developed. Data were submitted to descriptive analysis, in proportion measurements and Pearson's Chi-Square test, in SPSS Software version 18.0, to verify the association between adhesion and non-adhesion to HH in each of the five recommended moments and among professionals (nurse or technician of nursing), considering a level of significance of 5%.
Results
12 (17.6%) were professional nurses and 56 (82.4%) were nursing technicians. The nursing staff received a general adhesion rate of 311 (47.8%). There was no adhesion to the moment "before performing aseptic procedures". The "after" moments presented higher accession rates.
Conclusion
The rate of adhesion to HH was very low, and hygiene practice before contact with the critical patient needs to be improved with greater urgency.
Keywords: Hand Hygiene; Cross Infection; Patient Safety; Intensive Care Units; Nursing
INTRODUCTION
Persistently, effective prevention and control measures of Healthcare-Associated Infections (HAIs) are required, a relevant problem and challenge that deserve clinical, epidemiological and managerial prominence. This is because, in the various care spaces, HAIs can cause increased costs to the health system, besides constituting a threat to safety for both users and workers1.
In Brazil, it is estimated that 3% to 15% of hospitalized patients are affected by infections2. However, in the context of intensive care, an international study performed in more than 300 hospitals showed frequent involvement of HAIs in patients3.
In order to prevent HAIs, it is known that hygiene measures allow actions of protection to these diseases, with a vast emphasis on hand hygiene (HH) directed to health area professionals who develop care actions4. The hands of the workers are considered the main instrument in the execution of activities in labor practice and therefore, they make up an important reservoir of microbiological agents that cause HAIs. In this aspect, the impact of the nursing team emerges, once it is known that such profession is one that is present in an uninterrupted and direct way in hospital care, scenario of higher incidence and severity of HAIs4.
HH's indirect objective is to prevent infection produced in the care context, since it is a practice based on the removal of dirt, organic material and/or microorganisms2. This simple measure, besides promoting infection control, increases quality in care, optimizes costs, reduces morbidity and mortality, and meets ethical and legal requirements that govern the work in health area; Being considered, for these reasons, a primary action in the search for safe care1.
Although it is a simple and efficient practice, adhesion to HH has been an arduous and complex task(5). Observational studies have shown that adhesion to this practice is below 50% by health professionals6 7-8.
Thus, in an attempt to contribute to the existing paradigm shift, the World Health Organization (WHO) proposed the "Global Alliance to the Patient Safety", based on the assumption that "Clean Care is a Safer Care" in which the first global challenge planed emphasized HH2.
In this line of thought, the indications for hand hygiene do not correspond to the beginning and the end of a sequence of care activity, but they merge into five essential moments, namely: "before establishing contact with the patient; before performing aseptic procedure; after exposure risk to body fluids; after establishing contact with the patient and after establishing contact with the areas close to the patient "1;2.
Furthermore, seeking the guarantee of quality in the actions execution, based on scientific evidences, the observation for the evaluation of HH is a promising way9. Moreover, this is the most relevant indicator of performance, dealing with the behavior of the health professionals and the search for improvements, when recommended in daily life2.
It is postulated that the importance of adhesion to the practice of HH is well-known in view of the safety of the patient, the worker and the care with excellence. In addition, considering the complexity of care in ICUs, the greater risk of development of HAIs in critical sectors, and the relevance of the nursing team in the direct care of hospitalized patients in these environments, it becomes scientifically and socially relevant to carry out research that involves these places and people. This is because, its results can subsidize the planning of actions that contribute to the safety of the intensive care, in reference of HAIs prevention.
Given the above, it is asked: What is the adhesion to HH by the intensive care team? To answer the question, the study aimed to identify the adhesion to HH of the nursing professionals of a ICU for adults of a public university hospital.
METHODOLOGY
This is a descriptive, cross-sectional, observational study with a quantitative approach. The research was developed at the General ICU (for adults) of an university hospital located in the interior of Paraná state, Brazil, with a high complexity in several medical specialties, with a total operational capacity of 210 active beds exclusively associated with the Unified Health System or Sistema Único de Saúde (SUS).
The study scenario (ICU) has 14 beds or assistance points separated by partitions. Regarding the physical structure for HH, the sector has nine dispensers of liquid soap, ten paper towel holders and eighteen sinks for HH. In addition, there are gel alcohol dispensers near the 14 beds.
The study population consisted of the nursing team working in the General ICU under study, which had 70 professionals, 12 nurses and 58 nursing technicians, distributed in the shifts in the morning, afternoon and three nights (12 x 60 hours). It composes the scale of work per shift, from ten to twelve nursing technicians and two nurses.
