










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.19 no.57 Murcia ene. 2020 Epub 16-Mar-2020
https://dx.doi.org/eglobal.19.1.361801
Originals
Effect of an expert patient program in heart failure
1Pontificia Universidad Javeriana. Associate Professor of the Faculty of Nursing and coordinator of the GESCCA Seedbed: Cardiovascular Care Managers. Bogotá. Colombia. dachury@javeriana.edu.co
2 Pontificia Universidad Javeriana. Faculty of Nursing, GESCCA Seedbed: Cardiovascular Care Managers Bogotá. Colombia.
Introduction
One of the strategies that has shown improvement in self-care for patients with heart failure is the formation of dyads and groups to provide peer support and achieve individual goals.
General objective
To determine the effect of an expert patient program on heart failure related to the knowledge about adherence to treatment and satisfaction.
Method
A sectional-descriptive pilot study was conducted in patients with heart failure diagnoses in a fourth-level institution. The sample size represents the entire population with the restriction criteria (N: 20 subjects). An expert patient program was implemented for 6 months and the measured outcomes were level of knowledge and satisfaction. Data was gathered from a knowledge test on adherence to treatment and a satisfaction poll. Information was processed with IBM SPSS Statistics 23.0. The distribution of absolute and relative frequencies was performed by descriptive analysis.
Results
More than 95% of patients showed improvement in the level of knowledge and 85% reported a high global level of satisfaction (very satisfied), reflected in the dimension of loyalty and effectiveness.
Conclusions
The expert patient in heart failure program is a cost-effective intervention, which provides capabilities to help other patients gain self-confidence and skills to manage their health condition.
Keywords: Expert patient; Self-control
INTRODUCTION
In current time, heart failure (HF) is considered one of the main non transmitTable diseases that generate a great impact in population. It’s estimated that the rising in its incidence is related to the aging and increase of the vascular risk factors. Worldwide, it affects 26 million people. Likewise, it represents the third cause of death in developed countries1.
In Colombia, the 2.3% of population presents HF and in 2013 an increase of 40,8% was reported of hospitalary re-entries caused by decompensations2, which generates elevated costs for the health system and compromises the quality of life of patients and their families3. Therefore, it’s necessary to develop strategies suited to mitigate this problematic, oriented to promote the participation of the patient in the care and decision making process, in order to accomplish the proper level of self care and adherence to the pharmaceutical and non-pharmaceutical treatments4.
The world health organization (WHO), points out in the new chronic care model that the capacity of making decisions regarding their health status, needs to be developed in patients and create conductual changes in their lifestyle to promote self-care. With this purpose, the health professional should integrate different strategies to the traditional care, led by patients5.
One strategy that has shown to be effective is the formation of expert patients, in which people who have a chronic disease get orientation and are formed to create abilities in regards to handling their condition, abilities that allow them to even help other patients acquire self-trust. To establish a connection between two or more people that have similar characteristics, as the presence of a disease, it’s seeks to favor the achievement of individual and group goals. Patients acquire an active and leading roll and the health professionals a passive or observant rol, it’s a companionship that can act as re- conduct if necessary6.
One of the initiatives that responds to this strategy is the called Chronic Disease Self-Management Program. This project is born in 1990 at Stanford University with the purpose of transmitting knowledge and abilities related to the specific care of the disease to increase the self-care. The university has programs directed to patients with arthritis, diabetes, people with HIV, chronic pain and a workshop in which diverse chronicle diseases are talked about7. Progressively, the methodology impulsed the extension of the program worldwide: United Kingdom, patients university, Joseph Laporte foundation, Barcelona, Andalucía, Catalunya, among others, which pretend to improve the comprehension and awareness of chronic disease by the citizens. By implementing this on patients with heart failure and evaluating their level of satisfaction, it’s highlighted a satisfaction result above 4.6 out of 5, which is reflected as an adaptation of an auto responsible roll by the participant patients and, at once, can be effective both clinically and economically8.
The implementation of this program should be framed in its effectiveness. Authors such as González 9, Griffiths 10 and Holden 11 recommend evaluating their impact through the level of knowledge and satisfaction, as determinants to generate autonomy, co-responsibility and empowerment of the patient. Likewise, they point out that its implementation will allow changing the paradigm of the biomedical model that frames care, which will result in a better complement to the work of education carried out by health professionals.
