










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.17 no.51 Murcia jul. 2018 Epub 01-Jul-2018
https://dx.doi.org/10.6018/eglobal.17.3.289541
Originals
Anxiety in primary care nursing technicians
1 Licenciada en Enfermería por la Universidad Federal da Paraíba. Miembro del Grupo de Investigación y Extensión Sinapsis y Ansiedad- CCS/UFPB. Brasil. bruna_2292fernandes@hotmail.com
2 Alumno de doctorado por el Programa de Postgraduación en Desarrollo e Innovación Tecnológica PPGDITM/UFPB. Licenciada em Enfermería por la Universidad Federal da Paraíba. Miembro del Grupo de Investigación y Extensión Sinapsis y Ansiedad - CCS/UFPB. Brasil.
3 Alumna de Máster del Programa de Postgraduación en Neurociencia Cognitiva Comportamiento - PPGNeC/UFPB. Licenciada en Enfermería por la Universidad Federal da Paraíba. Miembro del Grupo de Investigación y Extensión Sinapsis y Ansiedad- CCS/UFPB.Brasil.
4 Alumna de Doctorado del Programa de Postgraduación Modelos y Decisión en Salud PPGMDS/UFPB. Licenciada en Enfermería por la Universidad Federal de Paraíba. Miembro del Grupo de Investigación y Extensión Sinapsis y Ansiedad - CCS/UFPB. Brasil.
5 Doctor en Farmacología por el Programa de Postgraduación en Productos Naturales y Sintéticos Bioactivos de la Universidad Federal de Paraíba. Profesor de la Universidad Federal de Paraíba. Coordinador del Grupo de Investigación y Extensión Sinapsis y Ansiedad - CCS/UFPB. Brasil.
Objective
To evaluate the level of anxiety in nursing technicians of the Family Health Strategy, emphasizing the determinant aspects for the emergence of anxiety.
Method
A descriptive, cross-sectional, quantitative approach, consisting of 28 Nursing Technicians, using the State-Trait Anxiety Inventory (STAI) as an instrument for data collection.
Results
Eight nursing technicians presented levels of high anxiety and 20 of low anxiety. There was an increase in the S-Anxiety Scale score during the activities, with statistical difference in relation to the moment before. The low remuneration, work overload and professional devaluation were pointed out as factors responsible for provoking the appearance of anxiety within the scope of work.
Conclusion
The study evidences a predominance of low anxiety among the study population; however, it was possible to detect factors triggering the anxiety, pointing out that such aspects may come to harm the peculiarity of the assistance to the user.
Keywords Anxiety; Basic Attention; Nursing technicians
INTRODUCTION
The Family Health Strategy (FHS), gateway to the Unified Health System, which corresponds to the services of Primary Care (PC), aims to reorganize primary health care with integral attention to the individual and collective users, offering services of disease prevention, health promotion and rehabilitation in the face of a specific problem through an accurate diagnosis. The FHS works in conjunction with sanitary and epidemiological surveillance to minimize harm, promote and protect the health of the population according to their needs, as well as perform family planning and develop health education actions1)(2)(3.
The nursing team that acts in the PC is composed of three types of professionals, the nurse, nurse technician and nursing assistant, who must work collectively in order to achieve the goals required by the government with the goal of maintaining and producing health4.
The Nursing Technician performs primary functions for the operation of the Basic Health Unit (BHU) and that require a great deal of involvement, among which may be highlighted: to be part of activities in the unit and if necessary at home or in community settings; develop programmed and demand-driven actions; implement health education practices in accordance with planning; to be present in the administration of the necessary resources for the unit; and to collaborate with lifelong education2)(3.
The health of the worker has become a constant concern due to the occupational risks that are exposed. Health professionals, especially nursing professionals, who act in direct contact with the population are more likely to develop diseases, whether physical or emotional. The routine they face involves a number of burdensome factors, such as population demands, service or staff failure, lack of material and human resources, environmental conditions and exacerbation of the work place, among other factors. This makes these professionals demand more of themselves, causing fatigue of the body and mind, and consequently allowing the intercurrence of health problems and the development of feelings such as anguish and anxiety5.
