










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkEnfermería Global
versão On-line ISSN 1695-6141
Enferm. glob. vol.18 no.56 Murcia Out. 2019 Epub 23-Dez-2019
https://dx.doi.org/10.6018/eglobal.18.4.341611
Originals
Effects of motivational interviewing on cardiovascular patient adherence
1Master in Nursing National University of Colombia. Assistant Professor Faculty of Pontifical Nursing Universidad Javeriana. Colombia. achuryl@javeriana.edu.co
Objective
To determine the effect of motivational interviewing, a nursing strategy, on adherence to treatment in patients who have suffered acute myocardial infarction and attend phase II in a cardiac rehabilitation program in Bogota.
Method
This research used a quasi-experimental design that had a nursing strategy based on motivational interviewing as its independent variable and adherence to treatment as its dependent variable. The control group (n=22) received the usual intervention in the cardiac rehabilitation program, while the experimental group (n=22) additionally received one weekly nursing intervention session of motivational interviewing during a three-week period. Three measures of adherence to treatment were taken: the first at the beginning of the study, the second, one week after the intervention had finished, and the third, five weeks after the intervention had finished.
Results
Inter-group analysis showed statistically significant changes only in the third measurement of the dimension that refers to the management of tense situations (p=0.013). Nevertheless, intra-group analysis showed statistically significant differences for the experimental group in their global results for treatment adherence (p=0.007) and in the expectations/self-efficacy behavior (p=0.013), as well as for the need of support for treatment adherence (p=0.013) five weeks after the intervention had finished.
Conclusion
Motivational interviewing seems to be a promising strategy for treatment adherence in patients who have suffered acute myocardial infarction. Therefore, it is advisable to continue researching in the field, so that results derived from intervention can be standardized.
Keywords: compliance of medication; cardiovascular nursing; motivational interview; myocardial infarction; self-efficacy
INTRODUCTION
Despite the implementation of several strategies for health promotion and illness prevention, nowadays, cardiovascular diseases are still among the major causes of morbidity and mortality at a national and international level. According to the statistics offered by the Global Burden of Disease study, by 2016, cardiovascular diseases were the cause of 17.33% of the world general death rate ,1.
Furthermore, coronary disease is the most frequent death cause in all countries. According to the American Heart Association (AHA), out of the 85.6 million American adults who are diagnosed with at least one cardiovascular disease, 15.5 million suffer from coronary disease 2. In Colombia, according to the Figures of the National Administrative Department for Statistics (DANE for its name in Spanish), the ischemic heart disease is the main cause of death in people over the age of 45, which caused 8,403 deaths in 2015 3.
Acute myocardial infarction triggers important consequences at physical, psychological and social levels, which limit the natural development of everyday activities 4. Patients suffer from a reduction in their physical capabilities, which has emotional outcomes that significantly affect their social and job performance and their independence, as well as their adherence to treatment 5; this increases the possibility of having depressive episodes 6,7. Moreover, the physiological effects of an infarct, such as angina pectoris, can potentially cause anxiety and fear in front of a coronary event 8. These events, together with depression, have a significant repercussion on the patient emotional state.
The social performance of patients is conditioned by the physical and emotional effects caused by the infarct, for the social activities with family, friends and the community are affected by the loss of independence to perform daily tasks and the role swap implied in this. Isolation and the reduction in the perception of health and quality of life entails a reduction on the patients’ dedication to their work and other social activities. This situation usually turns into a vicious cycle, for isolation increases stress, helplessness and the belief of being a burden to the family, all of which may pave the way for the development of another coronary event 9.
This is how the coronary disease becomes a chronic condition, which makes imperative the patient’s adherence to pharmacological and non-pharmacological treatment. Such adherence also includes following medical recommendations, attending scheduled appointments, avoiding potentially risky behavior, taking medication as indicated and properly fulfilling the assigned therapeutic regime 10.