In Colombia, there is only one expert patient program led by the Santa Fe de Bogotá Foundation, which offers educational strategies to patients with chronic diseases and their families, allowing them to assume commitments to health care and prevention of diseases. However, this program is not specific to the population of patients with HF.
In the country there are still few such programs that, although they are included in the technical guide Good practices for patient safety in health care of the Ministry of Social Protection of the Republic of Colombia 12 and aim to strengthen self-care of patients, have not reached the impact and relevance they require. This is due to the fact that a predominantly paternalistic health system continues to be managed, and doctors and nurses are still the ones who exclusively manage the information; they are in charge of patient education and leave aside the possibility of using the modality of "expert patient program" as a tool to educate and improve the current morbidity and mortality Figures by HF.
Likewise, reluctance on the part of health professionals to identify these types of programs is identified, when they perceive that they can lose their leading role in education 13. Due to the above, there is evidence of a knowledge gap and the need to involve the new profile of the expert patient with heart failure in health institutions, in addition to assessing its effect in the short and long term. The scope of this investigation was short-term evaluation.
OBJECTIVE
To determine the effect of a patient's expert program on heart failure on the knowledge related to adherence to treatment and satisfaction
METHOD
Design, population and sample size
A cross-sectional descriptive pilot study was carried out in patients with CF diagnoses who attended an outpatient clinic in a fourth level institution. The inclusion criteria were: male or female patients older than 18 years, with a diagnosis of heart failure that are linked to a heart failure program. The sample size corresponded to the entire population with the restriction criteria (N: 20 subjects), through a non-probabilistic sampling. Patients with functional class IV and who were in palliation treatment and could not participate in the program were excluded from the study.
Intervention
The intervention consisted of the design and application of the expert patient program. The first stage was to select the patients who would lead the program and train their peers. Patients selected as experts should have characteristics such as: adequate communication skills and adequate adherence to treatment. The training of these leading patients was carried out during 4 sessions, with a periodicity of once a week and a duration of 2 hours each. The content of the educational sessions in the patient training process was oriented to teaching methodologies in adults, and the management of pharmacological and non-pharmacological treatment based on the experience lived. Once the sessions were finished, the expert patient was evaluated from a role play. The second stage was oriented to the process of peer formation by the experts. For this purpose, a screening of patients who wanted to participate was carried out, a group of 20 patients was formed, and the expert made 6 educational sessions during 6 months with a monthly periodicity. The methodology used in the educational sessions was reflexive, based on guiding questions about the experience lived in the change of behaviors versus pharmacological and non-pharmacological treatment. The active role during the program was that of the expert patient and the nursing professionals played a passive role as observers; they only intervened if necessary. At the end of the last session, the knowledge test and the satisfaction survey were applied.
Main outcome
The level of satisfaction and changes in knowledge related to adherence to pharmacological and non-pharmacological treatment.
Instrument
A knowledge test of 10 questions with a multiple-choice response scale was designed to assess the aspects of adherence to non-pharmacological treatment contemplated in the European Guide on the diagnosis and treatment of acute and chronic heart failure 14, such as diet, weight control, physical activity, warning signs and taking medications and liquids. In order to assess satisfaction, a survey was conducted with 13 questions, based on Hall and Dornan referents 15, designed to measure three dimensions: program quality, technical competence and loyalty. It has a Likert scale with five response options, where one is the lowest value (very dissatisfied) and five the highest (very satisfied). The knowledge test was applied before and at the end of the expert patient program, and the satisfaction survey at the end. A pilot test was carried out with 5 patients and a review by 2 professional experts with the purpose of examining the clarity and understanding of the survey and the test.
Process
Analysis plan
The information was processed through the IBM SPSS Statistics 23.0 program of 2014. A descriptive analysis was performed with distribution of absolute and relative frequencies.
Ethical aspects
The study met the standards of scientific, technical and administrative standards for health research, Resolution 008430 of 1993 of the Ministry of Health of the Republic of Colombia. It was considered a minimum risk study and, additionally, the ethical principles related to respect and autonomy, beneficence - non maleficence, justice and confidentiality were taken into account. The study adhered to national or international ethical standards for the protection of the rights of research participants. Finally, voluntary participation, confidentiality of information and informed consent on the part of study participants are included.