Anxiety disorders have been frequently present today, although it is already a subject reported in history. Anxiety is a psychic state characterized by emotional oscillations in which physiological components are present in conjunction with psychological ones affecting human behavior in certain situations. It is highlighted as normal as the emitted reaction becomes harmonious to the triggering stimulus of affliction. It becomes pathological from the moment when the circumstance it is causing is disproportionate, or when there is no motive to which it is directed, becoming harmful, characterizing itself as a disorder6)(7.
Anxiety can be classified as anxiety-trait and anxiety-status. The first is personality, being therefore stable, and the second refers to the emotional state, which changes over time and encompasses feelings of tension, nervousness, and concerns about variations according to the intensity of the danger identified8 .
This study aimed to evaluate the level of anxiety in nursing professionals of the FHS, emphasizing the main determining factors for the emergence of anxiety and its relationship with the variables: age and length of service.
MATERIAL AND METHODS
Study design, population and sample
This is a cross-sectional descriptive study with a quantitative approach, developed with Nursing Technicians that make up the FHS of the Family Health Units of a Sanitary District of the municipality of João Pessoa- PB. The sample consisted of 28 Nursing Technicians who accepted to participate in the study by signing the Informed Consent Form (ICF) and met the eligibility criteria: Being a Nursing Technician, working in the FHS for more than two months, not making use of anxiolytic substance, and is not being subjected to any types of anxiety therapy.
Instruments for data collection
Initially, a semi-structured questionnaire was applied, developed by the researchers to characterize the sample and its relation with the study variables. The questionnaire included questions aimed at investigating the relationship between anxiety presented by the Nursing Technicians and the variables: age range and length of service.
In order to evaluate the Anxiety of Nursing Technicians, we used the State-Trait Anxiety Inventory (STAI), which consists of two self-assessment sub-scales: the STAI-Trait (STAI-T) and the STAI-State (STAI-S).
The State-Trait Anxiety Inventory (STAI), elaborated in 1970 by Spielbergeret al9, is an instrument translated and validated to the Portuguese language by Biaggio et al. In 197910. The STAI-T evaluates the reaction of the individual in situations of danger, and, therefore, allows the knowledge of the trait of anxiety. The STAI-S evaluates anxiety at a specific time, presenting variations according to the situation faced. They each consist of 20 questions, with four possible intensity of response, ranging from 1 to 4, the scores added by each volunteer oscillate between 20 and 80 points. The scores presented by the evaluated population below 40 points were assigned to the group judged with low anxiety (LA) and those who obtained scores above 41 were assigned to the high anxiety group (HA)11.
Procedures for data collection
At the first moment, the semi-structured questionnaire and the STAI-T were applied to evaluate the level of anxiety of the Nursing Technician. The STAI-S was used during the three moments of the development of the work process:
1st moment: before the start of their care activities, when the nurse prepares to initiate the care tasks.
2nd moment: two hours after the start of activities, time considered intermediate during the course of a shift.
3rd moment: fifteen minutes after the completion of the activities of the research participants.
After the measurement of the STAI-S at the last mentioned time, the questionnaire was applied on the factors considered by these professionals as anxiety triggers.
Statistical analysis
For the descriptive and analytical statistical analysis of the data, the program GraphPadPrism (version 4.00, GraphPad Software Inc., San Diego, CA, USA) was used. The Kruskal-Wallis test and the Dunns post-test were performed for non-parametric variables. The results were considered significant when they presented a level of significance of 95% (P <0.05).
Ethical aspects
The research was approved from the CAAE No. 47766815.9.0000.5188 of the Ethics and Research Committee of the Health Sciences Center of the Federal University of Paraíba, in compliance with Resolution No. 466/2012 of the National Health Council, which regulates the conduct of research involving human beings.
RESULTS
The results obtained refer to the levels of anxiety-trait and anxiety-state measured through the STAI-T and STAI-S instruments applied to the 28 nursing technicians who work in the FHS in a sanitary district of the municipality of João Pessoa-PB.
When analyzing the level of anxiety-trait, these professionals presented a median value of 30 points. As for the distribution of low anxiety levels (LA) and high anxiety (HA), it was found that 8 nursing technicians presented high anxiety level, representing 28.57% of the sample, while 20 subjects were categorized with low levels of anxiety (71.43%), predominating the LA, according to Table 1.
Table 1 Classification of Nursing Technicians according to the trace and median level of the STAI-T score. João Pessoa - 2016.

Source: Research data.
