










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkEnfermería Global
versão On-line ISSN 1695-6141
Enferm. glob. vol.18 no.56 Murcia Out. 2019 Epub 23-Dez-2019
https://dx.doi.org/10.6018/eglobal.18.4.342601
Originals
Quality of life of people with hansen’s disease assisted in a reference hospital, Paraíba-Brazil
1Nurse. Federal Univesity of João Pessoa, Paraíba. Brazil. cibellynf@hotmail.com
2Nurse. PhD in Nursing. Adjunct Professor, Department of Clinical Nursing and Graduate Nursing Program, Health Sciences Center, Federal University of Paraíba. Brazil.
3Nurse. Technical Advisor at the Leprosy and Tuberculosis Coordination at the Municipal Health Secretariat of João Pessoa, Paraíba. Nurse at the Dr. Clementino Fraga Hospital for Infectious Diseases, João Pessoa, Paraíba, Brazil.
4Nurse. Student of the Master course in the Graduate Nursing Program of the Health Sciences Center of the Federal University of Paraíba. Member of the Center for Studies and Research in Bioethics and Palliative Care of the Federal University of Paraíba. Joao Pessoa, Paraiba, Brazil.
5Nurse. Student of the Master course in the Graduate Program in Decision Models and Health of the Federal University of Paraíba. Joao Pessoa, Paraiba, Brazil.
Objective
Evaluate the degree of impairment of the quality of life of people with Hansen’s disease, according to social demographic and clinical variables
Method
Descriptive, transversal, quantitative study, involving 45 patients from a reference hospital located in João Pessoa, Paraíba, Brazil. For obtaining data, interviews were performed based on a semi-structured questionnaire, including social demographic and clinic variables of the participants; to evaluate their life quality the instrument Dermatology Life Quality Index was used, after approval in the Committee of Ethics in Research of the Federal University of Paraíba. In the data analysis, the non-parametric Test of the Chi-square of Pearson was used with level of significance of 5% (p<0,05), being used the Yates correction continuity, when necessary.
Results
It is highlighted a prevalence of male, brown, single, aged 18 to 40 individuals, with family income lower than three minimum salaries and low schooling. From this total, 88,9% presented the clinical multibacillary form of the Hansen’s disease and 60% of them, with level of impairment of quality of life varying between moderate and very serious, according to scores of the instrument used.
Conclusion
It is reassured the important impact of the Hansen’s disease in the quality of life of their carriers, as indicated by the high scores obtained in the application of the DLQI.
Key words: Hansen’s disease; Quality of life; Nursing
INTRODUCTION
The Hansen’s disease is a chronic infectious and contagious disease. It is considered one of the most ancient diseases, which affect men, since 600 B.C., including cases described in the Bible 1. Although it is curable, Brazil is considered the second most endemic country in the world.
The epidemiologic situation of the Hansen’s disease in the country, according to the Secretary of Surveillance in Health of the Ministry of Health Saúde, points that the coefficient of the year 2013 was of 1,42 case at each 10 thousand inhabitants. In 1991, during the 49th World Health Assembly (WHA), it was established as aim by the World Health Organization that the 122 most endemic countries committed with the elimination of the Hansen’s disease as public health problem, when reaching a prevalence inferior to 1 case at each 10 thousand inhabitants 2,3.
The clinical manifestations of the Hansen’s disease are characterized, specially, by the presence of skin lesions, loss of sensibility and neural thickening. It can affect people of all ages, although, it is less frequent in children. There is higher incidence in male people, in most regions of the world 4,5.
For operational purposes, the World Health Organization (WHO) classifies the Hansen’s disease, according to the number of cutaneous lesions and neural damage, in paucibacillary and multibacillary. The specific treatment of Hansen’s disease is made with polychemoteraphy (PCT), globally standardized. The PCT eliminates the bacillus, making it unviable and avoiding the evolution of the disease, preventing the functional alterations, leading to cure when performed correctly and completely4.