The study sample consisted of 12 nurses and 56 nursing technicians working in the unit, all shifts. Officials on leave, leave and leave of absence of any nature were considered exclusion criteria.
All the professionals who voluntarily accepted to participate in the study signed the Free and Informed Consent Term or Termo de Consentimento Livre e Esclarecido (TCLE), made available in two copies by the researcher, one of which was granted to the participant.
For the data collection, direct observation was used as the research method. A data collection form was developed to characterize the professionals, composed of objective questions with the following variables: sex, age, professional training, work regime, time of operation in the institution, time spent in the General ICU, training received Related to the theme HH in the last two years and forms of training.
In addition to this, the Adapted Instrument of the Manual for Observers - WHO Multimodal Strategy for the Improvement of HH2, was used to observe the five moments for HH by the nursing team.
Besides the researcher, a student of the course of Nursing, properly trained, assisted in the direct observations of the professionals, after conducting a pilot test.
During the investigations, the instrument was filled based on the indications for HH presented by the professionals, in which the presence of the assessment item in the column was marked with an "I" as performed or not performed. Also, for greater assistance and trustworthiness in the observation, the correspondence table of the instrument was taken as a basis, containing a description of the indications for HH at each moment: "before contact with the patient: (before direct contact); before performing aseptic procedures: (before handling invasive devices, whether or not they are wearing gloves; changing body sites); after exposure to body fluids: (after contact with fluids or excretions, non-intact skin, mucous membrane, wound dressings, moving from a contaminated body site to another, cleaned; after removing gloves); after contact with the patient: (after direct contact with patients, after removal of gloves); after contact with areas close to the patient: (after contact with objects and surfaces, including equipment; after removing the gloves)".
Data collection was carried out from May to October of 2016, in an average of four hours of daily observations, in the three shifts at random, on days and at intercalated schedules, for a total of 100 hours of observations of the opportunities and achievements of HH, by the professionals of the nursing team.
It was used by the researcher the criterion of observing the first member of the team, who participated in the study, that would perform HH, where a professional (nurse or nursing technician) was observed during a period of two consecutive hours of work activities. It should be pointed out that the central focus of the present study was to evaluate the adhesion or not to HH in the five recommended moments. Therefore, the technique performed and the removal of ornaments were not observed.
After that, the data was organized and stored in spreadsheets in Microsoft Excel® version 2010, and then subjected to simple descriptive analysis in proportion measurements. It was also performed the Pearson chi-square test in the SPSS software version 18.0, to verify the association between adhesion and non-adhesion to HH in each of the five recommended moments and among the professionals (nurse or nursing technician), considering significance level of 5%.
It should be noted that the research complied fully with the ethical precepts set forth in Resolution No. 466/2012 of the brazilian National Health Council. In addition, it was approved by the Research Ethics Committee of the Universidade Estadual do Oeste do Paraná (Unioeste), under constitutional opinion No. 1.447.806.
RESULTS
Table 1 presents the characterization of the study participants that make up the nursing team. A majority 54 (79,4%) of the professionals were female, 56 (82.4%) were nursing technicians. Also, 12 professionals who act as nursing technicians also had a nursing degree.
The predominant age was between 30 and 39 years (40-58.8%). The work regime with the highest frequency in the sector studied is statutory professional, totaling 55 (80.9%). Regarding the acting duration in the institution, 49 (72.1%) professionals worked from 1 to 10 years in the institution, and 52 (76.4%) professionals worked from 1 to 10 years in the ICU.
Table 1 Characterization of the participants (n=68) regarding sex, age, professional qualification, work regime, action period at the institution and action period at the General ICU. Cascavel-PR, Brazil, 2016.