Research shows adherence to treatment as having multiple causes, where the patients’ beliefs, the kind of disease, the type of pharmacological treatment, information and social support are not the only aspects that influence on it. Motivation plays a crucial role as well, for there is a close relationship between it and the importance that the individual gives to the monitoring of treatment and the actual possibility of undergoing it 11. According to Camacho and Del Campo 12, there are countless definitions of motivation, all pointing at an action that implies encouraging someone to meaningful learning. This will help explain human behavior, for motivational behavior goes by the stages of initiation, alerting and resolution. These stages make it easier for individuals to reach their goals, such as treatment adherence.
Motivational interviewing is conceived as a clinical communication method that can be used in professional nursing with the aim of encouraging patients to assume behavioral changes that will benefit their health 13. Here, nursing staff work as facilitators who help patients develop their own motivation for a change; hence, resistance is reduced, ambivalence is sorted out and self-confidence is increased (self-efficacy), so that they choose their own goals and the necessary actions to reach them (self-control). These are necessary features for patients who have suffered acute myocardial infarction to assume responsibility over their taking of prescribed medicine and recommended diet. Likewise, such features are crucial for patients to deal with risk factors for their condition, attend medical checkups and boost the increase of self-efficacy, all of which is undeniably related to adherence to treatment in disease management 14.
Boveda Fontan 15, states that motivational interviewing has been developed as a clinical method to promote patient behavior changes. Nonetheless, when referring to cardiovascular patients, Rivera Mercado 16 claims that at an international stage, this method has been studied in the control of risk factors only; it has proved effective in diet and physical activity and it could be useful in patient weight management, systolic blood pressure and cholesterol levels. On the other hand, Spoelstra 17 found motivational interviewing to be an effective strategy in pharmacological treatment adherence, however, at a national stage, no relevant data was found.
Having in mind what has been stated above, it is imperative that nursing professionals design, apply and evaluate the efficiency of various strategies meant to improve the understanding of established treatments. This will not only help improve the adherence to treatments, but it will also reduce in the medium and long term effects that coronary disease may have over patient performance. Therefore, the objective of this research has been to determine the effect of motivational interviewing, a nursing strategy, on adherence to treatment in patients who have suffered acute myocardial infarction and attend phase II in a cardiac rehabilitation program in Bogota.
METHODOLOGY
Research design
This study used a quasi-experimental design that applied nursing intervention through motivational interviewing, in order to improve adherence to treatment in patients who have suffered acute myocardial infarction and attend phase II in a cardiac rehabilitation program, which has been considered a key aspect in the management of patients in this condition.
Population and sample size
The target population was composed of subjects that had suffered acute myocardial infarction and attended phase II in a cardiac rehabilitation program. Available population for the study were those subjects who had suffered acute myocardial infarction and attended phase II in a cardiac rehabilitation program in Bogota in the first half of 2015. The size of the sample was calculated based on the instrument standard deviation (5.7), with a type I error of 0.05, corresponding to 44 patients, 22 for each study group.
Inclusion criteria
Patients (male and female) who had suffered acute myocardial infarction, under any treatment, and who attended phase II of the cardiac rehabilitation program in the selected institution. Patients with adequate cognitive capacity to participate in the motivational interviewing. Patients with access to telephone service, for the procedure of the used motivational interviewing included two sessions by telephone.
Intervention
The control group received the usual intervention from the cardiac rehabilitation program, which consisted of monitored physical exercise sessions and educational activities, suited to the personal needs of each patient, offered by the nursing staff. Beside this treatment, the experimental group received extra nursing intervention which consisted of one weekly motivational interview during three weeks: the first interview was carried out face to face, the last two interviews were carried out by telephone.
Each session began establishing the patient’s stage of change (or motivation) (precontemplation, contemplation, preparation, action and maintenance), then, the motivational interview followed a script previously designed for the study. This script links the process for adopting precautions, based on the Prochaska and DiClemente model, with the interview general guidelines, thus, including potential statements to use through the interview, considering the objectives of the stage of motivation in which each patient was.