Along the years, people affected by Hansen’s disease suffer discrimination by the society. These attitudes, associated to the deformities and mutilations provoked by the disease, generate prejudices which continue to happen until today, affecting negatively the quality of life of people with Hansen’s disease 1.
According to WHO, the term quality of life “[…] refers to the perception of the individual in his or her position in the life in the context of the culture and systems of values in which he or she lives related to their objective, expectancies, patterns and worries”6. The definition considers physical and psychological aspects, independence, social relations, environment, spirituality, religion and personal beliefs. Therefore, a grievance or infirmity might have negative impacts in the quality of life of the people 7.
Aiming objective measures of the problem and their consequences, as well as a better therapeutic approach of patients with Hansen’s disease, some questionnaires that serve as evaluation instruments of the quality of life related to health , specifically for the area of dermatology were developed, with emphasis to the Dermatology Life Quality Index (DLQI), developed by Finlay and Khan, in 1994, in United Kingdom, which was translated and validated to the English language in Brazil by Martins, Arruda and Mugnaini em 2004 (Index of Quality of Life in Dermatology), already known and applied previously, in other dermatological diseases8,9.
The performance of this investigation was justified by the need of assessing how much the Hansen’s disease affects the quality of life of affected people, allowing to display the possibility of impact of the disease in the quality of life of the patients, and, therefore present the results to the managers, to subside actions and strategies to be implemented, as well as to the health professionals involved in the attention to the patients, meaning a holistic and humanized care.
Among these professional the performance of the nurse is highlighted. According to their Professional Ethics Code, he is the one committed to the health and the quality of life of the people, working with autonomy in the promotion, prevention, recovery and rehabilitation of health, having a fundamental role in this process and contributing for a qualified and innovating nursing assistance to the patient with Hansen’s disease 10.
Overall, this study aimed to evaluate the level of commitment of the quality of life of people with Hansen’s disease attended in a Hospital in João Pessoa-PB, according to social demographic and clinical variables.
MATERIAL AND METHOD
It is a descriptive, transversal study, with quantitative 11 approach. The scenery of the research was a hospital institution, of public management, destined to attend patients with infections and parasitic diseases, located in the city of João Pessoa - PB. The choice of the place was due to the fact that the hospital is a reference institution in the treatment of the Hansen’s disease in Paraíba.
The population of this study was composed of 151 patients, registered and attended in the specialized ambulatory in dermatology of the selected institution, in the period of data collection. The sample, obtained by the non-probabilistic technique of convenience, was of 45 participants, who turned up expontaneously, to the outpatient care, during the period from August to September 2016, and that attended to the inclusion criteria: Be 18 years old or more and be in ambulatory treatment for at least one month. On the exclusion criteria, the following issue was listed: the patient had any kind of neurological or psychiatric disorder, which made him impossible to answer precisely the items of the instrument.
The data collection was begun after the approval of the Ethics Committee in Research of the Federal University of Paraíba (UFPB), under protocol number 0314/16, and CAAE nº 56539516.0.0000.5188, with agreement of the Direction of the Institution chosen as scenery of research. It is also highlighted that during all the phases investigated the ethic aspects in researches involving human beings were considered, contained in the Resolution number 466/12, of the National Council of Health12.
In order to obtain the empiric material, a semi structured questionnaire was used, composed of objective and subjective questions, referring to the social demographic and clinical characterization of the participants of the research according to the variables: gender, age, skin colour, marital status, level of education, situation of residence, occupation, family income, operational classification of the Hansen’s Disease, previous understanding on the term quality of life, besides the main difficulties and clinical conditions most affected during the sickness process.
To evaluate the quality of life of the participants of the research a specific instrument for dermatology was used, it was developed by Finlay and Khan in 1994 - Dermatology Life Quality Index DQLI which was translated and validated to the Portuguese language in Brazil by Martins, Arruda and Mugnaini in 20048,9.
