










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.18 n.55 Murcia Jul. 2019 Epub Oct 21, 2019
https://dx.doi.org/10.6018/eglobal.18.3.337311
Originals
Child mortality: trend and changes after the implantation of the rede mãe paranaense program
1Universidade Estadual do Centro Oeste/UNICENTRO. Guarapuava (PR), Brasil. kellyhprezotto@hotmail.com
2Universidade Estadual do Norte do Paraná/UENP. Bandeirantes (PR), Brasil.
3Universidade Estadual de Maringá/UEM. Maringá (PR), Brasil.
4Universidade de São Paulo/USP. Ribeirão Preto (SP), Brasil.
Introduction
The prevention of infant mortality is one of the main objectives of global public policies. The Rede Mãe Paranaense Program was established in 2012 in the State of Paraná Brazil, recommending the management of mother and child health in the prenatal, puerperal and follow-up of children’s growth and development. The objective of the study was to analyze the trend of infant mortality according to macroregional health in the State of Paraná and changes after the implantation of the Rede Mãe Paranaense Program.
Method
This is an ecological study with data from the Mortality Information System from 2000 to 2014. Mortality coefficients were calculated, and trend analysis was performed using polynomial regression models. Deaths in the pre-implantation trimester of the Rede Mãe Paranaense Program (2009-2011) and in the post-implantation triennium (2012-2014) were analyzed according to maternal, childbirth and child variables.
Results
There was a reduction in infant mortality in macroregional health and in the state of Paraná. From the pre-implantation period for the post-implantation period of the Program, there was a reduction in the infant mortality rate in the State of Paraná, from 12.0 to 11.2 deaths/thousand live births. There was an increase in the coefficients in six of the 22 regional health and in the reduction of deaths among children and mothers under 20 years of age, schooling less than eight years and non-white children.
Conclusion
Infant mortality declined in the State of Paraná and, after implementation of the Rede Mãe Paranaense Program, there was a reduction in deaths in the groups with factors commonly associated with infant mortality.
Key-words: Infant mortality; Public health; Epidemiology
INTRODUCTION
Improving maternal and child health and avoiding prevenTable deaths of children or their mothers remains a major national and international concern in the field of reproductive health and rights1. Infant mortality (IM) decimates millions of children annually throughout the world, especially in developing countries. Outlined as that occurring among children under one year of age, the coefficients related to these deaths are excellent indicators of living and health conditions and go along with the economic development and quality of life of the population, since they show the physical and social vulnerability in which these children are let into after birth2.
Infant deaths have their outcome after one or several risk factors correlated with each other, which directly interfere with maternal and child health during gestation, delivery and lactation, extending up to 12 months of life. These factors include biological, physical and socioeconomic characteristics, such as age, schooling and marital status, number and quality of prenatal consultations, type of delivery, prematurity and birth weight3.
In underdeveloped or developing countries such as Serra Leoa, Angola, Chad and Somalia, the Infant Mortality Coefficient (IMC) in 2012 exceeded 145 deaths per 1000 live births (LB). In developed countries such as Sweden, Norway, Iceland and Luxembourg, the IMC is limited to less than three deaths per 1000 LB4, which confirms the repercussion of local socioeconomic development in infant deaths5.
Prevention of IM is one of the main objectives of global public policies, which occur through federal, state and local government actions and interventions, such as the various pacts and programs developed after the fourth of the Millennium Development Goal (MDG), which aimed to reduce child mortality by two-thirds, between 1990 and 20156, such as the Rede Mãe Paranaense Program (PRMP) in the state of Paraná.
The Rede Mãe Paranaense Program was established in 2012, recommending the management of mother and child health in the prenatal, puerperal and follow-up of children’s growth and development especially in the first year of life7, in order to identify gestational risks and, consequently, ensure effective and quality care.
In Brazil, the trend of infant mortality is decreasing, since the IMC has decreased considerably in the last ten years. In Paraná, there is also a decrease in this indicator, especially in the period from 2001 to 2011, when the IMC increased from 17.4 to 11.6 deaths/1000 LB8, coefficients lower than those observed for all Brazilian municipalities9.
Despite the positive results observed from investments in maternal and child health in the state, such as the implementation of PRMP, Paraná still has high infant mortality rates, and it is possible to suspect regional iniquities and the need for more localized investigations10.
With this understanding, this study aimed to analyze the trend of infant mortality according to macroregional health in the State of Paraná and the differences after the implantation of the Rede Mãe Paranaense Program according to mother, childbirth and child characteristics.