Instrument for data collection
This research used a “questionnaire to measure adherence to treatment in patients with cardiovascular disease” as its data collection instrument. This questionnaire is composed of 29 items and produces a score between 29 and 174 points, where a higher score implies higher adherence to treatment. The instrument reports an adequate internal consistency with a Cronbach alpha of 0.837. The instrument provides six dimensions: expectations and self-efficacy behaviors, following the healthcare staff guidance regarding the taking of medicine and diet, need of support for treatment adherence, long term adherence expected behavior, management of tense situations and physical activity 18.
Proceedings
The study was developed through two stages:
The first one consisted on developing a pilot test that included 12 patients who had suffered acute myocardial infarction and attended phase II in a cardiac rehabilitation program in the institution selected for research. The aim of this pilot was to have a first take and feedback from the field in order to improve aspects of the intervention. These patients were not included in the final analysis of results.
The second stage was the carrying out of the research proposal. After having signed the informed consent, participants were assigned to a group (ether control or intervention) and then were given the instrument to measure their level of adherence. Control group patients received the usual treatment from the cardiac rehabilitation program, whereas experimental group patients, beside this treatment, received the extra nursing intervention. Finally, both groups were given twice again the instrument to measure their level of adherence, one week and five weeks after the intervention had finished.
Data processing and analysis
Data was tabulated in a spreadsheet and processed using SPSS (version 22, licensed for the National University of Colombia). Along with descriptive tools, the quantitative evaluation of the nursing strategy was performed using the Mann-Whitney nonparametric U test to analyze results between control and experimental groups. Wilcoxon test and Student's t-test were used to evaluate directionality in changes on adherence to treatment in intragroup analysis.
Ethical considerations
To be included in the study, patients had to be over 18 years of age, show mental capacity to answer the questionnaire and willingly accept their participation in the study. This responds to what is established in the 1993 008430 Resolution of the Health Ministry of the Republic of Colombia and agrees with the ethical guidelines from the Council for International Organizations of Medical Sciences and the World Health Organization (WHO). Furthermore, the study has been endorsed by the ethical and research committees from the National University of Colombia (as stated in the University’s minute number 6, dated April 14, 2014) and from the institution where the research was carried out (as stated in the institution’s minute number 7, from April 2014).
RESULTS
Socio demographic variables show the following:
Table 1. Participants’ socio demographic variables
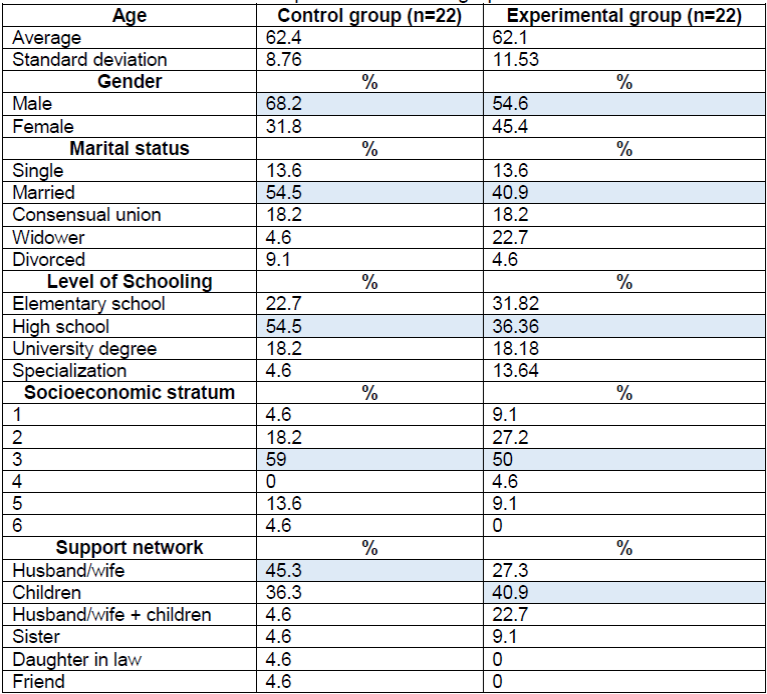
Source: Elaborated by the author based on the results of the study
Results from the socio demographic variables show that the average age for both study groups was 62, that most participants were married, most participants had finished high school, belong to socioeconomic stratum 3, and had their nuclear family as a support network.