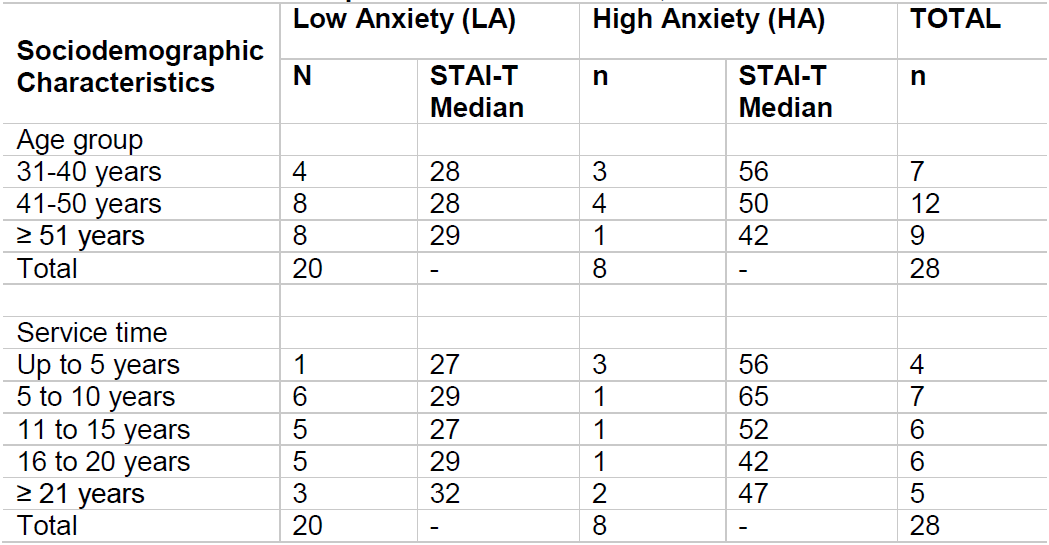
By correlating the median STAI-T with the age group of the professionals, it is observed that LA was predominant in all age groups. Among Nursing Technicians who were over 51 years old, only a single subject presented HA. The highest value of the identified median of the group categorized as HA was the age group of 31 to 40 years old, with a value of 56 points, as represented in Table 2.
When the median of the anxiety trait according to length of service is presented, it can be identified that the group of up to 5 years of service time has a higher concentration of subjects classified with HA, while in the remaining delimited periods of service, LA predominates.
Table 2 Median of the STAI-T distributed according to sociodemographic characteristics of the Nursing Technicians and according to the levels of anxiety presented. João Pessoa, 2016.
Source: Research data.
In the evaluation of the level of anxiety-state, we measured the STAI-S score medians measured at the moments of the work process: before the beginning of the working day (first moment), during the working day (second moment) and after (third moment), as demonstrated in Table 3. In the first moment, the professionals presented a median score of 23 points (Min: 20; Max: 47), during the work, the median value increased to 31 points (Min: 21; Max: 54), and at the end of activities the median was 29 points (Min: 20; Max: 41). This demonstrates a significant difference between the moments before and during the professional's work (p-value - 0.0151).
Table 3 Comparison of Medians (minimum and maximum) of STAI-S scores between the moments before, during and at the end of the professionals' activities. João Pessoa, 2016.

Source: Research data. Kruskal-Wallis statistical test and Dunns post-test. *Significantly different at the moment before.
The Nursing Technicians listed some factors considered to be anxiety triggers within the work process (Table 4). Each professional had autonomy granted to cite the factors that they considered pertinent.
Therefore, it can be emphasized: low remuneration, followed by work overload, professional devaluation, and compromised physical structure, were also cited excessive demand, excessive bureaucracy and other factors.

DISCUSSION
The present study demonstrated that according to the parameters stipulated for classification of the degree of anxiety and according to the analysis of the results of the STAI-T scores, the Nursing Technicians were classified with low anxiety. However, professionals who were categorized with high level of anxiety, have presented a result considered relevant to the clinical view, considering the effects that the aggravations to the psychic health of these professionals can cause in their personal lives, daily activities, in the work scope, in their social and interprofessional relationships, as well as in the care given to the community12.
These results corroborate findings from a study that evaluated 17 health professionals, and of these, only 4 presented a high level of anxiety. The results, however, were considered significant by the author, considering the possible consequences of pathological anxiety in personal and professional life of these individuals13. In research made, 2% of the professionals indicated a high level of anxiety, and the authors report that this figure is identified as high, since 25% of these individuals may acquire Generalized Anxiety Disorder (GAD) as the main diagnosis14.