Outcomes
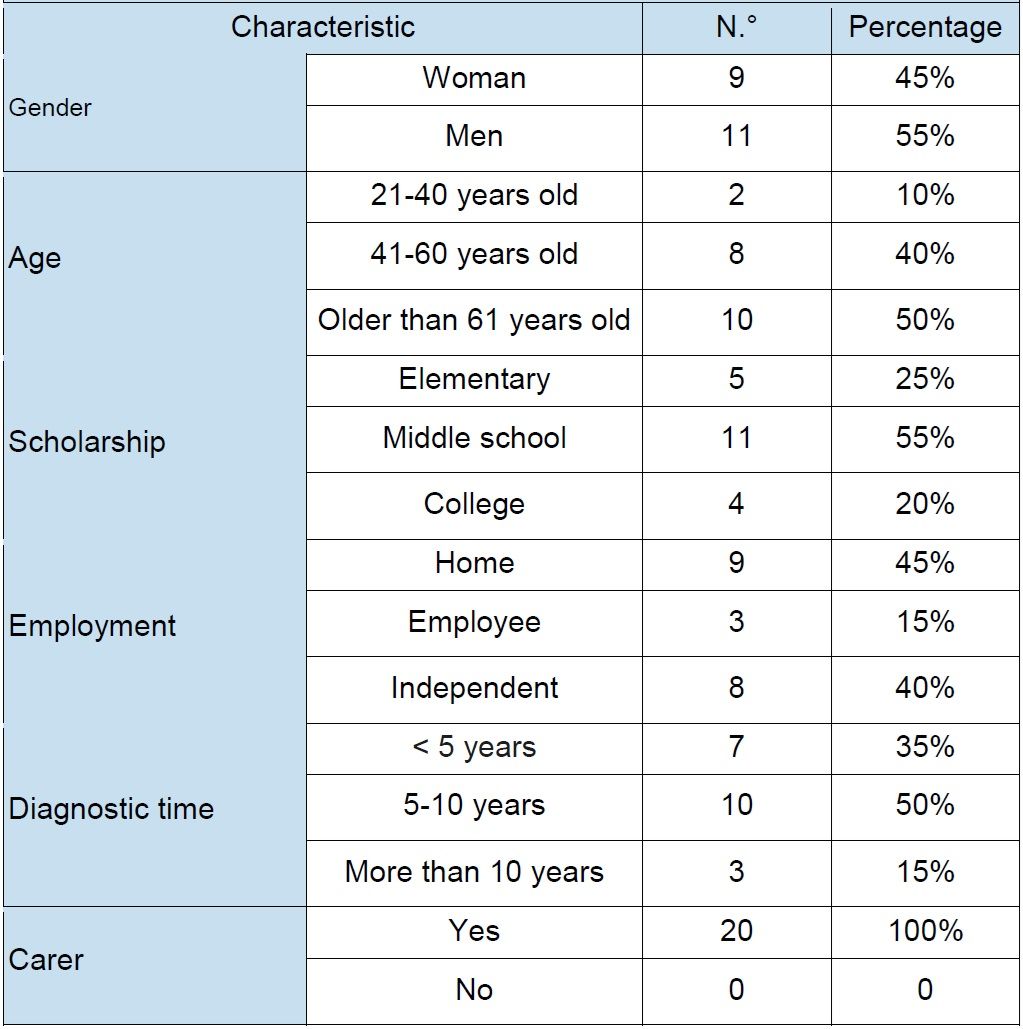
It is observed that the majority of patients were women with an average age between 41-61 years, with a high school education, whose occupation was home, followed by an independent one, with a diagnostic time of 5 to 10 years. All have a caregiver (Table 1).
Before the expert patient program, it was found that most of the participants did not know clearly and precisely the recommendations related to the medications (70%), diet (60%), warning signs (65%) and fluid control (60%). At the end of the 6 sessions on a monthly basis, there was a significant improvement in knowledge (95-100%) (Table 2).