METHOD
This is a cross-sectional, ecological, time-series study on infant mortality in the State of Paraná, Brazil, from 2000 to 2014. The State of Paraná is in the southern region of the country, with a territorial area of 199,307,922 km², and is composed of 399 municipalities, distributed in 22 Regional Health (RH) that are arranged in four Macroregional Health: East, North, Northwest and West. Macroregional Health are designed to link Regional Health so that they can combine their efforts to solve common problems11. The Human Development Index (HDI) of Paraná in 2010 was 0.749, ranking 5thamong all Brazilian states, and exceeding the HDI observed for the set of Brazilian municipalities, which was 0.742 in the same year12.
For the analysis of infant mortality data were collected in the Mortality Information System (SIM) and on Live Births Information System (Sinasc), available on the portal of the Department of Informatics of the Unified Health System - DATASUS. The deaths of children under one year old from Paraná, between 2000 and 2014 was selected. The infant mortality coefficient (IMC) per 1000 live births were calculated for each Regional and Macroregional Health by characteristics (natural and cesarean birth) and characteristics of the child (gender, race/color, birth weight and gestational age).
Trend analysis was performed using the polynomial regression model. The IMC was considered the dependent variable (Y) and the calendar years as the independent variable (X). To avoid autocorrelation between the terms of the regression, the year variable was transformed into the year-centered variable (X minus the midpoint of the historical series, year 2006). The simple moving average of the IMCs, consisting of the sum of the variable of three consecutive years divided by three, except for the first (2000) and the last year (2014), were calculated.
The regression models tested were linear (Y = β0+β1X), second degree (Y = β0+β1X + β2X2) and third degree (Y = β0+β1X + β2X2+ β3X3). The most appropriate model was the one with statistical significance (p<0,05), with a better measure of precision (r2) and presenting residues without defects.
Data were also analyzed considering three years: the first (2009-2011), which consists of the pre-implantation period of the Rede Mãe Paranaense Program, and the second (2012-2014), which deals with the post-implantation period. in the period before and after implantation of the Mãe Paranaense Program, the percentage variation between the triennia was calculated by multiplying the IMC of the second triennium by 100, divided by the IMC of the first triennium, subtracted from 100. For the organization and analysis of the data were used the programs Excel and Statistical Package for the Social Sciences - SPSS 20.0.
Because it is a study with a secondary database, in the public domain, it was requested exemption of analysis and evaluation by the Committee of Ethics in Research with Human Beings of the State University of Maringá, obtaining favorable opinion number 07/2017.
RESULTS
There was a downward trend in IMC in the state of Paraná and in all macroregional health (p<0.001), with a variation in the coefficient of determination (R2) from 0.86 to 0.98 (Table 1).
Table 1. Trends in infant mortality in the State of Paraná according to Macroregional Health Departments. Paraná, 2000 to 2014

$Determination coefficient; * Trend confidence level.
*Trend confidence level.
Figure 1 graphically shows the IMCs of the Macroregional Health during the study years. The four macroregions showed a decreasing curve in the studied period, with oscillations. It is emphasized the increase in infant deaths in the western region in 2003 (17.3 deaths/1000 LB), with a subsequent decrease in 2004 (15.6 deaths/1000 LB). Macroregional Northwest had the lowest IMC in the year 2010 (10.5 deaths/1000 LB), showing a gradual increase in the following years.