The following Table presents a comparative analysis of control and experimental group regarding adherence to treatment.
Table 2. Inter-group analysis for adherence to treatment.

Source: Elaborated by the author based on the results of the study
Comparative analysis between control and experimental groups considered the interpretation of results for global adherence in each measurement. In order to do this, the nonparametric Mann-Whitney U test was used, which compare the average information from each group ,19. The analysis found no statistically relevant difference when comparing control and experimental groups.
On the other hand, data processing considered intra-group analysis, where global adherence data was compared, considering the six dimensions included in the applied instrument using the Wilcoxon test, as it is shown in Table 3.
Table 3. Wilcoxon test results for the comparison of total score and every dimension in each measurement.
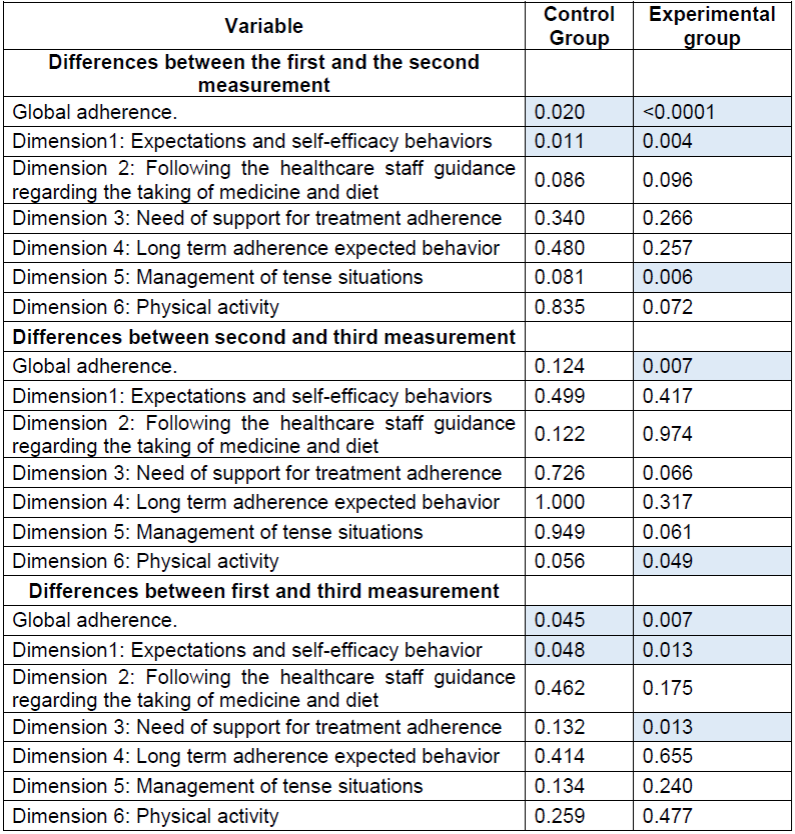
Source: Elaborated by the author based on the results of the study
The intra-group analysis for control group shows a statistically significant change in global adherence and in dimension 1 (expectations and self-efficacy behavior), when comparing the first and second measurement, as well as in the comparison between the first and third measurement.
Regarding the experimental group, statistically significant changes were found in global adherence and dimensions 1 and 5 (expectations and self-efficacy behavior, and management of tense situations, respectively) in the differences between the first and the second measurement. Besides, when looking at the differences between the second and the third measurement, statistically significant changes were found in global adherence and dimension 6 (physical activity). Finally, differences between the first and the third measurement show statistically significant changes in global adherence and dimensions 1 and 3 (expectations and self-efficacy behavior, and need of support for treatment adherence, respectively).
