










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.18 n.56 Murcia Oct. 2019 Epub Dec 23, 2019
https://dx.doi.org/10.6018/eglobal.18.4.348451
Originals
Epidemiological profile of congenital syphilis in a microregion inside the state of Bahia (2007-2017)
1Graduing from the Biomedicine course at FG University Center, Guanambi, BA, Brazil.
2Master in Environmental Sciences and Health from PUC-GO and professor at FG University Center, Guanambi, BA, Brazil.
Objective
To analyze the epidemiological profile of Congenital Syphilis in 18 municipalities in the state of Bahia between 2007 and 2017.
Method
A descriptive, cross-sectional and quantitative study of the confirmed cases of Congenital Syphilis in the micro-region registered in the Aggravation and Notification Information System.
Results
In the study period, 39 cases were confirmed, with 30.8% of the mothers being between 20 and 24 years of age, 59% were brown, 46.2% had incomplete primary education, 33.3% were housewives, 74.4% 94.9% underwent prenatal care, 53.8% were diagnosed at the time of delivery / curettage, 41% received inadequate treatment and 38.5% of the partners were not treated. With regard to newborns, 69.2% were diagnosed with 0 day of life, 74.4% with recent Congenital Syphilis and 46.2% asymptomatic.
Conclusion
The data reveal a serious public health problem in the micro-region analyzed, also pointing out failures in the notification system, observed in the high ignored index in the studied variables.
Key words: Epidemiology; Prenatal; Congenital syphilis; Infection
INTRODUCTION
Syphilis is a sexually transmitted infection (STI) of a systemic nature, caused by the bacterium Treponema pallidum that can be transmitted sexually, characterizing it as syphilis acquired, vertically (congenital), by blood transfusion or contaminated objects.1
Treponema pallidum is a spirochete that through its cytosines has the ability to tolerate the maternal immune system and progress to an infection to the fetus (2). The fact that infection with the baby provides an important relation to morbidity in children and perinatal mortality, since even being a Compulsory Notification infection, it still shows a serious public health problem.3
Congenital syphilis (CS) is divided into two periods depending on the time at which the first signs and symptoms appear, and may be early, more recent, and later after some years of life.1
Generally the number of cases of syphilis is different depending on the per capita income of each country, according to the literature4 low and middle income countries have more than 100 cases per 100,000 live births more than high income countries.
In a survey published by the World Health Organization in 2015, the country with the highest number of cases of SC in 2014 was Equatorial Guinea with a rate of 1233.5 cases per 100,000 live births, followed by Brazil with 472.2 per 100,000 live births, Paraguay with 424.1 per 100,000 live births, and Mozambique with 417.5 per 100,000 live births respectively.5
Given this scenario, WHO establishes a CS elimination plan, where countries to receive the target seal must have a maximum rate of up to 50 cases per 100,000 live births.5
In 2013, the cases of syphilis in pregnant women in Brazil reached 21,382, and the transmission rate from mother to fetus was 4.7% for every 1,000 live births.6 Between 2013 and 2016, the country underwent an intense process of progression in relation to the number of cases of SC, which went from 13,968 cases in 2013 to 20,474 cases in 2016.7
In Bahia in 2016, 1,388 cases of CS were reported, as the state of Bahia ranks 12th in the ranking of states with the highest mortality rates for SC in children under one year of age, with a rate of 7.7. /100.00 live births.7
Having this perspective, the present study aims to analyze the epidemiological profile of SC in 18 municipalities in the interior of the state of Bahia, in the time frame from 2007 to 2017.
METHODOLOGY
The research refers to a descriptive, cross-sectional and quantitative study of the cases.
CS in Guanambi microregion in the state of Bahia from 2007 to 2017. The microregion is located in the upper Bahian hinterland that comprises 18 municipalities, including: Guanambi, Caetité, Riacho de Santana, Caculé, Igaporã, Malhada, Palmas de Monte Alto, Pindaí, Urandi, Candiba, Ibiassucê, Iuíu, Jacaraci, Lagoa Real, Licínio de Almeida, Matina, Mortugaba and Sebastião Laranjeiras with about 374,180 inhabitants.8
The data collection was performed through surveys of confirmed cases of SC that are available in the Health and Notification Information System (SINAN) linked to the Department of Informatics of the Unified Health System (DATASUS), and included in the study all confirmed cases of CS in microregion and 2 cases excluded because reporting municipalities are not included in the microregion.