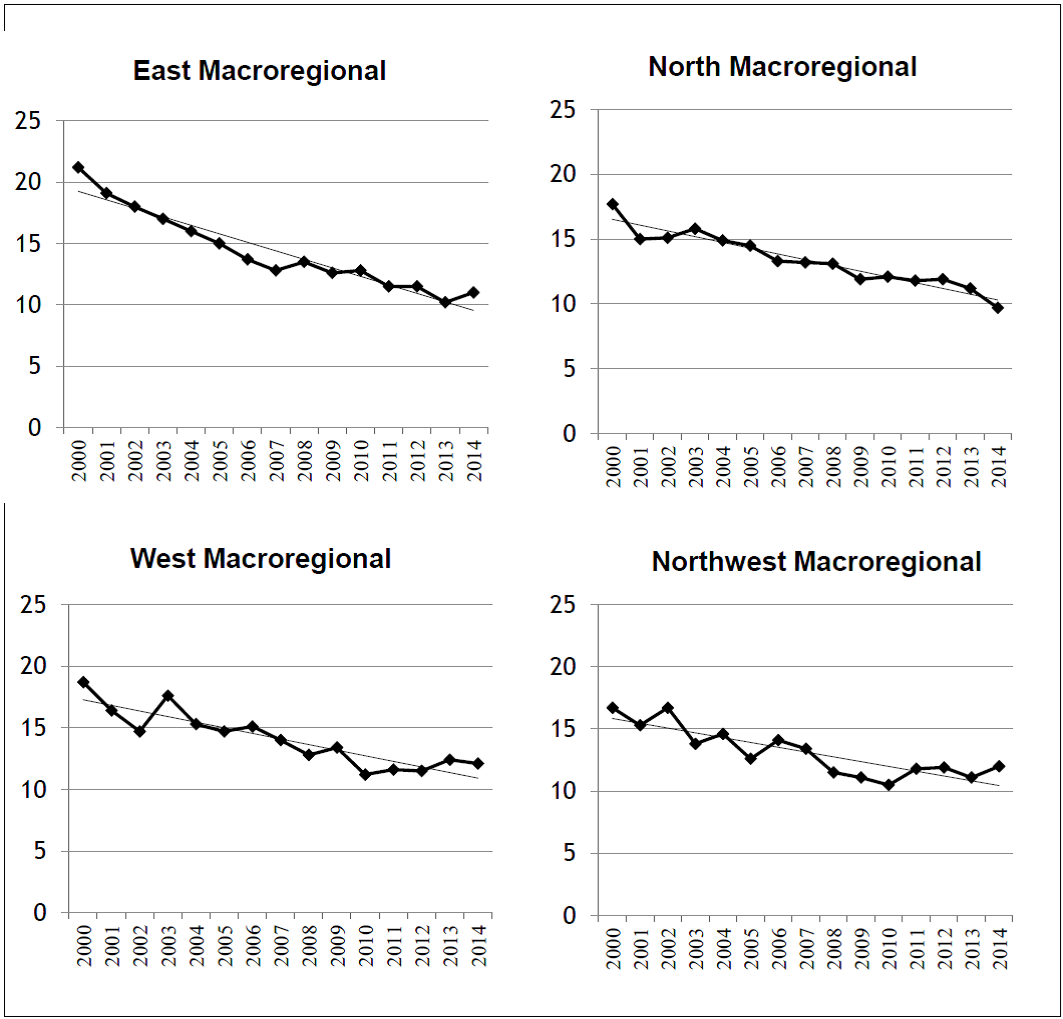
Axis y = infant mortality coefficient (IMC), Axis x = study years.
Figure 1. Infant mortality coefficients according to year of occurrence and macroregional health. Paraná, from 2000 to 2014
Table 2 shows the IMC of the triennium before and after the implantation of the PRMP in the Regional and Macroregional Health and their percentage difference. Of the 10,775 infant deaths occurred in the state of Paraná from 2009 to 2014, 5,483 occurred in the first triennium (12.0 deaths/1000 LB) and 5,292 (11.2 deaths/1000 LB) in the second triennium, indicating a decrease in infant mortality after implementation of the PRMP. In the first period, the macroregion with the highest IMC was in the East, with 12.3 deaths/1000 LB. However, it was also the Macroregional Health with the largest fall in relation to the second triennium (-11.4%). It stands out the Northwest Macroregional Health, with IMC increasing from the first to the second period, being the only macroregional with this profile (Table 2).
Table 2. Distribution of infant mortality according to Macroregional Health and Regional Health. Paraná, from 2009 to 2014.