The Kolmogorov-Smirnov test was applied to verify the fitness to normality of the variables studied, and finally, the Student's t-test was used to value directionality in global adherence variation and confidence intervals for the average increase, as it can be seen in Table 4.
Table 4. Student’s t-test results for the evaluation of directionality in global adherence at the different stages of measurement.
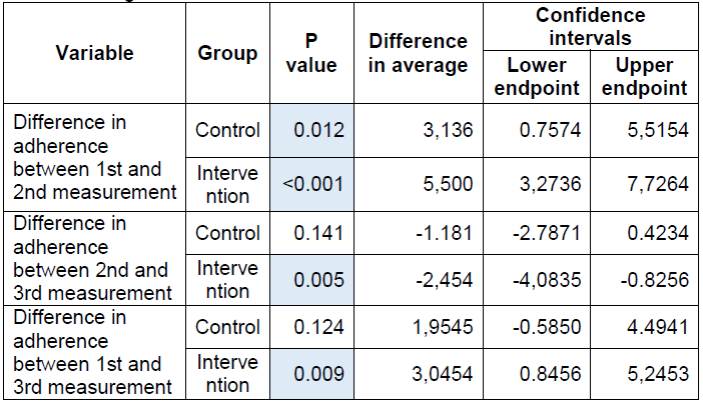
Source: Elaborated by the author based on the results of the study
Student’s t-test shows statistically significant changes in all stages of measurement for the experimental group, with a p<0.05, whereas in the control group, changes were meaningful only in the difference between the first and the second measurement. However, confidence interval analysis shows that such changes were positive in all stages but the second (difference in adherence between the 2nd and the 3rd measurements); such result could be expected given the normal behavior of adherence, which tends to diminish in time as the stimuli from the intervention stops.
DISCUSSION
In terms of socio demographic variables, the findings in this study are similar to findings reported by national statistics, where ischemic disease is considered common in adults between ages 45 and 55. Similarly, in their study, Chavarriaga et al 20 found an average age of 62 and the prevailing of coronary disease in adult males between ages 41 and 80. Vela and Barrón López 21 found that a partner plays an important role in keeping long term heart-healthy habits; this shows that the active involvement of nuclear families is a protecting factor that significantly favors treatment adherence, which is consistent with our results. Regarding level of schooling, some authors consider this variable to be influential in long-term mortality rates after an acute myocardial infarction, as well as in adherence to treatment, for it influences the understanding, appropriation and fulfilment of recommended activities as part of the disease treatment 22. Hence, having high school as the average level of schooling in this research may have influenced the results after the nursing intervention.
Intergroup analysis did not show results to be consistent with what is found in specialized literature, where motivational interviewing has proved to be effective in generating the necessary behavior changes to the management of diverse health conditions; such as in the case of patients with cardiovascular risk factors 23 and chronic diseases 24. This analysis was not consistent with the reports in Pietrabissa et al either; in their research, these authors applied three motivational interviewing sessions to a patient in cardiac rehabilitation and found, at the end of the intervention, a greater sense of control over the patient’s own health, as well as an increase in self-efficacy. This led the patient to assume full responsibility in his own process, change behavior and reach long term results 25.
Nevertheless, this inconsistency in the results can be explained by the length of the intervention performed, since a recent meta-analysis published by Easthall et al 26 has shown that cognitive behavioral techniques, such as motivational interviewing, are more efficient interventions in the increase of adherence than most of the educational interventions used in current practices. Such changes, though, are statistically significant only in studies where interventions lasted between 3 and 12 months. Similarly, Rubak et al 27 found in their meta-analysis that the average time of research follow-up periods is 12 months with a minimum of 2 months and a maximum of 4 years, which supports our argument that longer follow-up periods lead to an increase in the percentage of intervention effectivity.
