










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.17 no.51 Murcia jul. 2018 Epub 01-Jul-2018
https://dx.doi.org/10.6018/eglobal.17.3.286181
Originals
Association between hospitalization due to diabetes mellitus and diabetic foot amputation
1 Doctorando del Programa de Postgraduación Cuidados Clínicos en Enfermería y Salud de la Universidad Estadual do Ceará. Bolsista Coordinación de Perfeccionamiento de Personal de Niível Superior. Fortaleza, Ceará, Brasil. antonio-dean@hotmail.com
2 Doctora en Enfermería. Profesora Adjunta de la Universidad Estadual do Ceará. Fortaleza, Ceará, Brasil.
3 Doctor en Educación. Profesor Adjunto de la Universidad Estadual do Ceará. Fortaleza, Ceará, Brasil.
Objective:
To analyze the association between the number of people hospitalized for diabetes and the number of people with limb amputation.
Method:
This is an ecological study using the Hospital Information System of the Unified Health System (SIH / SUS) from 2010 to 2015 in the state of Ceará, Brazil. The data were analyzed by the Statistical Package for the Social Sciences (SPSS). Pearson's linear correlation coefficient was applied to measure the intensity of the linear association between the variables.
Results:
There were 27,054 hospital admissions for diabetes. There was an inverse correlation between the number of admissions for treatment of diabetes and proportional correlation of the number of hospitalizations for complicated foot treatment and hospitalization for limb amputations.
Keywords: Amputation; Diabetic Foot; Hospitalization; Ecological Studies
INTRODUCTION
Chronic no communicable diseases (CNCDs) are a serious global health problem due to their morbidity and mortality. Around 36 million deaths worldwide (63%) are estimated to be due to CNCDs annually, with emphasis on diseases of the circulatory system, diabetes, cancer and chronic respiratory disease1.
Among these, diabetes mellitus (DM) stands out, which is expected to reach 640 million people globally between the ages of 20 and 79 by 20402, which makes it one of the most prioritized chronic diseases at the global level1. In addition, it leads to the onset of vascular diseases that have serious consequences for different target organs, such as heart, brain, kidneys and peripheral circulation of lower limbs (3.
Among the common complications of DM there is the diabetic foot, which exacerbates the quality of life of the individuals affected. It is estimated that about 20% of the total diabetic population develops foot problems, 5-10% foot ulcers and up to 3% acquire a history of amputations due to the disease4. In the United States, approximately 6% of the population was diagnosed with DM and 15% of these clients are expected to develop foot ulceration, and 14% to 20% of cases may require amputation5.
Diabetic foot infections are often complicated by numerous other medical comorbidities, which may rapidly evolve to limb loss, and the etiology of the lesions is multifactorial. Arterial insufficiency and neuropathy are the main risk factors and leave the person with diabetes more susceptible to infection, injury and non-healing of the limb. These strata correspond to 15% of the ulceration rate in diabetics, and 20% result in amputation6. Added to these factors there are the increase in age, duration of diabetes, lack of education and previous retinopathy, which leave the foot at risk7. People with diabetic foot are up to 60% more likely to have a second limb amputation within five years after the first one6.
Diabetic foot is defined by the International Working Group on the Diabetic Foot - IWGDF8 as infection, ulceration and/or destruction of soft tissues associated with neurological changes and various degrees of peripheral arterial disease (PAD) in the lower limbs.
The rates of foot ulcer and amputation are different in each region. The study of epidemiological data supports the formulation of regional health policies, as it shows the rate of neurological and vascular impairment in feet of patients with diabetes, besides guiding preventive interventions9. Thus, early detection is a way to reduce the severity of complications, including avoidable amputations7)(10.
Diabetic foot is as a serious collective health problem that can lead to amputation of lower limbs, causing disability, exacerbation of disability and early retirement, besides a large financial impact on government budgets.
Based on this context, the purpose of this study was to analyze the association between the number of people hospitalized for diabetes mellitus and the number of people who underwent limb amputation.
METHOD
This is an ecological study carried out in the state of Ceará, Brazil, with the number of hospital admissions due to DM and amputation of limbs from 2010 to 2015.