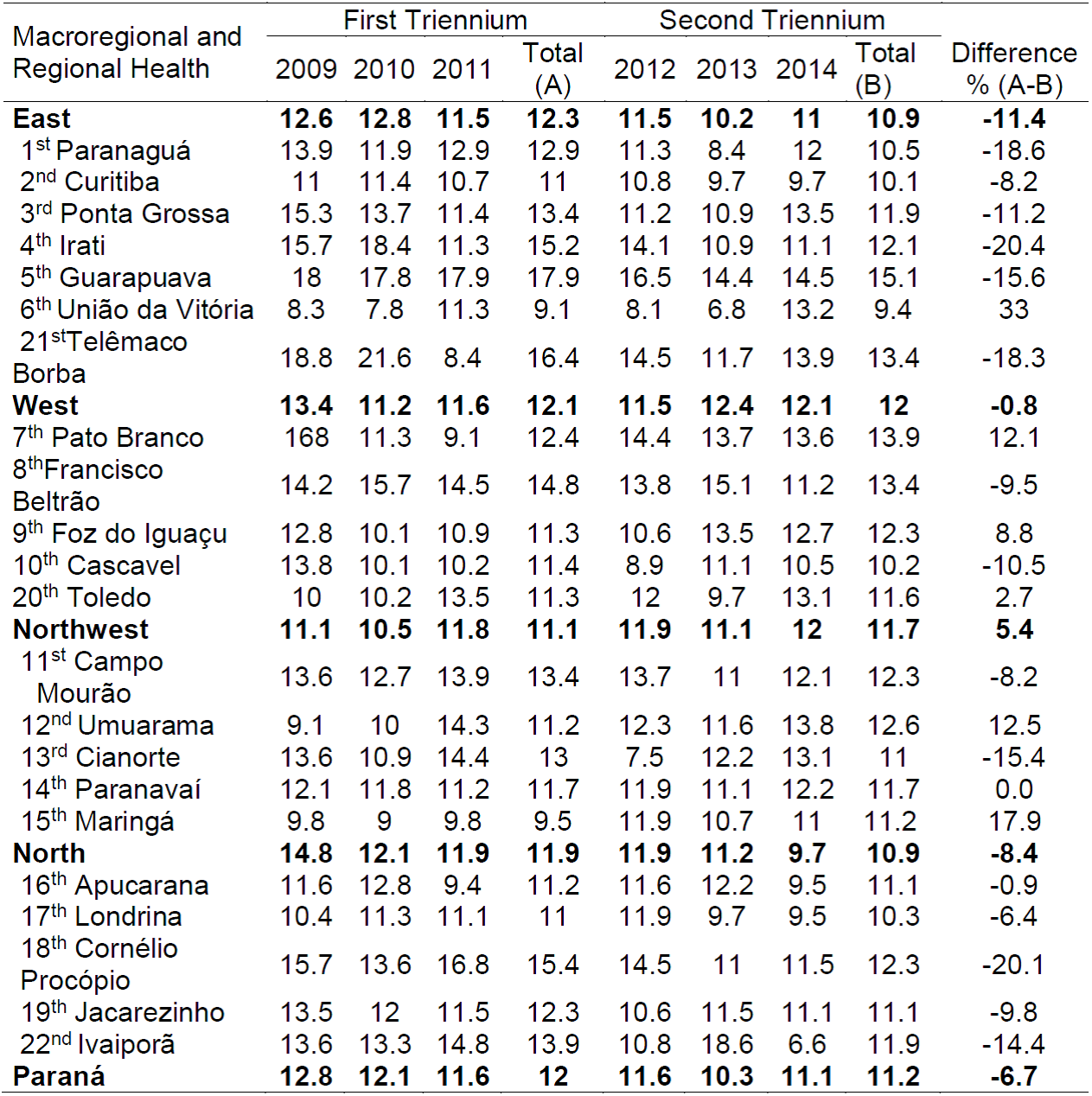
The Regional Health with the highest percentage reduction of the IMC between the three years was Irati (-20.4%) and the one with the highest percentage increase was that Maringá (17.9%). There was a reduction in all the Regional Health services of the North Macroregional Health (Table 2).
Regarding maternal age, Table 3 shows that the lower IMCs are in the range of 20 to 34 years, with IMC of 10.0 deaths/1000 LB before PRMP and 9.6 deaths/1000 LB after PRMP in the State of Paraná. The highest IMC was observed in the children of mothers under 20 years of age. In the North Macroregional Health, there was a percentage reduction in IMC for children of mothers less than 20 years of age (-17.9%) and for mothers aged 35 years or over (-30.1%) and increase in IMC in the range aged 20 to 34 years (2%). In the Northwest Macroregional Health, there is an increase in IMC for children of women 35 and over (11.6%) and for women 20-24 (4.2%) (Table 3).
It was observed a reduction in IMC for mothers with less than 8 years of study in all the Macroregional Health. The Northwest region was the only one that presented a percentage increase in IMC for maternal schooling over 8 years (9.8%). There was a reduction in the IMC of the State of Paraná for both types of delivery. Only the Northwest region showed an increase in IMC for both vaginal and cesarean sections (Table 3).