For data analysis, the variables used for maternal characteristics were: age, race / color, education, occupation, area of residence, prenatal care, time of diagnosis, treatment of pregnant woman and treatment of partner. Regarding the characteristics of the newborn, the child's gender, age at diagnosis, final classification, case evolution and presence of signs and symptoms were analyzed.
Data were organized and tabulated in Office Excel (Microsoft®) 2013 where tables and graphs were generated, which also performed the analysis of the percentages of each variable. Statistical analysis was performed using the BioEstat 5.3 software, which used the Chi-square test and Fisher's test, with a significance level of 5% (p <0.05), and was also used to perform the deviation. default for the other variables.
The entire study was conducted on ethical care, based on National Health Council Resolution No. 510/2016 (9). Thus, as it deals with secondary and public domain data, submission to the Research Ethics Committee is not required (REC).
RESULTS
This study consisted of 39 reported and confirmed cases of CS between 2007 and 2017 in the micro region of Guanambi - Bahia. Within the historical cut analyzed there is an increase in the number of cases of SC in the Guanambi microregion, where from 2014 this growth becomes even more intense being 2016 (n = 10) and 2017 (n = 11) ( Figure 1) The years that had the highest elevations. In this same temporary cut most pregnant women did not have adequate treatment during prenatal care, where, the same years that presented higher increases in the number of cases showed only 1 report of adequate treatment each year, emphasizing that the lack of adequate treatment. promotes an uncontrolled number of cases of SC.
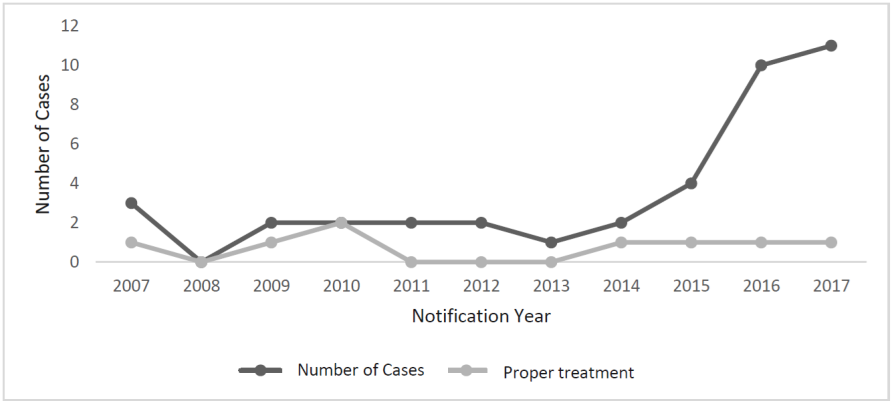
Source: SINAN, 2018 (Notification Disease Information System).
Figure 1. Number of cases of Congenital Syphilis between 2007 and 2017 in the Guanambi microregion.
When analyzing the rate of CS cases in relation to age group (Table 1), there is a frequency expressed in cases of pregnant women between 20 and 24 years old (30.77%). Regarding the race / color variable, there is a predominance of browns with 58.97% of cases. Mothers' education and occupation were ignored with 25.64% and 51.28%, respectively. Still, most mothers live in urban areas with percentages of 74.36% of cases.
Table 1. Distribution of maternal sociodemographic characteristics of reported and confirmed cases of congenital syphilis in the Guanambi microregion, 2007-2017.

Source: SINAN, 2018 (Notification Disease Information System).
*They did not compose the statistical analysis.
SD (Standard Deviation).
Regarding the care characteristics of mothers of newborns (Table 2), 95% of pregnant women had prenatal care, however 53.8% of pregnant women were diagnosed with CS during childbirth. Regarding the treatment of pregnant women 38.46% had inadequate treatment and 38.5% of partners of pregnant women did not receive treatment.
Table 2. Distribution of characteristics of prenatal care of mothers of newborns notified and confirmed with congenital syphilis in the Guanambi microregion, 2007-2017.

Source: SINAN, 2018 (Notification Disease Information System).