The DLQI is composed of 10 multiple-choice questions, divided into six fields: work, leisure, personal relations, treatment, symptoms and feeling, which evaluate the individual from the dermatological point of view and can be used to either measure or compare the quality of life among different skin diseases. The score of the instrument varies from 0-30, when 0 is attributed to the best result and 30 to the worse, being: without impairment of the quality of life (0-1), with mild impairment (2-5), moderated (6-10), severe (11-20) or very severe (21-30). The screening study will bring relevant information regarding the stigma of the Hansen’s disease, attending to the objectives of the research.
The data were submitted to the software SPSS - Statistical Package for the Social Sciences, version 20, aiming to perform the descriptive analysis of the variables studied and testing the hypothesis of possible association between the dependent variable (impairment of the quality of life) and the independent variables (gender, age, skin colour, marital status, school level, family income, operational classification).
To check this possible association, the non-parametric Test of the chi-square of Pearson with significance level of 5% (p<0,05), being used the Correction of Continuity of Yates, when necessary. It is worth to highlight that the dependent variable was reorganized into two categories: without impairment (score from 0 to 1) and with impairment (score of 2 or more).
RESULTS
The results of this investigation were arranged according to the social demographic data (gender, age, skin colour, marital status, school level, family income and occupation) of the interviewee, the clinical aspects related to the operational classification of the Hansen’s disease and to the level of impairment, and also the knowledge about the quality of life and main difficulties lived by the participants.
With regard to the social demographic data, it is emphasized that most of the patients with Hansen’s disease is male (53,3%), aged up to 40 (44,4%), brown (64,5%), single (55,6%), incomplete primary school level (44,4%) and family income ranging between 1 and 3 minimum salaries (53,3%), as show in the Table 1.
Table 1. Distribution of people with Hansen’s disease, according to the social demographic variables. João Pessoa, Paraíba, Brazil, 2016. (N = 45)
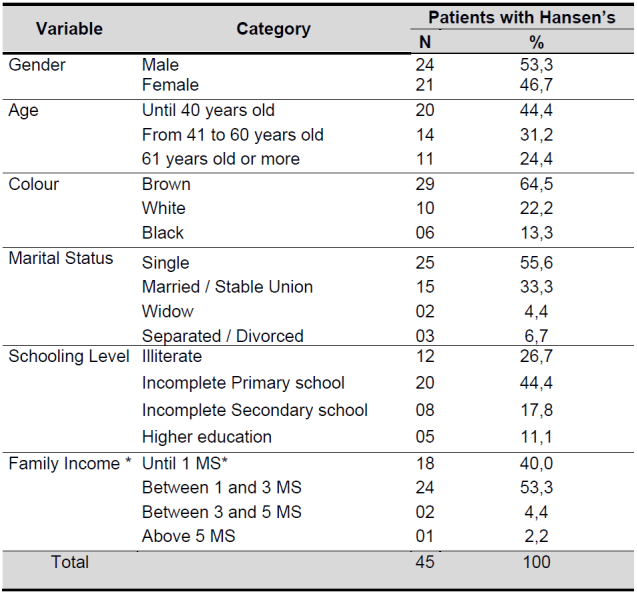
Source: Research data
*MS: Mininum Salary; Current value in the period of the study is R$ 880,00
On the occupation or income source it was observed a higher prevalence of maids (24,4%), followed by retired people (20%), bricklayer’s mates (11,1%), agriculturist (11,1%), student (8,9%), pedagogue (2,2%), among others (22,2%). From the total of patients, 86,7% mention to live in the urban zone and 13,3% in the rural zone.
With regard to the operational classification of the Hansen’s disease it was highlighted the multibacillary form, registered in 88,9% of the participants of this study, which can be seen it Table 2.