Table 3. Infant mortality according to maternal and labor characteristics by Macroregional Health. Paraná, from 2009 to 2014

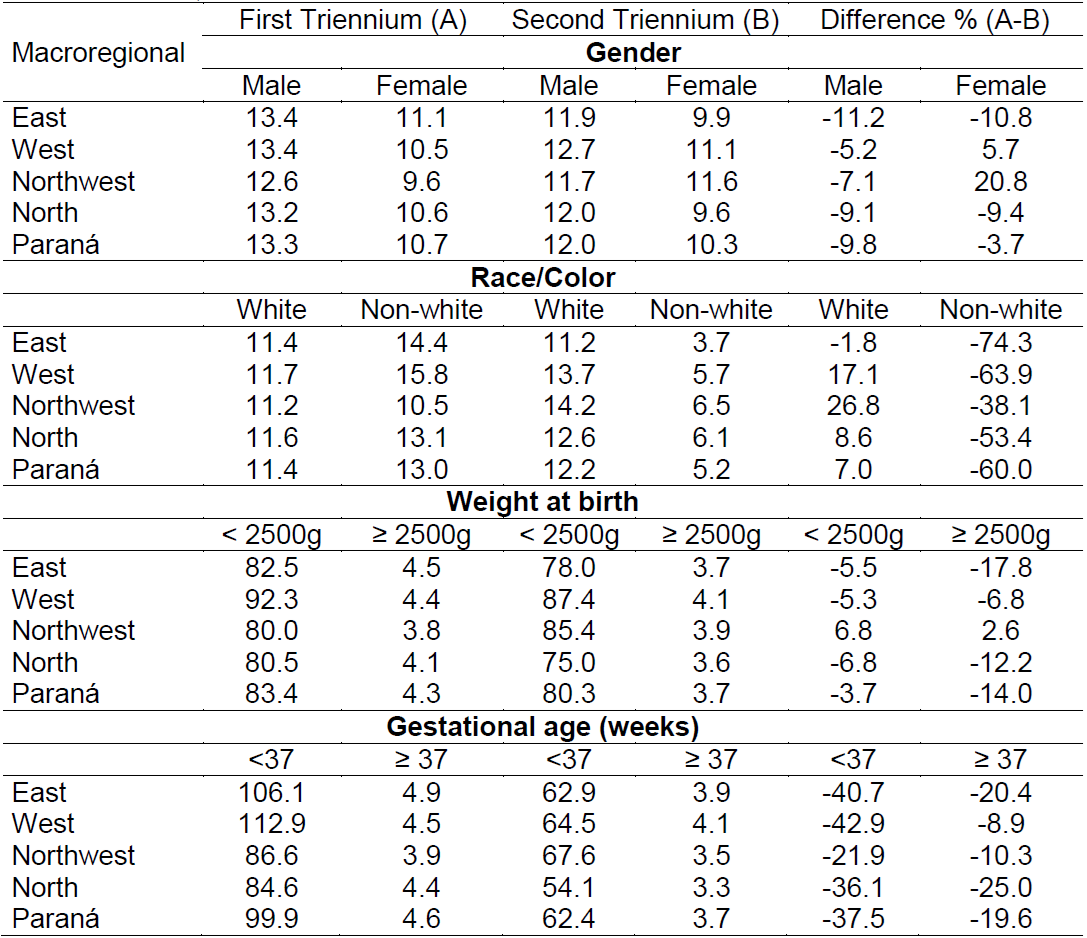
In the first triennium, children of non-white race/color had higher IMCs than white children (13/1000 LB and 11.4/1000 LB, respectively). After the implantation of the PRMP, it was observed a reduction of the IMCs in all macroregions for the non-white race/color. In Paraná, the reduction reached 60%, while for white children there was an increase of 7%.
Preterm and low birth weight infants had the highest IMC among all the characteristics analyzed. However, considering the pre and post-implantation period of the PRMP, there was a 3.7% reduction in IMC in low birth weight neonates in Paraná and 14% in those with a weight greater than 2500g. The percentage difference was higher considering gestational age, where a 37.5% decrease in IMC was observed for preterm infants (Table 4).
DISCUSSION
The present study analyzed the trend of infant mortality in the years 2000 to 2014 in the state of Paraná, and the changes in the pre and post-implantation period of PRMP, according to maternal, childbirth and child characteristics. The results showed a decreasing tendency of infant deaths in the four macroregions and in the State of Paraná and a reduction in most of the IMC, after the implantation of the PRMP.
Analyzes at each regional and macroregional health allowed us to identify the impact of PRMP on risk groups and the context in which infant deaths are inserted. The decrease in IMC can be justified from the implementation of actions to achieve goals proposed by the World Health Organization through the Millennium Development Goals, such as the advancement of immunization-related technologies and oral rehydration therapy, on the importance of breastfeeding, the expansion of basic sanitation, the reduction in fertility and the expansion of prenatal and childbirth care13. These results indicate that strategies need to be kept and intensified to reduce child mortality in order to maintain the declining trend observed in other studies14,15.