Although the intervention applied in this research did not cause statistically significant changes in the inter-group analysis, the increase of adherence as a result of behavior changes in patients suffering from coronary disease deserves a special mention, for it has effects at short and long term in reducing morbidity and mortality, improving patients’ quality of life and helping them go back to their everyday life activities. On this aspect, it is also worth referring to the well-known discussion on the P value 28, which, although it shows the probability of proving study hypothesis, can vary depending on the sample size and the significance of the change that a study may want to identify ,29. Thus, it is necessary to consider the effect of interventions from the perspective of their clinical significance and the impact on patients’ lives.
Moreover, it is important to highlight that after the inter-group analysis of the dimensions of adherence, a statistically significant difference was spotted in the management of tense situations 5 weeks after the motivational interviewing nursing intervention had happened. A pilot study carried out by Fried 30 has shown that motivational interviewing reduces stress levels perceived by a group of students; this author refers to other studies that show the use of motivational strategies to be useful in helping reduce stress in long terms, which is consistent with the findings of this study. Furthermore, it also needs to be considered the fact that patients lack knowledge about the importance of stress management as part of the treatment for cardiovascular diseases, which leads to poor or no stress management techniques. Thus, approaching this subject through motivational interviewing may also be related to the results obtained in this particular dimension.
On the other hand, intra-group analysis showed the efficiency of cardiac rehabilitation programs in terms of global adherence as well as in terms of expectations and self-efficacy behavior, since changes statistically significant were found at the different stages of measurement in control group. However, nursing intervention based on motivational interviewing could produce significant changes in global adherence at all stages and in most of the dimensions considered, which places motivational interviewing as a promising strategy for reaching a better adherence to treatment in patients who have suffered acute myocardial infarction.
Study limitations
There are two factors that could have influenced the results in this research: the patients’ high degree of adherence at the moment of starting the study, on the one hand, and, on the other, the size of the sample in each group, which could have limited the identification of modifications in terms of adherence to treatment.
Recommendations for further studies
Further research is advised to widen the size of the sample and to carry out comparisons of the number of interventions to determine the ideal number of sessions for motivational interviewing in order to improve patient adherence to treatment. This way, interventions, which have to be used through the nursing educational and care processes in order to ensure better adherence to treatment of patients who have suffered acute myocardial infarction, can be standardized.
CONCLUSIONS
Baseline measurements of adherence to treatment in both control and experimental groups showed values for high adherence. This can be related to perceptions towards the severity of acute myocardial infarction, since, the perception of a poorer state of health is related to major adherence to the treatment for the disease.
Inter-group analysis showed that there are statistically significant differences (p= 0.013) only in the third measurement of the dimension that refers to the management of tense situations. However, intra-group analysis showed a statistically significant difference in all three stages in global adherence as well as in the amount of dimensions of the experimental group as compared to the control group, which is also clinically relevant, due to the benefits that this implies.
Motivational interviewing is a strategy that looks for behavioral changes based on the increase of self-efficacy and self-control. This is efficient in the management of patients suffering chronic diseases, thus nursing professionals ought to guide their therapeutic relationship with the aim of optimizing results regarding patient decision making and empowerment facing the management of his health condition.
Based on the fact that adherence to treatment has multiple causes, motivational interviewing can be used to complete and reinforce all activities previously established for any cardiac rehabilitation program. Adherence to treatment then requires restructuring and implementation of diverse interventions aimed at managing the different factors that influence it. The only goal being the improvement of the quality of life of patients who have suffered acute myocardium infarct, and so helping them in their going back to their everyday life activities, as well as in the reduction of complications derived from the patients’ health condition. Nevertheless, more research in the field is needed.