Table 2. Results of the knowledge test before and after the application of the expert patient program
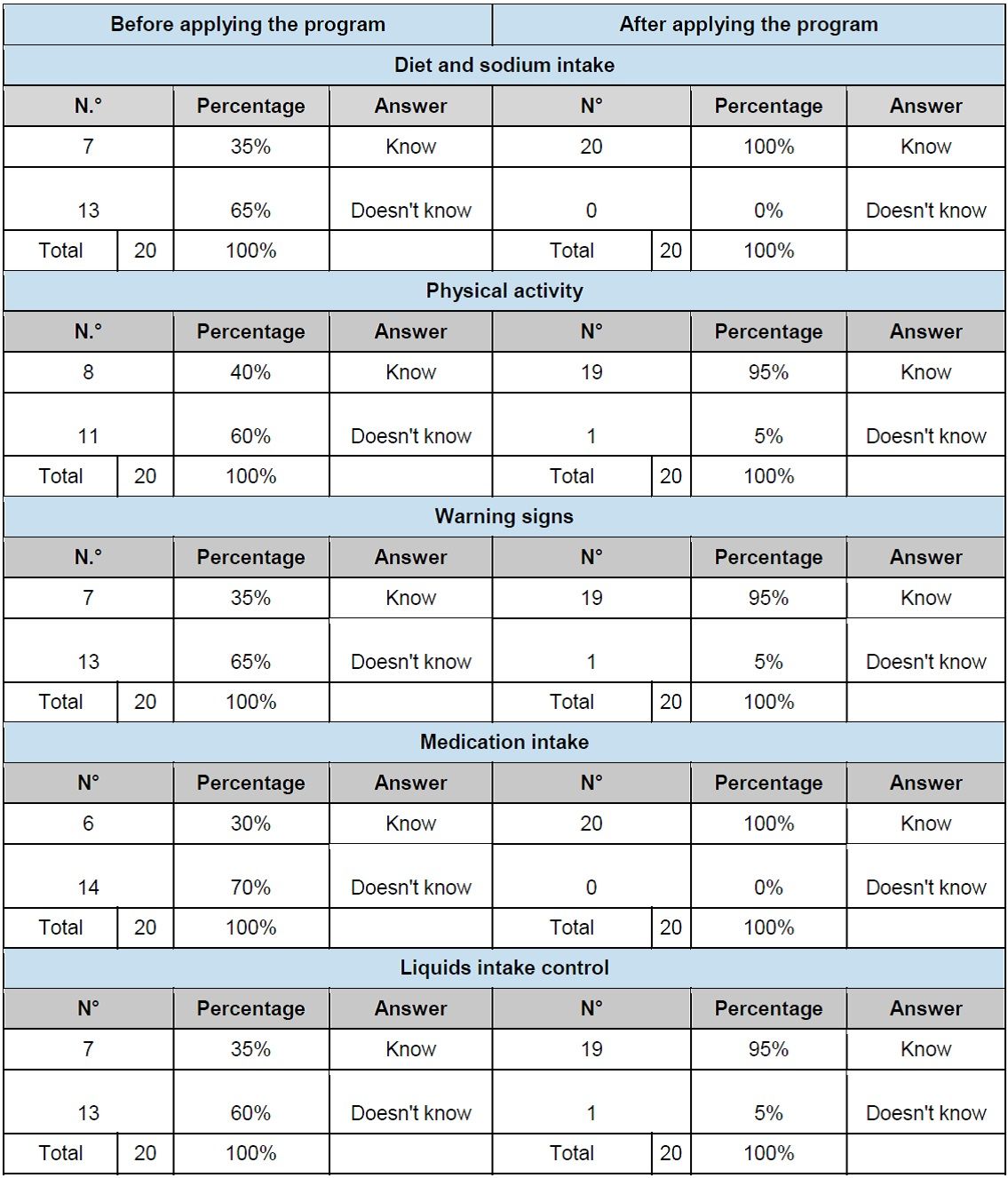
Source: study outcomes
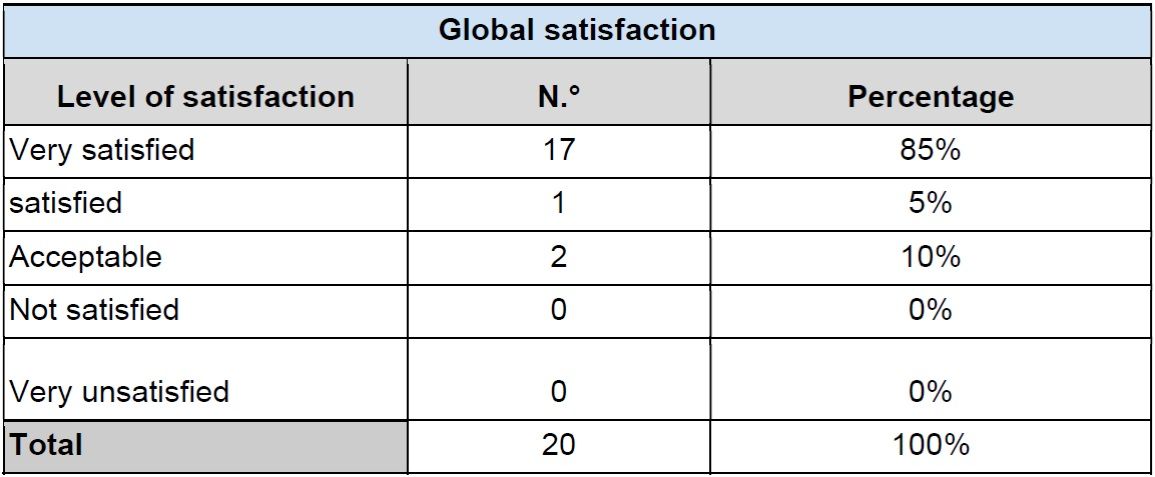
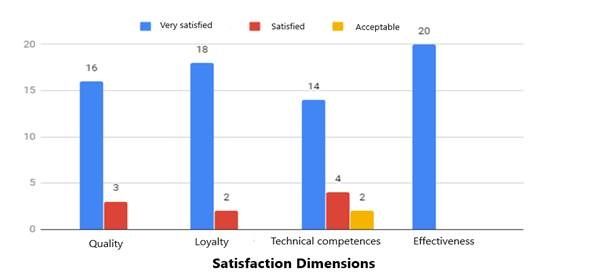
The overall satisfaction rating shows that most of the participating patients were very satisfied with what they had learned and achieved in the program (Table 3, Figure 1).

In the dimension of quality of the program, referring to the type and precision of the information, the clarity in its questions and the methodology used, it was found that 80% of the participants were very satisfied. Regarding the technical competences, understood as the ability of the expert patients in the teaching-learning process, it was evidenced that the participants were very satisfied in their greater percentage (70%). In the loyalty dimension, which refers to the expectations and recommendation of the program, 90% of patients were very satisfied. Finally, in the effectiveness dimension, which refers to the impact of the program reflected in the significant changes that they have had in their lifestyles and in their self-care from those learned and lived in the sessions, 100% of the participants were very satisfied (Table 4, Figure 2).
Table 4. Description of satisfaction dimensions on the expert patient program
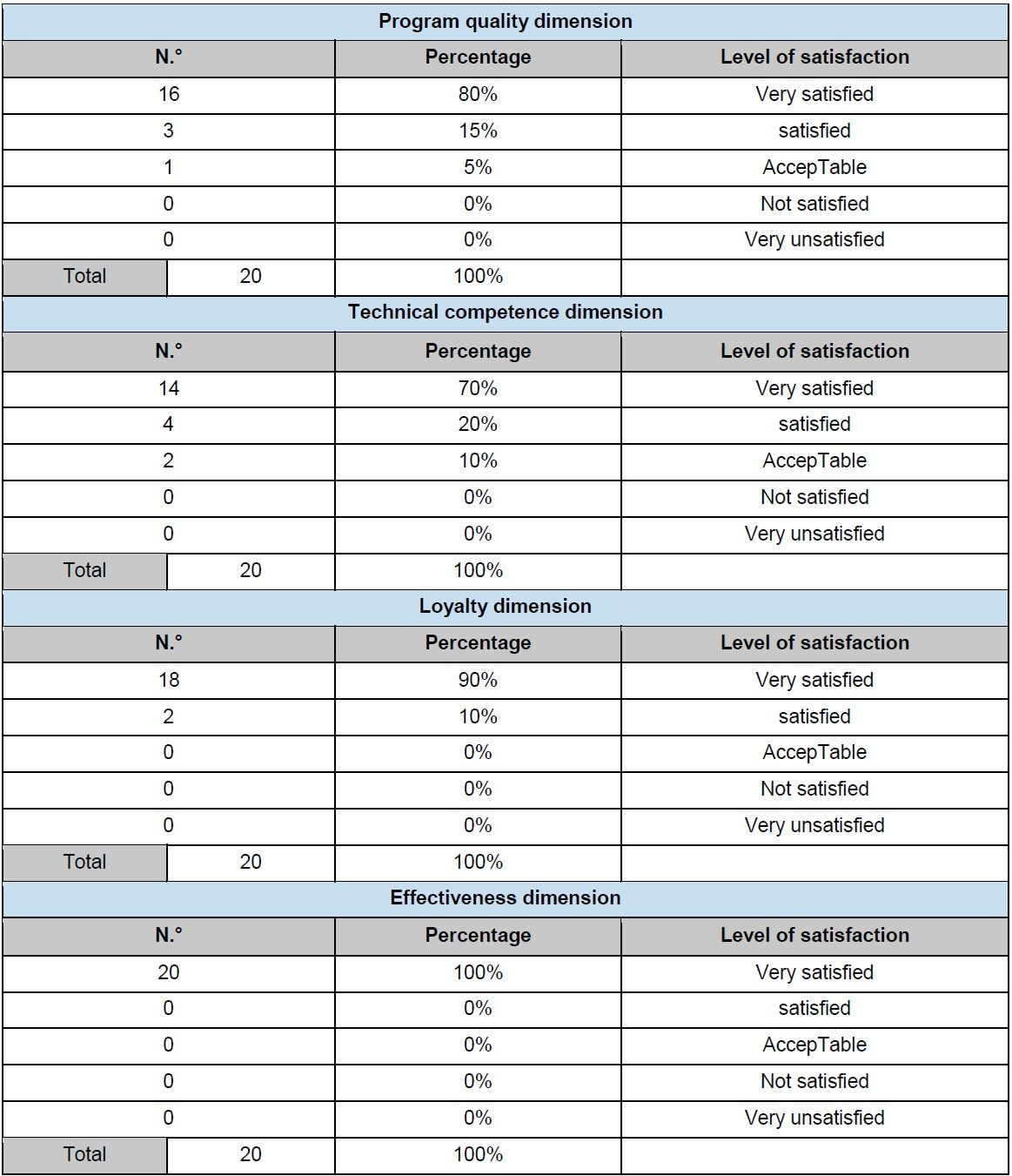
Source: study outcomes
DISCUSSION
The results show that the effect of the expert patient program generated a very important change in the degree of knowledge and level of satisfaction. Regarding the degree of knowledge, it was evident that most patients at the end of the sessions of the program significantly improved their knowledge related to pharmacological and non-pharmacological treatment, such as medications and diet, followed by