Table 2. Distribution of people with Hansen’s disease, according to operational classification. João Pessoa, Paraíba, Brasil, 2016. (N = 45)

Source: Research data
With respect to the evaluation of the quality of life of the people with Hansen’s disease, according to the scores obtained according to the classification of the DLQI, the study showed that 84,4% of the participants presented any type of level of impairment of the quality of life, as exposed in Table 3.
Table 3. Distribution of people with Hansen’s disease, according to level of commitment of quality of life obtained of the instrument DLQI. João Pessoa, Paraíba, Brasil, 2016. (N = 45)

Source: Research data
To the level of 95% of trust there are evidences of the significant association between operational classification of the Hansen’s disease and level of impairment (p=0,024), as exposed in the Table 4.
Table 4. Distribution of the level of impairment of quality of life of the people, according to the operational classification of the Hansen’s disease. João Pessoa, Paraíba, Brasil, 2016. (N=45)

Source: Research data
**Correction of continuity of Yate
However, it was not possible to observe a relation between the impairment of the quality of life and the variables: Gender (p=0,634), Age (p=0,961); Skin colour (p=0,251); Marital status (p=0,183); Education (p=0,777); Family Income Familiar (p=0,074) and Diagnostic Time (p=0,797).
In relation to the understanding of the participants about the meaning of the term quality of life, main difficulties found during the performance of the activities of the daily/social life and about the clinical conditions that affect more their quality of life. This study achieved multiple subjective answers, which varied particularly according to the reality of each individual. However, for a better comprehension of the results we preferred to categorize the answers according to their meaning, putting together the ones with higher similarity, which can be seen on the Chart 1.
Chart 1. Frequency of subjective answers of people with Hansen’s disease, according to knowledge about quality of life and main difficulties lived. João Pessoa, Paraíba, Brazil, 2016. (N = 45)
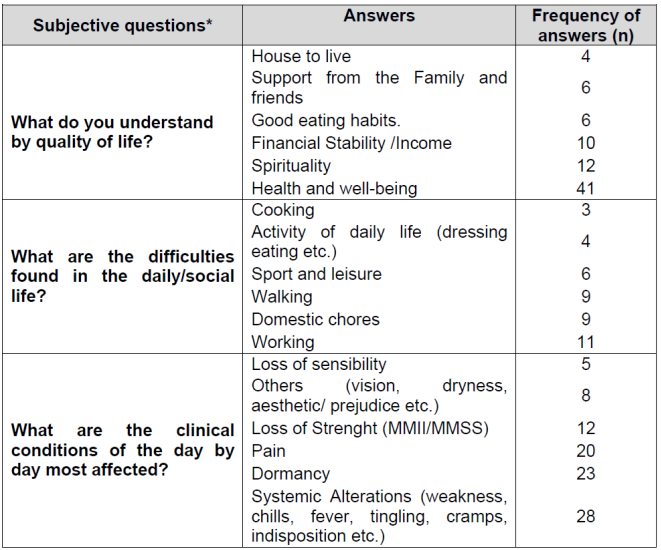
Source: Research data
*Questions which permito ne or more answers.
It is highlighted in 41 of the answers the term ‘health/well-being’, as the most mentioned when it was thought quality of life, followed by spirituality and financial stability.
With regard to the main difficulty found by the participants of the study, during the performance of any daily or social activity, multiple subjective answers were obtained. Notably: Work, perform house chores and walking.
In the aspect clinical condition that most affects the quality of life, the most mentioned were: systemic alterations, dormancy and pain.
DISCUSSION
The result of the research allowed to identify and comprehend how these individuals tried the reality and the impact of the disease in their lives, in a social context with the several complexities that involves them, as there are reports of numerous patients that stopped working and producing due to the pathology.
Reinforcing data found in the literature about the theme, the Hansen’s disease is a disease with high disabling potential, interfering drastically in the work and social life of the patient, which causes big economical losses in the family ambit and psychological traumas4.