*They did not compose the statistical analysis. SD (Standard Deviation).
Regarding the frequency of the number of cases of CS in newborns, males were the ones who expressed the highest amount (53.8%) (Table 3), since all cases were diagnosed with less than one year of life, thus favoring a higher elevation of recent CS in the final disease classification variable. Regarding the evolution of the case and the presence of signs and symptoms, reports of living and asymptomatic patients were the ones who expressed the highest percentages, presented: (89.7%) and (46.2%) consecutively.
Table 3. Distribution of demographic and care characteristics of newborns notified and confirmed with congenital syphilis in the Guanambi microregion, 2007-2017.

Source: SINAN, 2018 (Notification Disease Information System).
*They did not compose the statistical analysis.
SD (Standard Deviation).
Regarding the diagnosis of CS 64.1% of the non-treponemal tests at the time of delivery / curettage were reactive and only 2.6% non-reactive (Table 4), regarding the child and the non-treponemal blood test. 79.5% were reagents. Regarding the therapeutic scheme of SC, most cases were treated with crystalline penicillin g (46.2%).
Table 4. Distribution of the characteristics related to the diagnosis and treatment of confirmed cases of congenital syphilis in the Guanambi microregion, 2007-2017.

Source: SINAN, 2018 (Notification Disease Information System).
*They did not compose the statistical analysis.
**Test not applied.
SD (Standard Deviation).
DISCUSSION
Within the historical background analyzed there is an increase in the number of cases of SC in the microregion, such results are correlated with research conducted in a municipality in the interior of the state of Rondônia and research conducted in Canada.10,11
Improving the effectiveness of epidemiological reporting of CS cases is one of the factors contributing to the increase in the number of annual CS cases, as in recent years women have become increasingly interconnected with seeking antenatal consultations.12
Regarding the age group, the result is similar to the epidemiological study of CS carried out in the municipality of Sobral state of Ceará, as well as in a study conducted in Canada.13,11 This high percentage of CS cases over the age of 18 may be suggested due to the high prevalence of pregnant women in this age group, as well as the possibility of multiple partners and unprotected sex.8,14
Regarding the race / color variable, this result is justified because the process of miscegenation favors the mixing of various ethnicities, races and colors. Compared to other epidemiological studies, there is a remarkable parity in the values seen in the municipality of Ji-Paraná - RO and Jequié - BA.10,15
The level of education and occupation were ignored, which is similar to a study carried out in the state of Paraná between 2007 and 2013 (13). This increase in the proportion of the number of ignored may be suggested most of the time due to the poor quality of the notification form, thus compromising the data analysis and thus undermining the infection prevention, control and reduction process.15
However, it is important to point out the importance in the high percentage of the number in relation to women who have not completed elementary school, highlighting that the result of the present study is similar to research conducted in Porto Velho - RO and Palmas - TO.16,17 The level of education is a criterion that directly affects the prevalence of CS, since treatment often becomes impaired due to the lack of adequate information about proper care or because they are unaware of their own importance, thus showing a public health problem.18
As for the area of residence, the highest percentage observed was in the urban area, this predominance may be justified because most of the population in both Brazilian municipalities and municipalities of other countries, such as Canada, reside in cities, since The use of drugs related to the urban area is also one of the factors that favor the increased exposure of the infection and the transmission of CS.19,20 Comparing the present result with research carried out in Sobral - CE and in the state of Rio Grande do Norte between 2007 and 2010, a similarity is evident in the mentioned zone.13,21