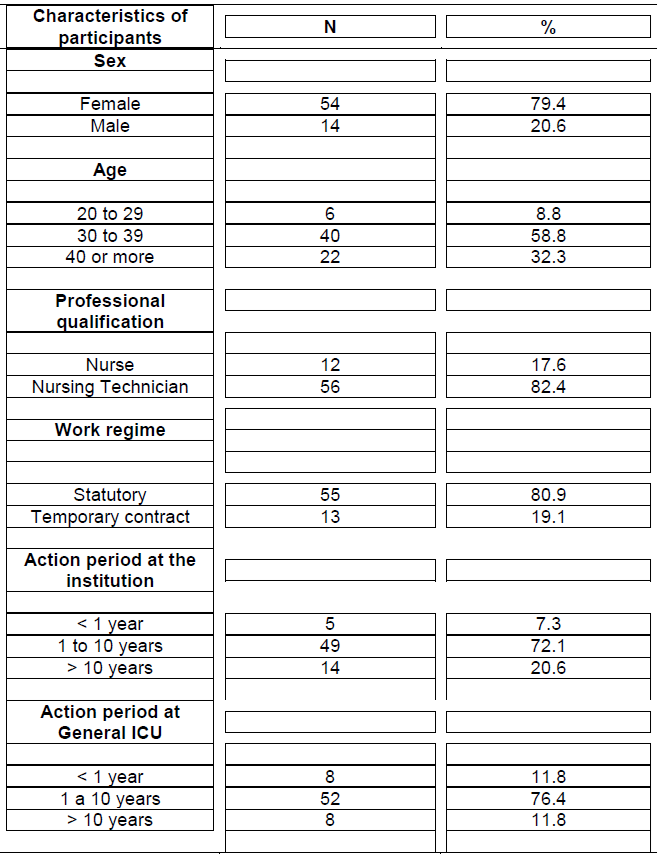
Regarding the receiving training related to HH in the last two years, four (33.3% - n=12) nurses and 29 (51.8% - n=56) nursing technicians reported this information, being in their majority, realized in the form of lectures. Two nursing technicians (3.6%) did not report on the performance of this activity.
Among the observations made in the study, three (6.0%) of these occurred with nurses and 47 (94.0%) with nursing technicians. A majority, 25 (50.0%) of the observations occurred in the afternoon, followed by 13 (26.0%) observations at night, and 12 (24.0%) in the morning shift.
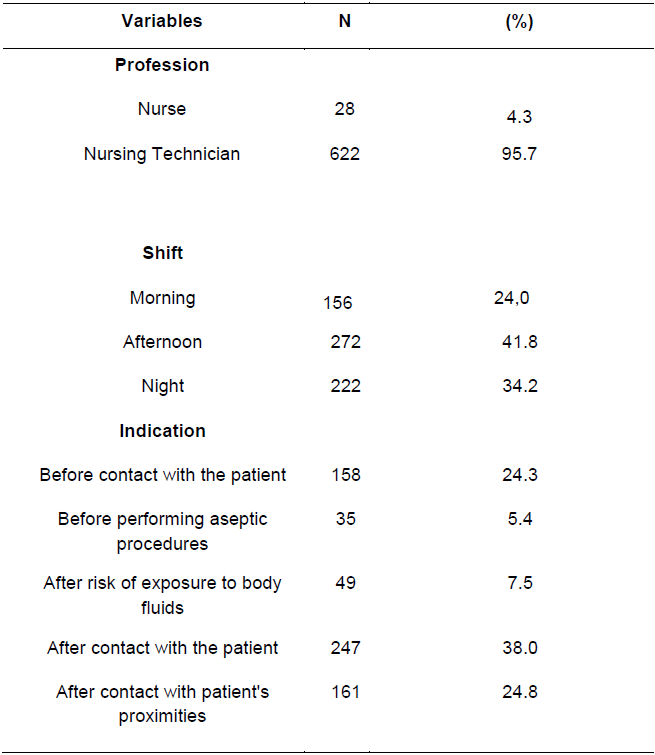
Regarding the characteristics of the observations (Table 2), the nursing professionals received the highest number of indications, with 622 (95.7%) and the afternoon shift, with 272 (41.8%).
With respect to the five moments of HH for nurses and nursing technicians, it was observed 158 (24.3%) moments before contact with the patient, 35 (5.4%) moments before performing aseptic procedures, 49 (7, 5%) moments after risk of exposure to body fluids, 247 (38.0%) moments after contact with the patient and 161 (24.8%) moments after contact with the patient's proximities, totaling 650 indications.
Table 2 Distribution of the characteristics of the observations made (n=650) according to the observed professional, shift and indication for HH. Cascavel-PR, Brazil, 2016.
The general adhesion of the professionals of the nursing team to HH was 311 (47.8%). In the morning shift, 66 (42.3%) HH were adhered; In the afternoon shift, 144 (52.9%) and the night shift 101 (45.5%).
Regarding the five moments, before contact with the patient, there were 16 (10.1%) HH performed by the nursing team; before performing aseptic procedures, there was no adhesion to HH; after risk of exposure to body fluids, 8 (16.3%) HH were performed; after contact with the patient, there were 219 (88.7%) HH and after contact with patient's proximities, among the indications, 68 (42.2%) were performed.