The data were accessed through the Hospital Information System of the Unified Health System (SIH/SUS), using the TAB program for Windows (TabWin) developed by the Department of Information Technology of SUS (Datasus), which has the purpose of allowing the teams of the Ministry of Health and State and Municipal Health Secretariats to carry out rapid tabulations on DBF files.
The variables chosen for analysis were: treatment of DM and complicated diabetic foot (independent variables) and amputation/disarticulation of lower limbs and amputation/disarticulation of foot and tarsus (dependent variables).
A priori, the data were typed and stored in Microsoft Excel 2010 software in double typing. Subsequently, the database was exported to the Statistical Package for the Social Sciences (SPSS), version 20.0.
Quantitative variables were presented by mean and standard deviation (M ± SD). In order to calculate the intensity of the linear association between the variables, Pearson's linear correlation coefficient (r) was applied, which is a measure of the degree of linear relationship between two quantitative variables. This coefficient varies between -1 and 1. The value 0 (zero) means that there is no linear relationship, the value 1 indicates a perfect linear relationship and the value -1 also indicates a perfect, but inverse, linear relationship, that is, when one of the variables increases the other decreases. The closer it is to 1 or -1, the stronger the linear association between the two variables. A significant trend was considered when its estimated model reached p <0.05.
The present study was carried out exclusively with secondary data and already published in a public information system, without information that could identify individuals, respecting the ethical principles contained in Resolution of the National Health Council (CNS) no. 466, of December 12, 2012, dismissing the need for its appreciation by the Research Ethics Committee.
RESULTS
In the period selected for analysis, 27,054 hospital admissions were recorded, with a mean of 4,509 ± 537,3 admissions due to DM, regardless of age, in the state of Ceará. Of these, 22,872 were for the treatment of the primary disease (DM), with an average of 3,763.5 ± 593.3. For the treatment of diabetic foot complications, 4,182 were recorded, with a mean of 697 ± 137.7.
It was observed that, over the years, the rate of hospitalizations related to DM for treatment of complications is decreasing, with a strong negative correlation (r = -0.9, p = 0.001) (Figure 1: a). There was a directly proportional correlation of moderate positive type among number of hospitalizations related to complicated diabetic foot (r = 0.6; p = 0.001) (Figure 1: b). These data suggest that the number of hospital admissions due to DM for the clinical management of complications has decreased over the years, however, the number of hospitalizations due to complicated diabetic foot in Ceará has increased (Figure 1).
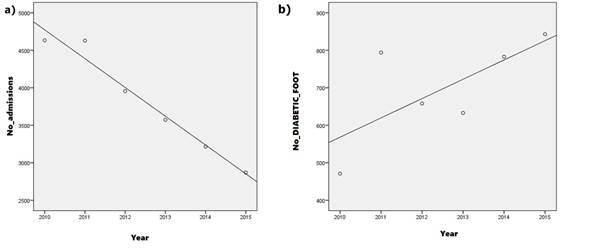
Figure 1 Correlation between the number of hospital admissions due to DM for the treatment of DM and treatment of complicated diabetic foot in Ceará between 2010 and 2015. Fortaleza-Ceará-Brazil, 2016.
We also analyzed the data regarding the number of hospitalizations in the state due to amputation regardless of the disease and/or health impairment. There were 5,914 cases with an average of 985.6 ± 299.7; of which 4,353 were dislocations of lower limbs, with an average of 725 ± 208.1; and 1,561 were disarticulation of foot and tarsus, with a mean of 260.1 ± 101.2.
In general, the Pearson coefficient obtained a strong correlation, but with no association (r = 0.8, p = 0.053) (Figure 2: a). For foot and tarsus, the correlation was moderate and positive, without association (r = 0.7, p = 0.061) (Figure 2:b).

Figure 2 Correlation between the number of hospital admissions regardless of the disease and disarticulation of lower limbs and disarticulation of foot and tarsus in Ceará between 2010 and 2015. Fortaleza-Ceará-Brazil, 2016.
Regarding the number of hospitalizations due to diabetes-related amputations in Ceará from 2010 to 2015, there were 1,283 cases, with a mean of 213.8 ± 128.4; of which 843 were of lower limbs, with a mean of 843 ± 140.5; and foot and tarsus were 439, with a mean of 79.2 ± 39.4.