As well as in several studies, regarding the demographical characteristics it was checked a predominance of male participants, the same way pointing to a bigger prevalence among young people, average age 40 years old. Most of the individuals said they were brown1,5,13,14.
Highlighting data from previous studies about the theme, the interviewees revealed low education level. Within the illiterates and the ones who had incomplete primary school level were 71,1%. It is important to highlight the low school level of the population studied, as a factor, which implies the dissemination of the disease, as it is known that the Hansen’s disease affects exactly poor populations and with low level of knowledge regarding important actions of prevention against drugs, connected to the aggravating of the poor social condition. Such factors can, somehow, make difficult the access and the apprehension of orientations about the prevention of the disease and complications, treatments and continuous necessary care.
In this study, from the total of interviewees 86,7% answered to have domicile into the urban zone. A very important datum, observing that studies from the Ministry of Health indicate the domicile as being an important space of transmission of the disease. Therefore, right after being diagnosed a case of Hansen’s disease it is recommended that an active search be initiated in the communicating households, aiming to track other possible cases of the disease 4,16.
With regard to the family income, 40% of the investigated of the study in screen live with up to 1(one) minimum salary, which is equivalent to R$ 880,00 per month. It is considered one of the most used social economic indicators to identify and elaborated the Human Development Index (HDI) of 2013, Brazil occupies the 79th position among 187 countries in the world ranking. Therefore, according to the document, 7,4% of the Brazilians are classified in the index as population almost in multidimensional poverty and that “suffers privation” in health, education and income17.
However, the income source from labour and from the workforce is one of the most important factors, which interferes directly in the quality of life of the people with Hansen’s disease. Either regarding reduced or impeded labour capacity, or, principally, for being ta contingent that, most of the times, does not have other income, but the physical force to get conditions of living. Over all, among the most mentioned professions by the interviewees are: maids, bricklayer’s mates and agriculturists. Therefore, associated to several other components, it is difficult to change the professional activity and relocation in the working market 15,18.
Regarding to the operational classification of the Hansen’s disease, it was observed in this research the predominance of multibacillary cases with higher level of impairment of quality of life, corroborating with data presented by other studies about this same thematic 1,13,15.
The scores obtained in the evaluation of patients according to the DLQI ranged from 0 to 27. From the total of the sample most of the patients (84,4%) presents, according to the instrument, any level of impairment of the quality of life. From these, 31,1% with severe impairment and 15,6% did not present impairment of the quality of life. This may be caused by the impact of the involvement of the Hansen’s disease in the activities of life of the ill people, interfering in the interaction of the individuals with the environment where they are inserted, as shown in a study which evaluates the impact of diseases in the activities of life of the people that suffer with these grievances 19.
With regard to the subjective answers of the interviewees on understanding about the term quality of life, there has been bigger frequency of participants that associated the terms health and well-being. In the previous century, the World Health Organization (WHO) clarified that the health must be understood in an expanded form, going through all the human dimensions, which corroborates with the improvement of the quality of life of the people. In this sense, due to the advances in the field of the health sciences, the quality of life of the human being has been the object of the intervention of several social sectors, associating health and well-being to the quality of life of the population, as the empiric idea of the collaborators of this study is shown 20,21,22.
With regard to the main difficulties faced by the participants during any activity of the social/daily life, multiple answers were obtained. Among the most mentioned are: the daily life activities, emphasizing the difficulty to work, walk and perform house chores. Previous study, performed in two deactivated colonies in the eighties and that continue to attend patients remaining the institutionalization, confirms this finding, confirming that the physical incapacities are risk factors for worsening in the quality of life of these individuals23.
Regarding the clinical conditions which most affect the quality of life of the Hansen’s disease patients, several systemic alterations were mentioned, highlighting dormancy and loss of motor strength in upper and lower limbs, accompanied by pain and loss of sensibility. This relation will be influenced by the capacity that the individual will present facing the grievance, as in some patients the minimum interference coming from symptoms can cause negative effects, in other individuals can react differently facing the interference of this symptoms24.