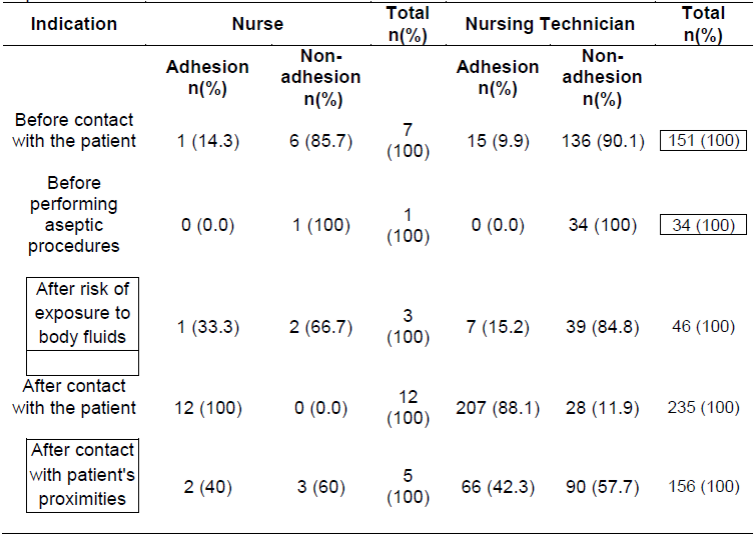
Table 3 shows the adhesion and non-adhesion of HH, distributed by professional category, among the five recommended moments. There was greater adhesion to the technique after contact with the patient by nurses (100.0%) and nursing technicians (207 achievements for 235 indications). The nursing team did not adhere to the practice before performing aseptic procedures, in which nurses had 1 indication and nursing technicians 34 indications.
Table 3 Distribution of the indications to the five moments of HH according to the professional and adhesion to HH. Cascavel-PR, Brazil, 2016.
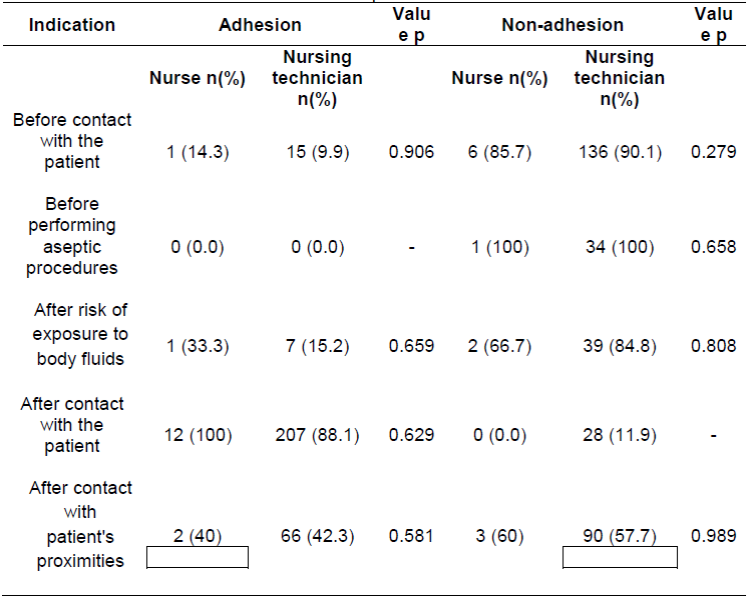
In the evaluation of the dependence between adhesion and non-adhesion to HH in the five recommended moments and the professional (nurse or technician of nursing) observed (Table 4), p value was presented p > 0.05. There is evidence to reject the hypothesis of statistical significance among the variables. Therefore, there is no statistical significance between adhesion to HH or non adhesion to HH and the observed professional (being a nurse or being a nursing technician resulted in the same level of association, ie, being a nurse or being a nursing technician did not interfere with adhesion or not to HH).
It was not possible to perform Pearson's chi-square test for adhesion "before performing aseptic procedures" and for non-adhesion "after contact with the patient", since there were no observations in these variables by two professional positions.
DISCUSSION
Most of the professionals participating in the present study (79.4%) were female, corroborating the findings of studies carried out in primary care in Goiânia, (95.3%)10; (97.5%)11, a study carried out in a public hospital in the state of Paraná (74.8%)12, and a study carried out in a pediatric inpatient unit of a university hospital in the southern region of Brazil (92.31%)13. Initially, empirically, nursing care was developed by sisters of charity, having improved as a science over time, maintaining the profile of female predominance. Thus, this result was expected, since it is historically characteristic of the profession.
Regarding professional qualification, the largest number was nursing technicians (95.7%) and the majority of professionals working in the ICU presented age between 30 and 39 years, as found in a study carried out in a hospital in the state of São Paulo Paulo, in which the average age was 34.7 years14.
The nursing team's action period was 1 to 10 years in both, the institution and the unit (72.1% and 76.4%), respectively. Results found in a study carried out at the Neonatal ICU of a teaching hospital in Curitiba showed that 25% of the professionals worked less than one year11, different from that presented in the present study.