In one study, the results presented demonstrate that individuals with altered levels of anxiety are present since graduation in nursing. These showed that 12% of the studied sample presented severe anxiety, stressing the importance of identifying and treating this problem, since this can significantly affect the construction of the student's identity as well as his quality of life15.
The individual diagnosed with GAD has little viability of a spontaneous remission, and there may be an increase in the probability of this disorder becoming chronic, or even provoking the appearance of new psychiatric disorders, if it does not have an effective treatment12. In study, it was found that these considerations lead not only to damages to workers' health, but also to the health of the population, as they suffer from consequences arising from the suffering of the professionals, thus making them propagators of anxiety16.
When comparing the results of the STAI-T scores with the age group, it can be observed that regardless of the compatibility in the values of the median, younger professionals tend to present an anxious profile, since they presented the highest level of anxiety in relation to professionals with greater age.
Such results corroborate findings in studies that show that younger professionals are more likely to manifest anxiety in relation to older workers17. Research performed showed that nursing professionals who were elderly were satisfied and fulfilled personally, presenting low levels of emotional stress and for this reason, anxiety levels were low18.
A nursing professional, when obsolete, develops a debilitation of physical force and a deficit in the work done, as a result of which the quality of the care provided to the patient suffers a direct impact. Some measures must be taken in relation to these professionals, such as: recognition at work, favorable working hours, economic incentives, less strenuous jobs and ergonomic measures in the workplace19.
When comparing the results of the STAI-T scores with the length of service, it can be observed that professionals who have a service time of up to 5 years had a higher level of anxiety, while those with superior service time, predominated with a low level of anxiety. These outcomes corroborate with the results of the study, in which the professionals with the highest anxiety level values are those with a professional experience of less than five years. The authors report that this episode may be related to the current situation of the nursing profession (greater professional instability, particularities of contracts, among others), to assume new responsibilities in the face of greater insecurity of their actions, due to the low professional experience and high experience expected to enter the labor market18.
When analyzing the level of anxiety-state from the results of the STAI-S scores, during the three moments of the study, before, during and at the end of the activities of the Nursing Technicians, it was verified that between the first and the second moment there was a significant variation at the statistical level. At the beginning of the activities, the professionals presented a low level of anxiety, and then during the work, this level increased, surpassed the previous moment. Subsequently, at the end of the activities the anxiety had a reduction. It was identified that it is during the work process that the professionals presented a higher level of anxiety.
In a study carried out, the professionals of the study showed a high level of anxiety during the work process13. It is evident that the impact of professional exercise during the shift has been provoking disturbances in the quality of life, in the biological rhythms and in the physical and mental health of these workers, generating obstacles in the harmonization of family and social life18.
Stress during the workday is associated with unfavorable circumstances and environments for the development of nursing professional assignments. Often times, the workers, when confronted with their neighbor's pain and the anguish of family members, take on a great emotional overload, and when they give their assistance to these individuals, they end up neglecting their own health and consequently impair their social life and working environment16)(20.
Although there is no variation with a degree of statistical significance (p value <0.05) between the second and third moments, the existence of a clinical significance in the decrease of the anxiety present between these moments cannot be overlooked, factor identified when confronted with the results of the STAI-S scores. Returning home or even going to other places of personal liking at the end of the workday of the professionals may be associated with the fact that the level of anxiety is less intense after the shift, thus indicating that this aspect may work as a reducing principle of anxiety21)(16.
Regarding the factors highlighted by the professionals as triggers of anxiety in the scope of work, one can verify daily exposure to circumstances of high emotional exigency that the nursing professionals are submitted, causing physical and mental exhaustion. Factors such as excessive bureaucracy, overwork and excessive demand were also emphasized by the professionals of Primary Care in a research made13. The demands of the professional environment exceed the physical or psychic capacities of the worker, generating dysfunction in the health of these individuals22.
Authors sought to identify favorable and impeding factors to the satisfaction of Nursing Technicians in the scope of work and according to their results, the impeding factors overlapped the favorable ones, thus generating barriers for self-care and consequently bringing demotivation and damages to the workers' health19.