For the Pearson coefficient, there was a strong positive correlation with association (r = 0.8, p = 0.023) between the number of hospitalizations due to amputation and disarticulation of lower limbs arising from DM (Figure 3: a). There was also a strong positive correlation and association (r = 0.9, p = 0.014) between foot and tarsal disarticulations (Figure 3: b). This strong correlation and association shows that the number of hospitalizations due to amputation with diabetes-related diagnosis has increased over time.
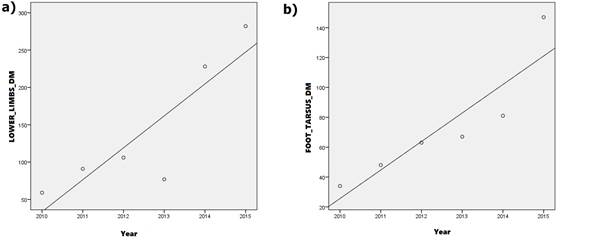
Figure 3 Correlation between the number of hospitalizations due to amputation related to diabetes and disarticulation of lower limbs and disarticulation of foot and tarsus in Ceará between 2010 and 2015. Fortaleza-Ceará-Brazil, 2016.
In summary, the strong negative correlation points out that the number of hospitalizations for treatment of diabetes complications has decreased. However, the positive correlation and strong association points out that, in contrast, the number of hospitalization due to complicated diabetic foot and diabetes-related amputation has increased proportionately over the years.
DISCUSSION
The complications of diabetic foot are the result of interaction between several risk factors, such as peripheral vascular disease, trauma, infection and neuropathy. Subsequent ulcerations and amputations impair quality of life and interfere with patient survival rates. The identification of risk factors and complications associated with diabetes subsidizes primary-level interventions and progression of minor lesions for the development of ulcers and future amputations5.
Infection is a more frequent complication of diabetic foot ulcers, accounting for up to 58% of infected ulcers. This rate increases in hospitalized patients and can reach up to 82%11. It was observed that a minor amputation predisposes to the increase of the possibility of larger amputation12.
The German Society of Vascular Surgery (DGG) defines minor amputations as any amputation below the ankle (including Chopart amputation). In Portuguese-speaking countries, minor amputations are all distal amputations to the tarsometatarsal line of articulation with anatomically correct resection and closure of the primary wound12.
In a cohort study conducted in the Netherlands with individuals with infected diabetic ulcers, independent predictors for lower extremity amputation were identified, such as positive probe-to-bone test, deep ulcer, elevated CRP levels and presence of sore skin or pre-tibial edema. Based on the findings, researchers developed new scores that are not covered by the IWGDF classification system and that can be easily used in clinical practice13.
Diabetic ulcers are often recalcitrant and at risk of infection, which can lead to amputation of the lower extremities or bone resection. In a clinical trial, the incidence of amputation/bone resection in general was 8.9% (28/314), 5.5% (9/163) of patients who had received a dermal replacement derived from human fibroblasts and 12.6% (19/151) of patients under conventional care (p = 0.031). Of the 28 cases of amputation/bone resection, 27 were preceded by ulcer-related infection. There were significantly fewer amputations/bone resections in patients who received dermal substitute derived from human fibroblasts versus conventional care, which is probably related to the lower incidence of adverse infection events observed in the dermal group substitute treatment derived from human fibroblasts14.
It is estimated that, in Brazil, for a population of 7.12 million people with DM, there is the occurrence of 484,500.5 ulcers, 169,600 hospital admissions and 80,900 amputations, of which the outcome is death for 21,70015. The prevalence has varied according to the region of the country, from 18.3% between 2007-2008 and 69% in 2014, within the same Brazilian state16)(17)(18)(19. The main factors related with the occurrence of amputations were low schooling (p = 0.027), two or more people living in the household (p = 0.046), patient income lower than a minimum wage (p = 0.004), not having the feet examined (PR = 1.17) and having not receive guidance on foot care (PR = 2.24) in the consultations carried out in the last year, besides not using medication to control DM according to prescription (PR = 1.60) and inadequate blood glucose control (PR = 1.83)18.