Only 33.3% of the nurses and 51.8% of the nursing technicians working in the ICU received training in the last two years on HH. The result obtained differs from other surveys carried out in hospitals in the state of Paraná, in which the majority of the nursing staff was trained, presenting educational action fees received of 87.5%11 and 94.8%12.
A study carried out in hospitals in the state of Paraná showed that 96.0% of the institutions performed training activities given to employees already hired, in which the nursing service was the most contemplated professional category. The most frequently addressed topic was HH (70.8%)15.
Considering the turnover of professionals, the constant presence of students and professors in academic activities, including the low adhesion to HH by the multi professional team, this theme should be addressed in all educational actions carried out, not only in the ICU, but in the whole hospital, study scenario. In the present research, it is inferred that the low index evidenced may be related to the undue importance given by the nursing professionals to the topic in question.
The lack of training and non-performance of training for the critical sector evidenced in this study emerges as a negative factor, considering the demand and creation of Quality Management Programs, which seeks strategies to improve the care actions developed, as well as safety of patients and health professionals.
It should be considered that being a care manager requires the nurse abilities of supervision of the care provided, and from this, the use of strategic tools for better results16. This study evidenced the need for actions to be implemented in order to boost the performance of HH10. In addition, a study comparing adhesion to practice before and after interventions, found an effectiveness in these actions with nursing technicians, presenting in the pre-intervention period 21.4% of HH performed and in the post-intervention period 28.9%, with an increase of the referred index6.
In a study carried out in an emergency department in São Paulo, the nursing team presented 31.2% of adhesion to HH practice before and 37.5% after intervention17. Likewise, a survey was carried out in 11 ICUs in general hospitals in Argentina, with nurses, physicians, pharmacists, physiotherapists, residents of the health area and radiology technicians, who estimated the effect of educational interventions on improving adhesion to HH, found higher rates (from 66.0% in the control group to 75.6% in the intervention group), as well as a greater impact in practice after contact with areas close to the patient18.
This fact, a qualitative study indicates that educational measures are considered important by the professionals of the nursing team, as well as their recognition of the necessity of adhesion to this practice in order to protect the user and the worker, as well as the control of HAIs11.
In the present study, the fact that adhesion to HH is less than 50% and lower among nursing technicians is worrying and requires attention from the sector coordination, considering that this professional is in continuous direct contact with patients8. It is also worth mentioning that the practice was not carried out before aseptic procedures by the nursing team, divergent results of research carried out in primary care, in which there was no HH after its completion in most of the procedures (vaccines, dressings, foot test, among others) as well as in 40.9% of these activities there was no previous and subsequent adhesion10. During the observations made in the present study, it was repeatedly observed that the use of gloves in this situation seemed to replace HH from the perspective of the professionals, which may be related to a lack of knowledge about the issue or the non-recognition of its importance. However, according to Rezende et al.10, practice is fundamental, both in the "before" moments, for patient safety and "after", mainly for the protection of the team.
The result found converges with those of other researches conducted, with an index of 43.7% (8); another, with a percentage of 12% for nurses and 11% for nursing technicians (7). However, the low index differs from the results presented in a study carried out in a municipal hospital and an Emergency Room in Minas Gerais, in which the rate of adhesion by nursing technicians was 83% (19). In addition, a study carried out in an ICU of a school hospital in London, based on the five moments for HH, indicated adhesion to the practice of HH of 60% (20).
The lower number of indications for HH by nurses (Table 2), as well as a small number of observations made with these professionals in this study, may be related to the great demand for administrative tasks in the unit, as already shown in another study carried out in a municipal hospital in Minas Gerais19. Still, the greater adhesion to HH by nurses, when compared to the nursing technicians evidenced in the present study, although not statistically significant (Table 4), converges with research carried out, in which the practice was not performed by nurses in three indications and by nursing technicians did not have adhesion in 60 indications 19.
Still, considering this context, the lower adhesion to HH by nursing technicians can infer a great workload, considering the complexity of patients in intensive care. Also, given the low levels of adhesion to HH by the team and generally the high demand of activities in these sectors, it is necessary to reflect if the nurses and nursing technicians of the present study are actually managing to work together, which directly reflects the supervision by the nurse, impacting the safety of patients and professionals.
The high quantitative indications for HH and reduced adhesion by the nursing team in the moments before the contact with the patient and after contact with areas close to the patient is disturbing, presenting greater adhesion in general to the moments "after", and lower in moments "before ". These results are in line with those of another study carried out in the ICU for adults in the state capital of Paraná, in which the adhesion rate before contact with patients was only 13% and before aseptic procedure was 7.8%, while after exposure risk to body fluids, 35% of HH indications were performed and after contact with patient and / or the environment, 46%7. Another investigation also pointed out how to perform procedures, ie, greater adhesion after (49.2%) compared to the moment before (18.8%)17.