REFERENCIAS
1. Global Health Data Exchange. Institute for Health Metrics and Evaluation. University of Washington. 2016. Estados Unidos de America [Internet] [Citado 19 de Julio de 2018]. Recuperado a partir de: https://vizhub.healthdata.org/gbd-compare/ [ Links ]
2. Mozaffarian D, Benjamin E, Go A, Arnett D, Blaha M, Cushman M, et al. Heart Disease and Stroke Statistics - 2016. Update. A report from de American Heart Association. Circulation. 2016;133(8):000-000. [ Links ]
3. Departamento Administrativo Nacional de Estadística. Defunciones no fetales 2015, preliminar. Colombia; [Internet] [Citado 5 de julio de 2017]. Recuperado a partir de: http://www.dane.gov.co/index.php/esp/component/content/article/118-demograficas/estadisticas-vitales/6234-defunciones-no-fetales-2015-preliminar [ Links ]
4. Rios Oropesa D, Cervera Estrada L, Hernández Riera R. Reincorporación laboral en pacientes con antecedente de infarto del miocardio. AMC. 2013; 17(4): 419-434. [ Links ]
5. Núñez LY, Vargas González D, Núñez Quintero M. Psicoterapia breve con pacientes infartados en fase extra hospitalaria. Revista Electrónica Dr. Zoilo E. Marínelo Vidaurreta [revista en internet]. 2013 [citado 15 abril 2018];38 (IV). [ Links ]
6. Esquivel Zúñiga MR, Garzona Navas AF, Sauma Webb AJ. Depresión post infarto agudo del miocardio: implicaciones en el manejo y la mortalidad. Revista cúpula. 2015; 29(12): 23-31. [ Links ]
7. Mendoza Franco RA. Prevalencia de la depresión posterior a un episodio de infarto agudo al miocardio en Cartagena. [Tesis en internet]. [Colombia]: Universidad de Cartagena; 2012. [Citado julio de 2017]. Recuperado a partir de: http://190.242.62.234:8080/jspui/handle/11227/1949 [ Links ]
8. Rodríguez Rodríguez CT. Factores emocionales en la prevención, diagnóstico y tratamiento de las enfermedades cardiovasculares. Valoración actualizada desde la psicocardiología. Rev Finlay. 2012;2(3):158-168. [ Links ]
9. Vargas Toloza R, Ordoñez Pabón E, Montalvo miranda O, Díaz Torres V. Calidad de vida relacionada con la salud de los pacientes postinfarto agudo de miocardio. Revista ciencia y cuidado. 2008;5 (1): 40-50. [ Links ]
10. Ramos Morales LE. La adherencia al tratamiento en las enfermedades crónicas. Rev Cubana Angiol Cir Vasc. 2015; 16(2): 175-189. [ Links ]
11. Martin Alfonso LA, Grau Abalo JA, Espinosa Brito AD. Marco conceptual para la evaluación y mejora de la adherencia a los tratamientos médicos en enfermedades crónicas. Rev Cubana Salud Pública. 2014; 40(2): 225-238. [ Links ]
12. Camacho-Miñano M, Del Campo C. Impacto de la motivación intrínseca en el rendimiento académico a través de trabajos voluntarios: un análisis empírico. Revista Complutense de Educación. 2015; 26(1): 67-80. [ Links ]
13. Droppa M, Lee H. Entrevista motivacional: un camino para mejorar la salud. Nursing. 2014; 31(6): 24-29. [ Links ]
14. Sánchez Monfort J. Entrevista motivacional para enfermería y otras profesiones sanitarias. 2017. España [Internet] [Citado 19 de Julio de 2018]. Recuperado a partir de: http://imc-diabetes.es/wp-content/uploads/2017/01/Entrevista-motivacional-para-enfermeri%CC%81a.pdf [ Links ]
15. Bóveda Fontán J, Perula de Torres LA, Campiñez Navarro M, Bosh Fontcuberta J, Barragán Brun N, Prados Castillejo JA. Evidencia actual de la entrevista motivacional en el abordaje de los probelmas de salud en atención primaria. Aten primaria. 2013; 45(9): 486-495. [ Links ]