Am ecological study conducted in the state of Ceará between 2001 and 2012 that investigated the trends of hospitalizations due to DM among adults and the elderly pointed to an increasing trend of hospitalizations, with a large majority of hospitalizations due to diabetes occurring in females. However, trends tended to be increasing for men (p = 0.002; r² = 0.734) and decreasing for women (p <0.001; r² = 0.957). For both sexes, the number of hospitalizations was higher among older people20.
Lower limbs are one of the most vulnerable regions of the body in people with DM, resulting in a deficiency in wound healing and even amputation. Therefore, it is necessary that, in addition to all the care with drug and non-drug treatment, there is also a disclosure of the need for foot care to prevent these diseases21.
There has been an increasing number of people with diabetic foot-related complications, which has an impact on public health and, above all, on the quality of life of these people. Regarding the proportion of people aged 18 years or older who reported a diagnosis of diabetes and had their feet examined in the last 12 months, the data indicate that, in Ceará, the overall proportion is 23.9, being below the general Brazilian proportion, which is 29.122.
However, despite these estimates and advances in health care, amputations are still significant in people with diabetes. In this context, the high rates of amputation and hospitalization cause a reduction in the working capacity of individuals of productive age, interfering in the quality of life of these people.
This study allowed inferring that in the state of Ceará there is a strong tendency to increase hospitalizations due to complicated diabetic foot, as verified in recent years. This allows managers and other health professionals to plan preventive policies, mainly to avoid the development of ulcers and, consequently, of amputations.
Among the limitations of this study, it is impossible to identify the number of people hospitalized by gender, age and other factors that may be associated.
CONCLUSION
Thus, the data reveal a thin line regarding the health care of the person with DM. The number of hospitalizations due to DN in the state of Ceará has decreased, but the number of hospitalizations per complicated foot and amputation of lower limbs and foot and tarsus have increased strongly. The identification of this serious problem can contribute to the formulation and assistance of public policies, health management strategies and health professionals engaged in the planning and implementation of actions aimed at the prevention of foot complications in people with diabetes and consequent hospitalizations and amputation, since it is a condition that is up to Primary Health Care.
REFERENCIAS
1. International Diabetes Federation. IDF Diabetes. 7ª ed. Belgium; 2015. [ Links ]
2. World Health Organization. WHO Global action plan for the prevention and control of noncommunicable disease 2013-2020 [Internet]. Geneva: World Health Organization; 2013 [cited 2016 Oct 20]. Available from: http://www.who.int/nmh/events/ncd_action_plan/en/. [ Links ]
3. Diretrizes da Sociedade Brasileira de Diabetes (2015-2016). São Paulo: A.C. Farmacêutica, 2016. [ Links ]
4. Alexiadou K, Doupis J. Management of Diabetic Foot Ulcers. Diabetes Ther. 2012 Dec; 3(1): 4. Published online 2012 Apr 20. doi: 10.1007/s13300-012-0004-9. [ Links ]
5. Malhotra S, Bello E, Kominsky S. Diabetic foot ulcerations: biomechanics, charcot foot, and total contact cast. Semin Vasc Surg. 2012 Jun;25(2):66-9. doi: 10.1053/j.semvascsurg.2012.05.001. [ Links ]
6. Neville RF, Sidawy AN. Surgical bypass: when is it best and do angiosomes play a role? Semin Vasc Surg. 2012 Jun;25(2):102-7. doi: 10.1053/j.semvascsurg.2012.04.001. [ Links ]
7. Alavi A, Sibbald RG, Mayer D, Goodman L, Botros M, Armstrong DG et al. Diabetic foot ulcers: Part I. Pathophysiology and prevention. J Am Acad Dermatol. 2014 Jan;70(1):1.e1-18; quiz 19-20. doi: 10.1016/j.jaad.2013.06.055. [ Links ]