Also, a study carried out in the ICU in the south of Brazil showed in its results that at the time before contact with the patient the rate of adhesion to the practice was 18.4%, before aseptic procedure 20.9%, after exposure risk to body fluids 55.6%, after contact with patient 58.9% and after contact with areas close to the patient 49.1%8. This result may be related to the lack of knowledge of the team about the moments recommended for the accomplishment of HH and also about the influence each one has in a concrete way in the care of the patients.
It was noticed in the data collection that the routine organization of the nursing team in the sector makes the adhesion to HH a "do-for-doing" practice, demanding clarity of its importance and professional culture change. The direct observations showed that, in the majority, the professionals perform HH mainly after a certain sequence of care, ignoring or not knowing the risks inherent to non-adhesion at the recommended moments, a fact affirmed by the result of the association between adhesion and non-adhesion to HH in the five recommended moments and the observed professional performed in the present study (Table 4), which did not indicate a significant statistical difference.
The health team needs to be aware that even in the execution of activities in which low risk is perceived, the spread of HAIs may occur20. According to Mota et al. 19, the agreement of the correct implementation of this practice mandates a change in the behavior of employees, which seems to be difficult to reach when health professionals, working in critical sectors, do not adhere to HH based on the recommended times, but according to their perception of the need.
Among the intervening factors that can influence the adhesion to HH, are the aspects related to the physical structure. In a study carried out, the number of stations to perform this practice that were fully operational and without access prevented was less than 50%7, results that corroborate with the findings of the present study, since there is not at all points of care of the unit, sinks, soap dispensers and paper towel. Likewise, in the beds where the necessary equipment and products are available, they are difficult to use because they are in close proximity to wires of monitors, infusion pumps and ventilators that make it difficult to approach professionals, a relevant factor that may possibly be interlinked to non-adhesion to HH.
It is important to point out that the assistance point is a meeting place for three elements: care, patient and health professional. Therefore, products for the practice of HH should be made available in this place, within reach or within the two-meter limit, in order to avoid the need for the employee to leave the patient's zone for action21. A research carried out show in its results among the factors that make it difficult to perform this action, the sink distance, inadequate sink and material deficit22. Considering the existing structure for HH in the studied ICU, it is inferred that the results can be in keeping with the reality of the nursing team participating in this research.
In this perspective, conditions for HH, as well as participation in the decisions, selection of priorities in the assistance of flexible way, are related to the motivation for the adhesion to HH by the professionals. However, the actual practice of this action depends on each professional23.
It is noticed that the nurse as manager of the care is certainly indispensable in the incentive to the adhesion of the practice of HH by the nursing team. Possibly, moments of discussion, raising the potential and difficulties of professionals, goal setting and constant evaluation of the results in the practice of care, using assertive tools and indicators, could have a positive impact on adhesion to HH by the nursing team of this research.
Therefore, it is necessary the interest of the managers and the joint work in the institution to achieve better results, recognizing the relevance of good practices in health, the importance of culture of institutional security, the reduction of costs and compliance of ethical and legal precepts.
As limitations of the study, it is possible to mention the non-registration in the instrument of data collection of the product used by the professionals for the HH during the observations, although it has been empirically perceived, greater adhesion to the practice with water and liquid soap; failure to observe the correct technique and removal of ornaments for HH, relevant to the evaluation of the actual effectiveness of the practice. As a fragility of the technique used, it is inferred that the Hawthorne Effect may have influenced the adhesion presented, since it refers to the behavioral change of the participants when observed24.
Still, it is suggested to carry out other studies on the subject, with new approaches that can contemplate the aforementioned aspects. It is believed that participant observation would be relevant as a method of investigation, so as to intervene at the moment of performing the actual care practice. Also, researches that aim to identify factors with influence on adhesion, from the perspective of professionals working in care, and that relate adhesion to HH to safety indicators and indicators of prevention and control of HAIs.
CONCLUSION
It was concluded that the adhesion to HH by the professionals of the nursing team of the studied ICU was very deficient, especially the moments before aseptic procedures and before the contact with the patient.
The presented results are worrisome, considering that nursing as a profession has the object of work care, provides direct assistance in an uninterrupted manner, which predisposes the occurrence of HAIs in critically ill, immunodepressed patients, usually with several invasive procedures, with multiresistant germs and associated risk factors.