the recognition of warning signs, physical activity and fluid control. The global guidelines for diagnosis and management of HF suggest that the patient should receive education to increase the level of knowledge about the proper management of their treatment, with the purpose of generating long-term changes that allow them to have a good control of their disease and avoid possible decompensation 16.
Authors such as Salvadó-Hernández 17 point out that there is a challenge in the search for strategies that increase adherence to non-pharmacological treatment from the health services, since numerous studies have shown that medications alone are not sufficient for the control of the disease or its complications. For this reason, it is necessary to promote education, not only with individual but group approach, where patients can have a leading role and can form other pairs from the example and strategies for changing their behaviors in self-care.
Barrios 18 points out that knowledge is a set of information stored through experience or learning (a posteriori) or through introspection (a priori). There are many ways to transmit that knowledge; one of the most used methods is the explicit one, in which the information is transmitted to the subjects through a formal communication. This process can be provided both by health personnel and expert patients, who have had a theoretical and experiential journey, therefore, have the necessary bases and livelihoods to educate or transmit their information to apprentice patients. They will be more open to adhere to the knowledge that comes from someone with whom they feel identified.
It is also important to emphasize that the nursing professional plays a fundamental role in this process, since he is in charge of complementing and supporting the expert patient in case it is necessary. Both parties generate an important complement: on the one hand, the patient expert contributes his experiences and tips (tips) for the day to day. On the other hand, the professional contributes technical and specific knowledge that are essential to achieve the empowerment of patients. The described can be confirmed with authors such as Molina et al. 19, who affirm that the information that is transmitted by an expert patient reaches the peer patient more directly, since it is performed from a similar level to their own, with a similar experience and using their same language. This, in turn, helps to avoid the defeatist attitude of some patients in front of health personnel and to raise doubts, difficulties and concerns that patients have regarding their illness.
The positive results achieved in the level of knowledge in this study coincide with the research of González A 20, where improvements in the self-care of the patients that were part of the expert patient program were evidenced, this thanks to the experiences that the Expert patients shared with apprentice patients. This promoted positive changes in the habits and lifestyles of patients, through actions that allowed them to recognize, treat and manage their health problems autonomously.
On the other hand, some sociodemographic variables characterized in this study, such as "being a woman" and a "medium-high level of schooling", could favor the improvement in knowledge. When reviewing the literature, Barreiro 21 showed that the highest degree of ignorance about chronic disease was associated with a low level of studies. It could also be affirmed that the fact of being a woman gives patients the skills to learn a little faster, because their thinking is typified in a network and the information under this scheme is permanently totalized.