Regarding the psychological dimension, the quality of life of people with Hansen’s disease can be reached negatively, as the society configures an aesthetic paradigm focused on the beauty and physical integrity, which can be changed due to the disease 13,14. Besides this, historically, as in many places, for centuries, the disease was considered a maximum punishment coming from God, configuring, yet in modernity, as an archaic idea of the involvement from guilt and spiritual unhappiness25.
Overall, it is necessary to highlight the high level of clinical impairment observed among the participants of this study and with consequent impact of varied levels in their quality of life, with impairments for its functionality, sociability, as well as self-esteem. Such results emerge reflections on the actions which are being implemented in the attention to the health of the patients in the diverse assistance scenarios, as well as to search effective and efficient strategies that change this reality.
It is highlighted as limitation of this study the fact of it having a transversal character and uses a sample on demand of service in a centre of reference, which results may not reflect all the universe of the community who suffers the infection studied. However, it is conjecture the necessity of increasing and improving the attention to health of people with Hansen’s disease, above all regarding the care to the dimensions committed of these patients, through interventions in the ambit of the health articulated to the public policies, aiming to improve the quality of life. It is emphasized, therefore, the necessity of other studies, broader, regarding the theme, involving participants and diversified regions.
CONCLUSION
Based on the interpretation of data from this study, it is reaffirmed the important impact of the Hansen’s disease in the quality of life of the people infected, as indicated by the high scores obtained in the application of the DLQI. It is shown the direct relation of the occurrence of Hansen’s disease, mostly, males, with operational multibacillary classification, in adverse social economic conditions, highlighted by low family income per capita monthly, low scholar level and precariousness of the relations of work in the participating population, found this in accordance to what is described in the literature on the evident theme.
The evaluation of the quality of life from the specific point of view of the “Dermatology Life Quality Index” - DLQI showed that the patients classified as multibacillary presented important involvement of the quality of life, showing the highest scores in level of involvement if compared to the paucibacillars.
It is necessary to turn the attention of the health professionals to recognize the impairment of the quality of life, especially in those patients classified as multibacillary Hansen’s disease, so that actions and care be implemented focusing on the necessities in their diverse dimensions, general state of health, pain, physical, psychological, social, emotional, functional aspects, vitality, spirituality and mental, personalizing the health care individually and integrally of the human being.
It is also important to highlight that it is necessary new studies which can be developed in other levels of attention, aiming to understand how the Hansen’s disease interferes in everyday life of the people with the disease in the several social strata, because, as indicated in this study, the Hansen’s disease interferes in several dimensions of the quality of life of the people, who suffer as a result of the infection.
This study enables evidences that information on life quality can be useful to evaluate and increase the effectiveness of the treatments that aim not only the biological necessities and the grievances to the health, but, also associate to the physical and psychosocial impact, contributing to the improvement of the service rendered to the patients, in several services of the Attention to the Healthcare network.