Finally, it is expected that this study may subsidize practices of improvement in care, especially in the prevention and control of HAIs and adhesion to HH. In this endeavor, it is hoped that the nurse will lead the actions of improvement to the care, including in its role of manager of the assistance the monitoring of the adhesion to HH to the leverage of the patient security.
REFERENCIAS
1. Brasil. Ministério da Saúde/Anvisa/Fiocruz. Protocolo para a prática de higiene das mãos em serviços de saúde. [Internet] 2013. Disponível emhttp://www.hospitalsantalucinda.com.br/downloads/prot_higiene_das_maos.pdf. [ Links ]
2. Organização Pan-Americana da Saúde. Agência Nacional de Vigilância Sanitária. Manual para observadores: estratégia multimodal da OMS para a melhoria da higienização das mãos. Brasília: Organização Pan-Americana da Saúde. [Internet] 2008. Disponível em: http://www.anvisa.gov.br/servicosaude/controle/higienizacao_oms/manual_para_observadores-miolo.pdf. [ Links ]
3. Kelly D, Kutney-Lee A, Lake ET, Aiken LH. The critical care work environment and nurse-reported health care-associated infections. Am J CritCare. [Internet] 2013; 22(6):482-8. Disponível em: http://ajcc.aacnjournals.org/content/22/6/482.full.pdf+html. [ Links ]
4. Melo MHC, Leal ACAM. Controle das infecções na assistênciaà saúde relacionada à higienização das mãos. R. Interd. [Internet] 2015; 8(1): 91-7. Disponível em: http://revistainterdisciplinar.uninovafapi.edu.br/index.php/revinter/article/view/351/pdf_187. [ Links ]
5. Calil K, Valente GSC, Silvino ZR. Acciones y/o intervenciones de enfermería para laprevención de infecciones hospitalariasen pacientes gravemente enfermos: una revisión integrativa. Enfermería Global. [Internet] 2014;13(2):406-24. Disponível em: http://revistas.um.es/eglobal/article/view/156491/160761. [ Links ]
6. Prado MF, Oliveira AC, Nascimento TMB, Melo WA, Prado DB. Estratégia de promoção à higienização das mãos em unidade de terapia intensiva. CiencCuidSaude. [Internet] 2012 Jul/Set; 11(3):557-64. Disponível em: http://eduem.uem.br/ojs/index.php/CiencCuidSaude/article/view/16366/pdf. [ Links ]
7. Bathke J, Cunico PA, Maziero ECS, Cauduro FLF, Sarquis LMM, Cruz EDA. Infraestrutura e adesão à higienização das mãos: desafiosà segurança do paciente. Rev Gaúcha Enferm. [Internet] 2013;34(2):78-85. Disponível em: http://www.scielo.br/pdf/rgenf/v34n2/v34n2a10.pdf. [ Links ]
8. Souza LM, Ramos MF, Becker ESS, Meirelles LCS, Monteiro SAO. Adesão dos profissionais de terapia intensivaaos cinco momentos da higienização das mãos. Rev Gaúcha Enferm. [Internet] 2015 dez;36(4):21-8. Disponível em: http://www.seer.ufrgs.br/RevistaGauchadeEnfermagem/article/viewFile/49090/35654. [ Links ]
9. Agência Nacional de Vigilância Sanitária (ANVISA). Assistência Segura: Uma Reflexão Teórica Aplicada à Prática. Série Segurança do Paciente e Qualidade em Serviços de Saúde. Brasília; [Internet] 2013. Disponível em: http://www20.anvisa.gov.br/segurancadopaciente/images/documentos/livros/Livro1-Assistencia_Segura.pdf. [ Links ]
10. Rezende KCAD, Tipple AFV, Siqueira KM, Alves DB, Salgado TA, Pereira MS. Adesão à higienização das mãos e ao uso de equipamentos de proteção pessoal por profissionais de enfermagem na atenção básica em saúde. CiencCuidSaude. [Internet] 2012 Abr/Jun; 11(2):343-351. Disponível em: http://ojs.uem.br/ojs/index.php/CiencCuidSaude/article/viewFile/15204/pdf. [ Links ]
11. Guedes M, Miranda FMD, Maziero ECS, Cauduro FLF, Cruz EDA. Adesão dos profissionais de enfermagem à higienização das mãos: uma análise segundo o modelo de crenças em saúde. CogitareEnferm. [Internet] 2012;17(2);304-9. Disponível em: http://revistas.ufpr.br/cogitare/article/view/27886/18494. [ Links ]