According to a study carried out, the low salaries appear as a demotivating aspect to the worker, in which it makes this factor significant from the point of view of mental health. In their results, it was verified that the prevalence of anxiety episodes is more related to the monthly income, and in the time when the income variable decreased, the professionals were more anxious17. The work overload is the category most cited by nursing professionals, pointing out that 47.6% of these feel overwhelmed in relation to the activities they carry out in their daily lives22.
The appreciation of the Nursing Technician and the recognition for his or her work performed are of great significance, since the professional will feel motivated to carry out his activities with quality, as well as stimulate him in the pursuit of a humane care, and in the ascendancy of their self-esteem, thus leading to a decrease in the level of anxiety16.
Care for the human being is the essence and specificity of nursing, a primordial principle for the team that makes up this profession. However, often these workers are susceptible to improper work conditions, such as long hours, overwork, devaluation of the professional, insufficient resources, low pay, among others. These aspects affect the professional daily, inducing them to perform their service mechanically and inhibiting the development of their duties with competence and ability, thus directly reflecting the assistance provided to the user and the community as a whole16)(18.
CONCLUSIONS
The study shows that there was a predominance of the low level of anxiety-trait among the studied population, but with a relevant number of individuals with high anxiety. It was verified that according to the STAI-S scores, there was a significant increase in the level of anxiety-state during the nursing technicians’ work process, characterizing it as an anxiogenic moment.
The factors highlighted by the nursing technicians as triggers of anxiety may be correlated with the high levels of anxiety pointed out in the STAI scores, allowing the hypothesis that such aspects may be detrimental to the care given to the user and the community.
In view of these outcomes, there is a need for greater attention from supervisors towards these professionals, allowing them to guarantee favorable working conditions and the implementation of non-pharmacological strategies in the work environment of these with anxiogenic profiles, such as, Integrative Community Therapy (ICT), work gymnastics, music therapy, among others, as methods of coping with this anxiety.
REFERENCIAS
1. Souza DP, Silva GA, Paula EMJ. Atividades do técnico e do auxiliar de enfermagem numa unidade de clínica médica de um Hospital Universitário. EFDeportes Rev. Digital [Internet]. 2013; 15(166). [ Links ]
2. Ministério da Saúde (BR). Política Nacional de Atenção Básica. Brasília: Ministério da Saúde; 2006. [ Links ]
3. Ministério da Saúde (BR) - GABINETE DO MINISTRO. Portaria nº 2.488, de 21 de outubro de 2011. Brasília: Ministério da Saúde; 2011. [ Links ]
4. Moura GMSS, Inchauspe JAF, Agnol CMD, Magalhães AMM, Hoffmeister LV. Expectativas da equipe de enfermagem em relação à liderança. Acta paul. enferm.[Internet]. 2013; 26(2): 198-204. [ Links ]
5. Castilho CRN. A relação do processo de trabalho de enfermagem com o adoecimento desses profissionais: uma pesquisa bibliográfica [Monografia]. Rio Grande do Sul: Universidade Federal do Rio Grande do Sul; 2010. [ Links ]
6. Díaz Tobajas MC, Juarros Ortiz N, García Martínez B, Sáez Gavilán C. Estudio de la ansiedad del profesional de enfermeria de cuidados intensivos ante el proceso de la muerte. Enfermeria Global. 2007; 45: 246 - 255. [ Links ]
7. Andrade A, et al. Ansiedade associada a fatores sociodemográficos e clínicos de mulheres com síndrome da fibromialgia. Rev. dor[Internet]. 2013; 14(3): 200-203. [ Links ]