The finding on the care characteristics of the mothers of newborns, where most of them attend prenatal care, corroborates studies conducted in the states of Ceará and Mato Grosso.13,14 The results of the study demonstrate an effectiveness in the acceptance of monitoring by mothers during the gestational period, thus proving the applicability of prevention programs implemented by the Ministry of Health.22
With regard to the moment of diagnosis, the largest record of cases during childbirth stands out, a situation similar to that found in the state of Alagoas from 2007 to 2011.14
It is also evident that most pregnant women received inadequate treatment for the disease and their partners were not treated, similar data can be seen in others as for example in a survey conducted in Jequié - BA.15
According to studies, prenatal care is the most opportune time to treat the partners of infected pregnant women, thus preventing the reinfection of women, as well as reducing and controlling syphilis.1 Thus, the need for care improvements directed to partners is under discussion, given that the treatment of women together with their partner is extremely important in reducing the incidence of CS cases, thus, the chances of reinfections significantly reduce.17
Male newborns were more affected, however, this variable has no clinical or epidemiological significance, considering that infection by Treponema pallidum is not selective regarding the sex of the conceptus, ie both sexes may equally acquire the disease.14
It is noted that newborns with SC were diagnosed at 0 days of life and 100% under 1 year, similar to what is shown in a study in the southern municipality of Mato Grosso,14 as well as newborns. reported, the frequency was higher in asymptomatic patients, similar to the findings in Montes Claros-MG.1 Most newborns diagnosed with CS are asymptomatic, thus reinforcing the need for more accurate monitoring and correct serological screening of pregnant women during pregnancy.1
Regarding the diagnosis of maternal and newborn CS, most mothers had a positive VDRL at the time of delivery / curettage, and in the peripheral blood the non-treponemal test of the newborns was reactive, showing similarity. with data presented in another study in Brazil.23
Observing the diagnostic characteristics adopted, most newborns were treated with crystalline Penicillin g, a result similar to that reported in studies in the city of Rondonópolis-MT.14 Nevertheless, 35.9% underwent another therapeutic regimen. Among those informed, the use of ceftriaxone was predominant in different dosages, possibly due to allergic reactions to the use of penicillin.14
CONCLUSION
Given the data presented, there is a serious public health problem in the analyzed micro-region, highlighting failures in maternal care, both in diagnosis and in the management of pregnant women during prenatal care, making necessary measures that enable insertion of pregnant women in effective control programs, as well as in the training of agents and professionals involved in this process.
Also noteworthy is the large number of cases ignored, indicating a failure in the notification system by the epidemiological surveillance of each municipality involved in the study. Such failure implies the reliability of the data presented, making it necessary to conduct further studies on the subject.
REFERENCIAS
1. Lafetá KRG, Martelli Júnior H, Silveira MF, Paranaíba LMR. Sífilis materna e congênita, subnotificação e difícil controle. Revista Brasileira de Epidemiologia. 2016 Mar; 19(1): 63-74. DOI: http://dx.doi.org/10.1590/1980-5497201600010006 [ Links ]
2. Ribeiro ATB, Jacociunas LV. A coinfecção sífilis/hiv e sua importância no rastreamento sorológico em bancos de sangue. Clinical & Biomedical Research. 2016; 36(2): 101-109. DOI: http://dx.doi.org/10.4322/2357-9730.63878 [ Links ]
3. Saraceni V, Miranda AE. Relação entre a cobertura da Estratégia Saúde da Família e o diagnóstico de sífilis na gestação e sífilis congênita. Cadernos de Saúde Pública. 2012 Mar; 28(3): 490-496. [ Links ]
4. Kojima N, Klausner JD. An Update on the Global Epidemiology of Syphilis. Current Epidemiology Reports. 2018 Fev 19; 5(1): 24-38. DOI em: http://dx.doi.org/10.1007/s40471-018-0138-z [ Links ]