After the implementation of the PRMP, infant mortality decreased in three of the four macroregions of health and in the State of Paraná, a result similar to that of a study that evaluated PRMP in the years 2010 to 2013, and showed that infant mortality reduced only in some Regional Health16.
The discrete decrease in infant mortality in Paraná after the implantation of PRMP (12.0 in the first period to 11.2 deaths/1000 LB in the second period) can also be observed in the East, West and North macroregions of health, in which the best performance was in the East macroregional, which decreased from 12.3 to 10.9 deaths/1000 LB from the first to the second period. On the other hand, in the North-Western macroregion, the IMC increased from 11.1 in the first period to 11.7 deaths/1000 LB in the second period. In addition, six of the 22 regional health showed an increase in the IMC in the three-year period analyzed. Corroborating these findings, official data from the United Nations agency showed that differences observed in a locality, such as the State of Paraná, are strongly associated with socioeconomic conditions and access to health services in each region, constituting an indicator of iniquity related to specific groups17.
Regarding the maternal characteristics, the IMC of the children of mothers aged 20 to 34 years were lower than those of the other age groups. The result was expected since in this age group, the woman’s body is usually developed and healthy for gestation and, therefore, with a lower reproductive risk18. Similar results were also found in a study carried out in Paraná in the year of 2015, which analyzed the obstetric profile of users of the Unified Health System after implementation of PRMP19. On the other hand, adolescent mothers presented higher IMC in the two triennial years. Adolescence is a risk factor for infant mortality, since, for the most part, the life condition of these adolescents is linked to the adverse socioeconomic conditions, mainly low income and schooling levels20.
However, it is worth mentioning that a greater reduction of the IMCs was observed in the age groups under 20 years of age and over 35 years of age in the State of Paraná (-11.2% and -10.1%, respectively) compared to the age of 20 to 34 years, which shows that PRMP has impacted IMC in mothers at risk ages. In all macroregions, there was a reduction in IMC for adolescent mothers.
Children of women with education less than eight years of schooling presented a higher IMC when compared to the children of women with schooling equal to or greater than eight years. Women with low schooling are classified in the intermediate risk group according to the PRMP, since the deficit in prenatal care is directly related to low socioeconomic and cultural conditions, which may interfere adherence to the ideal gestational follow-up process21. However, after the implantation of the PRMP, the IMC of the children of these women reduced significantly in all the macroregions and in the State of Paraná.
Regarding the type of delivery, higher IMCs were identified for vaginal delivery, which corroborates with other studies22,23,24,25. However, a study carried out in Spain showed that cesarean sections without a medical indication have a negative impact on newborn’s health, analyzed by the Apgar score26. Considering that the procedure increases the risks of mother and infant morbidity and mortality, the PRMP aims to reduce caesarean sections by 10% per year throughout the state7. The impact of PRMP on IMC when delivered by cesarean section was positive, only the north-western macroregional did not present a drop in IMC for this type of delivery.
Regarding the race/color of the children who died during the study period, it was observed that before the implantation of the PRMP the IMC of non-white children was higher than the IMC of white children (13 and 11.4 deaths/1000 LB, respectively). In the post-implantation period of the program, there was a decrease in the IMCs of non-white children and an increase in the IMCs of white children. The PRMP guideline, which characterizes mothers and children of black race/color as people of intermediate risk in the reproduction process, because they presented higher coefficients of maternal and infant mortality in 2010 when compared to the mortality of mothers and children of white race/color, showed twice greater risk for individuals of non-white race/color27. The analysis of the two periods identified that there was an impact for this group of children.
Major IMC were observed among children who were born weighing less than 2,500 grams and with a gestational age of less than 37 weeks gestation (greater than 80 deaths/1000 LB) in the four macroregional health centers of the state, with a decrease after implantation of PRMP for both groups. The high numbers of infant deaths are justified because of low birth weight and prematurity directly influence infant health presenting high risks of morbidity and mortality after birth, being correlated with socioeconomic characteristics such as maternal age and schooling28. Despite the decrease in IMC in children with low birth weight and premature infants (80.3 and 62.4 deaths/1000 LB) in the second triennium, IMC was higher than all other coefficients of each characteristic studied, demonstrating the need of high complexity services in the postpartum period for the care of these children, which can help in the prevention of infant deaths.
Regarding birth weight, there was a reduction in IMC in all macroregions, except in the northwest. Considering the gestational age, there was a decrease in all the macroregions studied. Despite the decrease in IMC, studies show that the reduction of infant mortality rates does not reduce the severity of these deaths, that is, a child’s death, depending on the circumstances in which it occurs, generates social discontent, something avoidable29.