REFERENCIAS
1. Budel AR, Costa CF, Pedri LE, Raymundo AR, Gerhardt C. Profile of patients affected by Hansen's disease seen at the Outpatient Clinic of Dermatology at Hospital Evangélico de Curitiba. An Bras Dermatol. [Internet]. 2011 [cited 2018 Jul 14]; 86(5):942-6. Available from: http://dx.doi.org/10.1590/S0365-05962011000500012 [ Links ]
2. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Boletim epidemiológico. Brasília. [Internet]. 2013 [cited 2018 Jul. 12]; 44(11): 1-12. Available from: http://portalarquivos2.saude.gov.br/images/pdf/2014/junho/11/BE-2013-44--11----Hanseniase.pdf [ Links ]
3. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância das Doenças Transmissíveis. Informe Técnico. Campanha Nacional de Hanseníase, Verminoses, Tracoma e Esquistossomose [Internet]. apr. 2015 [cited 2018 Jan 18]; 1-17. Available from: http://portalarquivos2.saude.gov.br/images/pdf/2015/agosto/19/Informe-Campanha-2-2015-maio.pdf [ Links ]
4. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Guia de vigilância em saúde. 2a ed. [Internet]. 2017 [cited 2018 Jul 12]; 287-318. Available from: http://portalarquivos.saude.gov.br/images/pdf/2017/outubro/06/Volume-Unico-2017.pdf [ Links ]
5. Bezerra PB, Silva MCL, Andrade MCF de et al. Avaliação física e funcional de pacientes com hanseníase. Rev enferm UFPE on line. [Internet]. sep. 2015 [cited 2018 Jul 14]; 9(8):9336-42. Available from: https://doi.org/10.5205/reuol.6812-75590-1-ED.0908sup201501 [ Links ]
6. World Health Organization. WHOQOL: measuring quality of life. [Internet]. 1997 [cited 2018 Jun 11]; 1-12. Available from: http://www.who.int/iris/handle/10665/63482 [ Links ]
7. Dolenz MFA, Silva NMMG, Melo SCCS et al. Avaliação da qualidade de vida dos pacientes durante o tratamento e Hanseníase. Rev Odontologia (ATO). apr. 2014 [cited 2018 Jul 14]; 14(4):238-56. Disponível em: https://www.researchgate.net/profile/Natalia_Guerra-Silva/publication/281108669_Avaliacao_da_qualidade_de_vida_dos_pacientes_durante_o_tratamento_de_hanseniase/links/55d5e35f08aed6a199a2c7da/avaliacao-da-qualidade-de-vida-dos-pacientes-durante-o-tratamento-de-hanseniase.pdf [ Links ]
8. Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI) - a simple practical measure for routine clinical use. Clinical and Experimental Dermatology. [Internet]. 1994 [cited 2018 Jul 14]; 19:210-16. Available from: https://doi.org/10.1111/j.1365-2230.1994.tb01167 [ Links ]
9. Martins GA, Arruda L, Mugnaini ASB. Validation of life quality questionnaires for psoriasis patients. An Bras Dermatol. [Internet]. 2004 [cited 2018 may 19]; 79(5):521-535. Available from: http://dx.doi.org/10.1590/S0365-05962004000500002 [ Links ]
10. Conselho Federal de Enfermagem. Resolução cofen nº 564/2017. Aprova o novo código de ética dos profissionais de enfermagem. [Internet]. 2017 [cited 2018 may 19]; Available from: http://www.cofen.gov.br/resolucao-cofen-no-5642017_59145.html [ Links ]
11. Prodanov CC, Freitas EC. Metodologia do trabalho científico: métodos e técnicas da pesquisa e do trabalho acadêmico. Novo Hamburgo: Feevale; 2013; 52-70. Disponível em: http://www.feevale.br/Comum/midias/8807f05a-14d0-4d5b-b1ad-1538f3aef538/E-book%20Metodologia%20do%20Trabalho%20Cientifico.pdf [ Links ]
12. Brasil. Ministério da Saúde. Conselho Nacional de Saúde. Resolução 466/2012. Aprova diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos. Brasília: MS. [Internet]. 2012. [cited 2018 Jan 14];. Available from: http://bvsms.saude.gov.br/bvs/saudelegis/cns/2013/res0466_12_12_2012.html [ Links ]