12. Giordani AT, Sonobe HM, Ezaias GM, Valério MA, Andrade D. Adesão da enfermagem à higienização das mãos segundo os fatores higiênicos de herzberg. Revenferm UFPE online. [Internet] 2016 fev; 10(2):600-7. Disponível em: http://www.revista.ufpe.br/revistaenfermagem/index.php/revista/article/downlod/8495/14274. [ Links ]
13. Silva FM, Porto TP, Rocha PK, Lessmann JC, Cabral PFA, Schneider KLK. Higienização das mãos e a segurança do paciente pediátrico. Cienc. Enferm. [Internet] 2013; 19(2):99-109. Disponível em: http://www.scielo.cl/pdf/cienf/v19n2/art_10.pdf. [ Links ]
14. Santos TCR, Roseira CE, Piai-Morais TH, Figueiredo RM. Higienização das mãos em ambiente hospitalar: uso de indicadores de conformidade. Rev Gaúcha Enferm. [Internet] 2014 mar;35(1):70-7. Disponível em: http://seer.ufrgs.br/index.php/RevistaGauchadeEnfermagem/article/view/40930/28935. [ Links ]
15. Alves DCI, Lacerda RA. Avaliação de Programas de Controle de Infecção relacionada a Assistência à Saúde de Hospitais.Rev. esc. enferm. USP [Internet]. 2015; 49(spe):65-73. Disponível em http://dx.doi.org/10.1590/S0080-623420150000700010. [ Links ]
16. Inoue KC, Matsuda LM. Segurança do paciente: abordando um antigo problema. CiencCuidSaude. [Internet] 2013; 12(2): 208-9. Disponível em: http://eduem.uem.br/ojs/index.php/CiencCuidSaude/article/view/23880/13023. [ Links ]
17. Trannin KPP, Campanharo CRV, Lopes MCBT, Okuno MFP, Batista REA. Adesão à higiene das mãos: intervenção e avaliação. CogitareEnferm. [Internet] 2016 Abr/jun; 21(2): 01-07. Disponível emhttp://revistas.ufpr.br/cogitare/article/view/44246/28015. [ Links ]
18. Rodriguez V, et al. A multimodal intervention to improve hand hygiene in ICUs in Buenos Aires, Argentina: a stepped wedge trial. Int J Qual Health Care. [Internet] (2015); 27(5):405-11. Disponível em: https://academic.oup.com/intqhc/article-lookup/doi/10.1093/intqhc/mzv065. [ Links ]
19. Mota EC, Barbosa DA, Silveira BRM, Rabelo TA, Silva NM, Silva PLN, Ribeiro JL, Silva CSO, Gonçalves RPF. Higienização das mãos: uma avaliação da adesão e da prática dos profissionais de saúde no controle das infecções hospitalares. RevEpidemiolControlInfect. [Internet] 2014;4(1):12-7. Disponível em: https://online.unisc.br/seer/index.php/epidemiologia/article/view/4052/3379. [ Links ]
20. FitzGerald G, Moore G, Wilson APR. Hand hygiene after touching a patient's surroundings: the opportunities most commonly missed. Journal of Hospital Infection. [Internet] 2013; 84:27-31. Disponível em: http://www.journalofhospitalinfection.com/article/S0195-6701(13)00048-0/pdf. [ Links ]
21. Agência Nacional de Vigilância Sanitária (ANVISA). Segurança do Paciente: Relatório sobre Autoavaliação para Higiene das Mãos. [Internet] 2012. Disponível em: http://www.saude.goiania.go.gov.br/library_source/relatorio_de_avaliacao.pdf. [ Links ]
22. Silva BV, Cardoso CMS, Nascimento SMC, Madeira MZA. Adesão da higienização das mãos por profissionais de saúde em unidade de terapia intensiva neonatal. RevEnferm UFPI. [Internet] 2013 Jan-Mar; 2(1):33-7. Disponível em: http://www.ojs.ufpi.br/index.php/reufpi/article/viewFile/863/pdf. [ Links ]
23. Giordani AT, Sonobe HM, Ezaias GM, Valério MA, Andrade D. The nursing team's compliance with hand hygiene: motivational factors. Rev Rene. [Internet] 2014 jul-ago; 15(4):559-68. Disponível em: http://www.revistarene.ufc.br/revista/index.php/revista/article/view/1567/pdf_1. [ Links ]
24. Oliveira AC, Gama CS. Antissepsia cirúrgica e utilização de luvas cirúrgicas como potenciais fatores de risco para contaminação transoperatória. Esc Anna Nery. [Internet] 2016; 20(2):370-77. Disponível em: http://www.scielo.br/pdf/ean/v20n2/1414-8145-ean-20-02-0370.pdf. [ Links ]
Received: December 22, 2016; Accepted: April 30, 2017
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