Some limitations may influence the results of the present study, such as the recent implementation of the PRMP in Paraná, considering that strategies are elaborated and require a certain time to show their effectiveness, as well as the use of secondary databases, being able to restrain the search for variables such as prenatal consultations and mother marital status. However, Health Information Systems are one of the most effective means in the analysis of health services, managements and evaluations at the national, state and municipal levels30, being a methodology widely used in scientific research in the area
CONCLUSION
Infant mortality declined throughout Paraná, in its distinct Macroregional Health, with differences in coefficients from one place to another. From the implementation of the PRMP, it was observed the continuity in the decrease of these deaths. This decreasing trend has been observed since the year 2000, and it is not possible, only with the difference of the coefficients year to year, to affirm the effectiveness of the program. However, there was an improvement in IMC according to maternal, childbirth and child characteristics, since the mortality among children of mothers with low schooling, over 34 years of age, children born with low birth weight, premature and non-white, had their mortality coefficients decreased after the implementation of the program.
The decrease in infant deaths is a reality that occurs at the global, national, state and municipal levels, due to the improvement of public policies such as PRMP. However, the decrease in these coefficients does not depend only on the implementation of these policies, but also on programs which aim to improve socioeconomic conditions, cultural and educational development of populations.
Infant mortality should be the object of constant study, since it contributes to the evaluation of programs and initiatives such as the Rede Mãe Paranaense, favors the detection of socioeconomic disadvantages and access to health services and allows the improvement of care for their reduction. Thus, the present study can contribute to the monitoring of infant mortality in the state of Paraná and bases later studies that can evaluate the effectiveness of the Rede Mãe Paranaense Program.
REFERÊNCIAS
1. Tavares L, Albergaria T, Guimarães M, Pedreira R, Junior EP. Mortalidade infantil por causas evitáveis na Bahia, 2000-2012. Rev Electron Comun Inf Inov Saude. 2016;10(3): 01-10. [ Links ]
2. Pizzo LGP, Andrade SM, Silva AMR, Melchior R, González AD. Mortalidade infantil na percepção de gestores e profissionais de saúde: determinantes do seu declínio e desafios atuais em município do sul do Brasil. Saude Socied. 2014; 23(3): 908-918. [ Links ]
3. Barbosa TAGS, Coelho KR, Andrade GN, Bittencourt SDA, Leal MC, Gazzinelli A. Determinants of infant mortality in cities of the Jequitinhonha Valley, Minas Gerais, Brazil. REME. 2014; 18(4):907-22. [ Links ]
4. The World Bank. Indicadores Banco Mundial, 2014. Available from: http://data.worldbank.org/products/wdi [ Links ]
5. Roser M [homepage on the Internet] (2018) - Child Mortality. 2018 Retrieved from: https://ourworldindata.org/child-mortality [ Links ]
6. Brasil. Presidência da República. Objetivos de desenvolvimento do milênio: Relatório Nacional de Acompanhamento. Brasília: Presidência da República, 2007 [Internet]. 2007; Available from: http://www.pnud.org.br/docs/3_relatorionacionalacompanhamentoodm.pdf [ Links ]
7. Paraná. Secretária de Saúde do Estado do Paraná. O que é Rede Mãe Paranaense. Paraná: Secretária de Saúde. 2012; Available from: http://www.saude.pr.gov.br/modules/conteudo/conteudo.php?conteudo=2892 [ Links ]
8. Paraná. Secretária de Saúde do Estado do Paraná. Situação da Mortalidade Infantil de 2000 a 2014. Paraná: Secretária de Saúde, 2014. [ Links ]
9. Departamento de Informática do Sistema Único de Saúde. Indicadores Básicos para Saúde no Brasil. 2ª Ed. Cap 6. 2015. [ Links ]