8. International Working Group on the Diabetic Foot the Diabetic Foot. IWGDF Guidance on the prevention of foot ulcers in at-risk patients with diabetes. International Working Group on the Diabetic Foot (IWGDF). 2015. Available from: http://www.iwgdf.org [ Links ]
9. Shahbazian H, Yazdanpanah L, Latifi SM. Risk assessment of patients with diabetes for foot ulcers according to risk classification consensus of International Working Group on Diabetic Foot (IWGDF). Pak J Med Sci. 2013 May;29(3):730-4. [ Links ]
10. Sagray B, Malhotra S, Steinberg JS. Current therapies for diabetic foot infections and osteomyelitis. Clin Podiatr Med Surg. 2014;31:57-70. http://dx.doi.org/10.1016/j.cpm.2013.09.003 [ Links ]
11. Prompers L, Huijberts M, Apelqvist J, Jude E, Piaggesi A, Bakker K et al. High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe. Baseline results from the Eurodiale study. Diabetologia. 2007 Jan;50(1):18-25. Epub 2006 Nov 9. [ Links ]
12. Matamoros R, Riepe G, Drees P. Minor amputations - a maxi task. Part 1: From the principles to transmetatarsal amputation. Chirurg. 2012 Oct;83(10):923-33; quiz 934. doi: 10.1007/s00104-010-2054-8. [ Links ]
13. Pickwell K, Siersma V, Kars M, Janeiro A , Bakker K , Edmonds M, et al. Predictors of lower-extremity amputation in patients with an infected diabetic foot ulcer. Diabetes Care 2015 May; 38(5): 852-57. http://dx.doi.org/10.2337/dc14-1598 [ Links ]
14. Frykberg RG, Marston WA, Cardinal M. The incidence of lower-extremity amputation and bone resection in diabetic foot ulcer patients treated with a human fibroblast-derived dermal substitute. Adv Skin Wound Care. 2015 Jan;28(1):17-20. doi: 10.1097/01.ASW.0000456630.12766.e9. [ Links ]
15. Brasil. Ministério da Saúde; Secretaria de Atenção à Saúde; Departamento de Atenção Básica. Manual do pé diabético: estratégias para o cuidado da pessoa com doença crônica. Brasília; 2016. [ Links ]
16. Oliveira VM, Moreira D. Prevalência de amputados de membros inferiores atendidos no Hospital da Vila São José Bento Cottolengo, em Trindade - GO. RVS [Internet]. 2009 Jan./Mar [cited 2014 Nov 21];3:20-37. Available from: http://www.fugedu.com.br/upload/journals/1/issues/24/public/24-52-PB.pdf 13. [ Links ]
17. Oliveira JC, Taquary SAS, Barbosa AM, Veronezi RJB. Pé diabético e amputações em pessoas internadas em hospital público: estudo transversal. ABCS Health Sci. 2016; 41(1):34-39. [ Links ]
18. Santos ICRV, Sobreira CMM, Nunes ENS, Morais MCA. Prevalência e fatores associados a amputações por pé diabético. Ciênc. saúde coletiva [Internet]. 2013 Oct [cited 2016 Nov 21] ; 18(10): 3007-3014. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232013001000025&lng=en. http://dx.doi.org/10.1590/S1413-81232013001000025. [ Links ]
19. Santos IV, Carvalho EF, Souza WV de, Albuquerque EC de. Prevalência de amputações e revascularizações por pé diabético e suas características. Rev enferm UFPE on line. 2016; 10(7):2354-61. [ Links ]
20. Santos FAL, Lima WP, Santos AL, Teston EF, Marcon SS. Hospitalizações por diabetes em adultos e idosos no Ceará, 2001-2012. Epidemiol. Serv. Saúde [Internet]. 2014 Dez [citado 2016 Nov 17] ; 23(4): 655-63. Disponível em: http://scielo.iec.pa.gov.br/scielo.php?script=sci_arttext&pid=S1679-49742014000400007&lng=pt. [ Links ]
21. Andrade NHS, Dal Sasso-Mendes K, Faria HTG, Martins TA, Santos MA, Teixeira CRS, et al. Pacientes com diabetes mellitus: cuidados e prevenção do pé diabético em atenção primária à saúde. Rev enferm UERJ. 2010;18(4):616-21. [ Links ]
22. Instituto Brasileiro de Geografia e Estatística. Pesquisa Nacional de Saúde 2013: percepção do estado de saúde, estilos de vida e doenças crônicas - Brasil, Grandes Regiões e Unidades da Federação. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2014. Disponível em: ftp://ftp.ibge.gov.br/PNS/2013/pns2013.pd. [ Links ]
Received: March 05, 2017; Accepted: May 27, 2017
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