13. Araújo DAL; Brito KKG; Santana EMF; et al. Characteristics of people of quality of life with leprosy in outpatient treatment. Rev Fund Care. [Internet]. 2016 [cited 2018 may 19]; 8(4):5010-16. Available from: https://doi.org/10.9789/2175-5361.2016.v8i4.5010-5016 [ Links ]
14. Quaggio CMP, Virmond M, Guimarães HCQCP. Qualidade de vida da pessoa tratada da hanseníase. Hansen Int. [Internet]. 2014 [cited 2018 jul 14]; 39(2):36-46. Available from: http://www.ilsl.br/revista/detalhe_artigo.php?id=12347# [ Links ]
15. Ribeiro GC, Lana FCF. Incapacidades físicas em hanseníase: caracterização, fatores relacionados e evolução. Cogitare Enfermagem. [Internet]. 2015 [cited 2018 may 19]; 20(3): 496-503. Available from: http://www.redalyc.org/articulo.oa?id=483647680006 [ Links ]
16. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Diretrizes para vigilância, atenção e eliminação da Hanseníase como problema de saúde pública: manual técnico-operacional. [Internet]. 2016 [cited 2018 apr 25]; 58. Available from: http://portal.saude.pe.gov.br/sites/portal.saude.pe.gov.br/files/diretrizes_para_._eliminacao_hanseniase_-_manual_-_3fev16_isbn_nucom_final_2.pdf [ Links ]
17. Programa das Nações Unidas para o Desenvolvimento [internet] 2016 [cited 2018 jul 14]; Available from: http://report.hdr.undp.org [ Links ]
18. Neto DL, Araújo RO, Meneghini MEF, Tsuzuki LM. Avaliação da qualidade de vida em pacientes com hanseníase: uso do Medical Outcomes Study 36. Brazilian Journal of Health Research [Internet]. 2015 [cited 2018 ago 14]; 17(1), 6-10. Available from: http://periodicos.ufes.br/RBPS/article/view/12454/8664 [ Links ]
19. Rosenblum S, Josman N, Toglia J. Development of the Daily Living Questionnaire (DLQ): A Factor Analysis Study. The Open Journal of Occupational Therapy. [Internet]. 2017 jan. [cited 2018 aug 25]; 5 (4):1-17. Available from:https://scholarworks.wmich.edu/ojot/vol5/iss4/4/ [ Links ]
20. Minayo MCS, Hartz ZMA, Buss PM. Qualidade de vida e saúde: um debate necessário. Ciência & Saúde Coletiva [Internet]. 2000 [cited 2018 aug 25]; 5(1):7-18. Available from: http://dx.doi.org/10.1590/S1413-81232000000100002 [ Links ]
21. Herbias LH, Soto RA, Figueroa HB, Reinoso LA. Significado de calidad de vida en pacientes con terapia de hemodiálisis: un estudio fenomenológico. Enferm Nefrol [Internet]. 2016 [cited 2018 aug 25];19(1):37-44. Available from: http://scielo.isciii.es/pdf/enefro/v19n1/05_original4.pdf [ Links ]
22. Damásio BF, Melo RLP, Silva JP. Meaning in Life, Psychological Well-Being and Quality of Life in Teachers. Paidéia. [Internet]. Jan/apr. 2013 [cited 2018 aug 25]; 23(54):73-82. Available from: http://dx.doi.org/10.1590/1982-43272354201309 [ Links ]
23. Leite IF, Arruda AJCG, Vasconcelos DIB, Santana SC, Chianca KSV. The quality of life of patients with chronic leprosy. Journal of Nursing UFPE on line. [Internet]. Jun. 2015 [cited 2018 aug 26]; 9(6):8165-71. Available from: http://doi.org/10.5205/reuol.7585-66362-1-ED.0906201503 [ Links ]
24. Amorim AAS, Pereira ISSD, Silva Júnior EG. Analysis of the quality of life of patients afflicted with leprosy. Journal of Infection Control. [Internet]. 2016 [cited 2018 aug 26]; 5(4):1-12. Available from: http://jic-abih.com.br/index.php/jic/issue/view/27 [ Links ]
25. Luker V, Buckingham J. Histories of Leprosy: Subjectivities, Community and Pacific Worlds. The Journal of Pacific History. [Internet]. 2017 [cited 2018 aug 26]; 52(3):265-86. Available from: https://doi.org/10.1080/00223344.2017.1379124 [ Links ]
Received: September 19, 2018; Accepted: November 05, 2018
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