10. Frank BRB, Toso BRGO, Viera CS, Guimarães ATB, Caldeira S. Avaliação da implementação da Rede Mãe Paranaense em três Regionais de Saúde do Paraná. Saude debate. 2016; 40(109): 163-174. [ Links ]
11. Paraná. Secretária de Saúde do Estado do Paraná. Plano Estadual de Saúde Paraná 2012-2015. Paraná: Secretária de Saúde, 2013. [ Links ]
12. Paraná. Instituto Paranaense de Desenvolvimento Econômico e Social. Paraná em números. Paraná: IPARDES, 2013. [ Links ]
13. Atlas do Desenvolvimento Humano no Brasil 2013[homepage on the Internet]. Brasília: Programa das Nações Unidas para o Desenvolvimento [cited 2018 Abr 16]. Available from: http://www.atlasbrasil.org.br/2013/pt/ [ Links ]
14. Oliveira CM, Bonfim CV, Guimarães MJB, Frias PG, Medeiros ZM. Mortalidade infantil: tendência temporal e contribuição da vigilância do óbito. Acta paul enferm. 2016;29 (3): 282-290. [ Links ]
15. Atrash HK. Childhood mortality: still a global priority. J Hum Growth Dev. 2013; 23(3):257-60. [ Links ]
16. Netto A, Silva R, Santos M, Tacla M, Caldeira S, Brischiliari S. Mortalidade infantil: avalilação do Programa Rede Mãe Paranaense em Regional de Saúde do Paraná. Cogitare Enfermagem. 2017; 22(1):01-08. [ Links ]
17. Organização das Nações Unidas. Situação Mundial da Infância. Cad Brasil. 2016; 25-29. [ Links ]
18. Donoso E, Carvajal JA, Vera C, Poblete JA. Women age as a risk factor for maternal, fetal, neonatal and infant mortality. Rev Med Chil. 2014;142(2):168-74. [ Links ]
19. Novaes ES, Oliveira RR, Melo EC, Varela PL, Mathias TAF. Perfil obstétrico de usuárias do Sistema Único de Saúde após a implantação do Rede Mãe Paranaense. Ciênc Cuid Saúde. 2015: 14(4):1436-44. [ Links ]
20. Fernandes C, Vieira VCL, Scochi MJ. Mortalidade infantil e classificação de evitabilidade: pesquisando municípios da 15ª Regional de Saúde do Paraná. Cien Cuid Saude. 2013; 12(4):752-59. [ Links ]
21. Gomes RMT, César J. A. Perfil epidemiológico de gestantes e qualidade do pré-natal em unidade básica de saúde em Porto Alegre, Rio Grande do Sul, Brasil. Rev Bras Med Fam Comunidade. 2013; 8(27):80-89. [ Links ]
22. Lima JC, Oliveira Júnior GJ, Takano OA. Fatores associados à ocorrência de óbitos fetais em Cuiabá, Mato Grosso. Rev Bras Saúde Mater Infant. 2016; 16(3):353-61. [ Links ]
23. Oliveira RR, Costa JR, Rossi RM, Rodrigues AL, Mathias TAF. Infant mortality and associated factors: a study according to socio-occupational typologies. Cienc Cuid Saude. 2015: 14(2):1165-74. [ Links ]
24. Santos SPC, Lansky S, Ishitani LH, França EB. . Óbitos infantis evitáveis em Belo Horizonte: análise de concordância da causa básica, 2010-2011. Rev Bras Saúde Mater Infant. 2015; 15(4):389-99. [ Links ]
25. Melo EC, Ribeiro AB, Oliveira RR, Zurita RC, Mathias TAF. Analysis of Maternal and Child Health Indicators in an Area at Paraná State, Brazil. Nurs Res Prac. 2013; 2013: 495178. [ Links ]
26. Costa-Ramón AM, Rodríguez-González A, Serra-Burriel M, Campillo-Artero C. It's about time: Cesarean sections and neonatal health. J Health Econ. 2018;59:46-59. [ Links ]
27. Paraná. Secretária de Saúde do Estado do Paraná. Linha Guia - Rede Mãe Paranaense. Paraná: Secretária de Saúde, 2012. Available from:http://www.saude.pr.gov.br/arquivos/File/ACS/linha_guia_versao_final.pdf [ Links ]
28. Liu L, Oza S, Hogan D, Perin J, Rudan I, Lawn JE, et al. Global, regional, and national causes of child mortality in 2000-13, with projections to inform post-2015 priorities: an updated systematic analysis. The Lancet. 2015; 385(9966):430-40. [ Links ]
29. Oliveira E, Souto MB, Santos RA, Fonseca RL, Matos FV, Caldeira AP. Mortalidade infantil evitável em montes claros, Minas Gerais, Brasil, 1999-2011. Rev Baiana Saúde Pública. 2015;39(2):397-407. [ Links ]
30. Chaves LD, Ferreira JBB, Camelo SHH, Balderrama P, Tanaka OU. Reflexões acerca de Sistemas de Informação em Saúde, Pesquisa Avaliativa e Enfermagem. Enfermeria Global. 2014; 13 (2): 303-12. [ Links ]
Received: July 13, 2018; Accepted: October 18, 2018
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