5. World Health Organization. Report on global sexually transmitted infection surveillance. Geneva: WHO, 2015. [ Links ]
6. Monteiro MOP, Costa MCO, Vieira GO, Silva CAL. Factors associated with the occurrence of syphilis in adolescents male, female and pregnant women in a Municipal Reference Center/MRC - STD /HIV/AIDS of Feira de Santana, Bahia. Adolescência & Saúde. 2015; 12(3): 21-32. [ Links ]
7. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Sífilis 2017. Boletim Epidemiológico, Brasília, v 48, n 36, set. 2017. [ Links ]
8. Oliveira TJ, Rios MA, Teixeira PN. Mortality of women of childbearing age in the health region of Guanambi/BA. O Mundo da Saúde. 2017 Dez 31; 41(4): 711-719. DOI: http://dx.doi.org/10.15343/0104-7809.20174104711719 [ Links ]
9. Brasil. Ministério da Saúde. Conselho Nacional de Saúde. Resolução Nº 510, de 7 de abril de 2016. Normas regulamentadoras de pesquisa envolvendo seres humanos. 24 maio. 2016. Seção 1 p. 44-46. [ Links ]
10. Travaim SF, Machado BS, Domingues BS, Morais LI, Alves HNS, Pereira GCA, et al. Analysis of the epidemiological profile of the cases of syphilis notified in the municipality of Ji-Paraná in the period from 2012 TO 2016. Brazilian Journal Of Surgery And Clinical Research. 2018 Fev; 21(2): 42-46. [ Links ]
11. Choudhri Y, Miller J, Sandhu J, Leon A, Aho J. Infectious and congenital syphilis in Canada, 2010-2015. Canada Communicable Disease Report. 2018 Fev 1; 44(2): 43-48. DOI: http://dx.doi.org/10.14745/ccdr.v44i02a02 [ Links ]
12. Benito LAO, Souza WN. Perfil epidemiológico da sífilis congênita no Brasil no período de 2008 a 2014. Universitas: Ciências da Saúde. 2016 Dez 27; 14(2): 97-104. DOI: http://dx.doi.org/10.5102/ucs.v14i2.3811 [ Links ]
13. Lima VC, Mororó RM, Martins MA, Ribeiro SM, Linhares MSC. Journal of Health & Biological Sciences. J Health Biol Sci. 2017; 5(1): 56-61. DOI: http://dx.doi.org/10.12662/2317-3076 [ Links ]
14. Silva LCVG, Teodoro CJ, Silva JK, Santos DAS, Olinda RA. Profile of the cases of syphilis in a municipality the south of Mato Grosso. Journal Health Npeps. 2017; 2(2): 380-390. [ Links ]
15. Teixeira MA, Santos PP, Santos PN, Araújo RT, Souza AGJ. Epidemiological and sociodemographic profile of children infected congenital syphilis in Jequié/Bahia. Rev saúde com. 2015 Nov; 11(3): 303-313. [ Links ]
16. Moreira KFA, Oliveira DM, Alencar LN, Cavalcante DFB, Pinheiro AS, Orfão NH. Perfil dos casos notificados de sífilis congênita. Cogitare Enfermagem. 2017 Mar 27; 22(2): 01-10. [ Links ]
17. Cavalcante PAM, Pereira RBL, Castro JGD. Sífilis gestacional e congênita em Palmas, Tocantins, 2007-2014. Epidemiologia e Serviços de Saúde. 2017 Mar; 26(2): 255-264. DOI: http://dx.doi.org/10.5123/s1679-49742017000200003 [ Links ]
18. Amâncio VC, Graciano AR, Cozer AM, Assis LPF, Dias DCS. Epidemiology of congenital syphilis in the state of Goiás. Educação em Saúde. 2016; 4(2): 58-62. [ Links ]
19. Venturi G. Consumo de drogas, opinião pública e moralidade: Motivações e argumentos baseados em uso. Revista de Sociologia da Usp. 2017 Ago 8; 29(2): 159-186. DOI: http://dx.doi.org/10.11606/0103-2070.ts.2017.126682 [ Links ]
20. Barbosa AS, Bruna GC. Estratégias de projeto e intervenção nas metrópoles contemporâneas: experiências e perspectivas, 4 colóquio brasil - Portugal, 2016, São Paulo, Sp. Os princípios de urbanização segundo o prof. Manuel da Costa Lobo e sua aplicação no Canadá: o projeto urbano de Angus, Ontario. São Paulo, Sp: Mackenzie, 2016. 16 p. [ Links ]
21. Carvalho IS, Brito RS. Sífilis congênita no Rio Grande do Norte: estudo descritivo do período 2007-2010. Epidemiologia e Serviços de Saúde. 2014 Jun; 23(2): 287-294. DOI: http://dx.doi.org/10.5123/s1679-49742014000200010 [ Links ]
22. Brasil. Ministério da Saúde. Manual Técnico para Diagnóstico da Sífilis. Brasília, 2016, 54p. [ Links ]
23. Alves WA, Cavalcante GR, Nunes FA, Teodoro WR, Carvalho LM, Domingos RS. Congenital Syphilis: Epidemiology of Cases Notified, Alagoas, Brazil, from 2007 to 2011. Revista Portal Saúde e Sociedade. 2016; 1(1): 1-15. [ Links ]
Received: November 04, 2018; Accepted: February 06, 2019
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