16. Rivera Mercado S, Villouta Cassinelli MF, Ilabaca Grez A. Entrevista motivacional: ¿Cuál es su efectividad en problemas prevalentes de atención primaria?. Aten primaria. 2008; 40(5): 257-261. [ Links ]
17. Spoelstra SL, Schueller M, Hilton M, Ridenour K. Interventions combining motivational interviewing and cognitive behavior to promote medication adherence: a literature review. J Clin Nurs. 2015: 24(9-10): 1163-73. [ Links ]
18. Achury- Beltrán LF. Validez y confiabilidad del cuestionario para medir la adherencia al tratamiento de pacientes con enfermedad cardiovascular. Aquichan. 2017; 17(4): 460-471. [ Links ]
19. Rivas-Ruiz R, Moreno-Palacios J, Talavera J. Diferencias de medianas con U de Mann-Whitney. Rev Med Inst Mex Seguro Soc. 2013; 51(4): 414-9. [ Links ]
20. Chavarriaga J, Beltrán J, Senior J, Fernández A, Rodríguez A, Toro J. Características epidemiológicas, clínicas, tratamiento y pronóstico de los pacientes con diagnóstico de síndrome coronario agudo en unidad especializada. Acta médica colombiana. 2014; 39(1): 21-28. [ Links ]
21. Varela Montero I, Barrón López A. La influencia de la pareja en el ajuste a la enfermedad cardiaca. Acta de Investigación psicológica. 2016; 6(2): 2459-2468. [ Links ]
22. Consuegra-Sanchez L, Melarejo-Moreno A, Galcera-Tomás J, Alonso-Fernández N, Díaz-Pastor Á, Escudero-Garcia G, et al. Educational level and long term mortality in patients with acute myocardial infarction. Rev Esp Cardiol. 2015; 68(11): 935-942. [ Links ]
23. Hardcastle S, Taylor A, Bailey M, Harley R, Hagger M. Effectiveness of a motivational interviewing intervention on weight loss, physical activity and cardiovascular disease risk factors: a randomised controlled trial with a 12 month post intervention follow-up. Int J Behav Nutr Phys Act. 2013; 10(40): 2-16. [ Links ]
24. Castilla Nieto R. Entrevista motivacional en el tratamiento de personas con enfermedades crónicas. Rev Esp común Salud. 2016; 7(1): 113-123. [ Links ]
25. Pietrabissa G, Ceccarini M, Borrello M, Manzoni GM, Titon A, Nibbio F, et al. Enhancing behavioral change with motivational interviewing: a case study in a Cardiac Rehabilitation Unit. Front Psychol. 2015; 6: 1-9. [ Links ]
26. Easthall C, Song F, Bhattacharya D. A meta-analysis of cognitive-based behavior change techniques as interventions to improve medication adherence. BMJ open. 2013; 3 (8): 1-17. [ Links ]
27. Rubak S, Sandbaek A, Lauritzen T, Christensen B. Motivational interviewing: a systematic review and meta-analysis. Br J Gen Pract. 2005; 55(513): 305-312. [ Links ]
28. Cohen J. The earth is round (p < .05). American psychologist. 1994; 49(12): 997-1003. [ Links ]
29. Manterola C, Pineda V. El valor de la "p" y la "significación estadística" aspectos generales y su valor en la práctica clínica. Rev Chil Cir. 2008; 60(1): 86-89. [ Links ]
30. Fied R. Calmly coping: a motivational interviewing via co-Active life coaching (MI-via_CALC) interventions for university students suffering from stress. [Tesis en internet]. [Canadá]: University of Western Ontario; 2014. [Citado noviembre de 2017]. Recuperado a partir de: https://ir.lib.uwo.ca/cgi/viewcontent.cgi?referer=&httpsredir=1&article=3772&context=etd [ Links ]
Received: September 13, 2018; Accepted: November 05, 2018
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