8. Nardi AE, Fontenelle LF, Crippa JAS. Novas tendências em transtornos de ansiedade. Rev. Bras. Psiquiatr.[Internet]. 2012; 34(1): 5-6. [ Links ]
9. Ries F, Vazquez CC, Mesa MCC, Andres OC. Relações entre ansiedade-traço e ansiedade-estado em competições esportivas. CPD[Internet]. 2012; 12(2): 9-16. [ Links ]
10. Spielbergert CD, Gorsuch RI, Lushene RE. Manual for the State-Trait Anxiety Inventory. Ca: Palo Alto Consulting Psychologists Press; 1970. [ Links ]
11. Biaggio AMB, Natalício L. Manual para o Inventário de Ansiedade Traço-Estado (IDATE). Rio de Janeiro: Centro Editor de Psicologia Aplicada (CEPA); 1979. [ Links ]
12. Almeida AAF, Behlau M, Leite JR. Correlação entre ansiedade e performance comunicativa. Rev. Soc. Bras. Fonoaudiol.[Internet].2011; 16(4): 384-389. [ Links ]
13. Sousa DA, Moreno AL, Gauer G, Manfro GG, Koller SH. Revisão sistemática de instrumentos para avaliação de ansiedade na população brasileira. Aval. Psicol. [Internet]. 2013; 12(3): 397-410. [ Links ]
14. Chaves Neto G, Braga JEF, Diniz MFFM,et al. Avaliação da Ansiedade em Enfermeiros da Atenção Básica. Revenferm UFPE online [Internet]. 2014; 8(12): 4345-52. [ Links ]
15. Gomes RK, Oliveira VB. Depressão, ansiedade e suporte social em profissionais de enfermagem. Bol. Psicol. [Internet]. 2013; 63(138): 23-33. Disponível em: http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S0006-59432013000100004&lng=pt&nrm=iso. [ Links ]
16. Marchi KC, Bárbaro AM, Miasso AI, Tirapelli CR. Ansiedade e consumo de ansiolíticos entre estudantes de enfermagem de uma universidade pública. Rev. Eletr. Enf. [Internet]. 2013;15(3):731-739. Disponível em: http://dx.doi.org/10.5216/ree.v15i3.18924 [ Links ]
17. Duarte MLC, Avelhaneda JC, Parcianello RR. A saúde do trabalhador na estratégia de saúde da família: percepções da equipe de enfermagem. Cogitareenferm[Internet]. 2013; 18(2): 323-330. Disponível em: http://bases.bireme.br/cgi-bin/wxislind.exe/iah/online/?IsisScript=iah/iah.xis&src=google&base=LILACS&lang=p&nextAction=lnk&exprSearch=698908&indexSearch=ID. [ Links ]
18. Schmidt DRC, Dantas RAS, Marziale MHP. Ansiedade e depressão entre profissionais de enfermagem que atuam em blocos cirúrgicos. Rev. Esc. Enferm. USP [Internet]. 2011; 45(2): 487-493. Disponível em: http://www.revistas.usp.br/reeusp/article/view/40726/44015. [ Links ]
19. Oliveira V, Pereira T. Ansiedade, depressão e burnout em enfermeiros: Impacto do trabalho por turnos. Rev. Enf. Ref. [Internet]. 2012; 3(7): 43-54. Disponível em: http://www.scielo.mec.pt/scielo.php?script=sci_arttext&pid=S0874-02832012000200005&lng=pt&nrm=iso. [ Links ]
20. Forte ECN, Trombetta AP, Pires DEP, Gelbcke FL, Lino MM. Abordagens teóricas sobre a saúde do trabalhador de enfermagem: revisão integrativa. CogitareEnferm.[Internet]. 2014; 19(3). Disponível em: http://ojs.c3sl.ufpr.br/ojs/index.php/cogitare/article/view/35379. [ Links ]
21. Ribeiro RP, Martins JT, Marziale MHP, Robazzi MLCC. O adoecer pelo trabalho na enfermagem: uma revisão integrativa. Rev. Esc. Enferm. USP[Internet]. 2012; 46(2): 495-504. Disponível em: http://bases.bireme.br/cgi-bin/wxislind.exe/iah/online/?IsisScript=iah/iah.xis&base=LILACS&nextAction=lnk&lang=p&indexSearch=ID&exprSearch=625162&label=O%20adoecer%20pelo%20trabalho%20na%20enfermagem:%20uma%20revis%E3o%20integrativa. [ Links ]
22. Loureiro LMJ, Gameiro MGH. Interpretação crítica dos resultados estatísticos: para lá da significância estatística. Rev. Enfer. Refer.[Internet]. 2011; 3(3): 151-162. Disponível em: http://www.scielo.oces.mctes.pt/pdf/ref/v3n3/v3n3a16.pdf. [ Links ]
23. Meneghini F, Paz AA, Lautert L. Fatores ocupacionais associados aos componentes da síndrome de Burnout em trabalhadores de enfermagem. Texto and Contexto Enfermagem [Internet]. 2011; 20(2): 225. Disponível em: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-07072011000200002. [ Links ]
Received: March 23, 2017; Accepted: April 30, 2017
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