Regarding the overall level of satisfaction, it was found that the participating patients were mostly very satisfied with the program, which reveals the fulfillment of the main objectives set. The participants were given an opportunity to become empowered of all the knowledge corresponding to heart failure, not only at a theoretical but practical level, including emotional aspects, in order to improve their quality of life in the medium and long term. A high level of satisfaction is influenced, because patients feel identified with other individuals who have lived the disease and are able to guide others in self-care and self-regulation of their health. In this way, the care offered by professionals, based on evidence, is combined with those of experience and experience.
Pesquera and López-López 22 state in their article what was stated by Prieto M, director of the first school of patients in Spain: this type of project, in addition to improving the quality of life of patients, decreases the number of visits to patients. doctor. In addition, he points out that the initiative is based on the concept that when the disease is well known, and when patients receive information among peers, diseases progress more slowly, side effects diminish and satisfaction increases. Therefore, the dependency of the health system is lower and the therapeutic adherence is greater, results comparable to those obtained in the present study.
For its part, the study carried out by Torres-Gonzáles and León-Manco 23 documents that the level of satisfaction is a very important concept:
"[...] for the subjectivity that accompanies it, since it is focused more towards the perceptions and attitudes of the person who made concrete and objective criteria. It also allows evaluating the perspective that patients have of the services that are provided to them and can serve as a predictor of the quality of care that is being offered to them."
Santana et al. 24 recommend listening to patients about the care delivered, since it is an opportunity to construct an outcome indicator that guides managers on the possible decision-making paths of transformations and innovations.
Satisfaction is a multidimensional concept in which different aspects related to the attention delivered are evaluated individually. The dimensions better qualified by the participants of the present study were effectiveness and loyalty. According to Gómez-Ramírez et al. 25, the perception of satisfaction is definitive to recognize the quality of a service. Therefore, as confirmed by Ampuero 26, it can be affirmed that there is a significant relationship between the quality of the service and the loyalty and effectiveness of the patient. The better the quality of care provided to the patient, the more opportunities there are to achieve fidelity with patients. In this sense, health institutions must offer quality services that guarantee patient loyalty; that is, that the person has a certain preference and recommends the institution to others.
According to Díaz and Gil 27, effectiveness is a dimension that acquires great importance in satisfaction. If the users identify a change in their self-care and the fulfillment of the planned objectives, they will recognize the benefits in their state of health. The effectiveness achieved of the expert patient program of this study was achieved thanks to the experiential or experiential learning methodology used, since it allowed to improve knowledge and increase satisfaction. For Gómez-Ramírez et al.25, this methodology is based on Dewey's experiential learning model: the construction of knowledge from a concrete experience is represented as a cyclic process, in which the different phases (concrete experience, reflection, conceptualization and application) they are interrelated In this sense, an experience is not enough to provoke knowledge, but for this to happen, the participation and the cognitive implication of the subject are necessary, looking for meaning about the experienced, relating it to their previous knowledge and developing conceptual structures that allow them to apply the new knowledge to different situations. This method is precise for the type of population of the study in question, since it is about older adults in which, as confirmed by Acero et al. 28, learning is a complex process, composed of a series of essential factors for its realization.
They point out that, for this learning to be effective, at least three areas should be considered: cognitive, affective and psychomotor. Likewise, this educational process must be aligned with the context, the rapid sociocultural changes and the emerging needs. Therefore, it is valid to affirm that this methodological tool is the indicated one, since it allows self-discovery based on facts and based on the interrelation between experience and reflection. This type of learning motivates the training of the people involved, as it enhances their leadership characteristics and decision making, which becomes an essential and synergistic element that is strengthened in their relationship with other individuals.
Finally, this study allows to recognize the usefulness of the expert patient program in the education process that directs the nursing professional as a complementary tool to promote self-care. To the extent that they are more informed, express their needs, be able to make decisions and increase their self-efficacy, patients will adopt an active and co-responsible role that favors the reduction of complications and hospital readmissions.
Health institutions should be more open to the inclusion of these programs, because, by having more informed and responsible patients, the effectiveness is significantly enhanced. In this way, the care provided is transformed, framed in a deliberative and relational model by the professionals, based on active listening, greater degree of participation on the part of the patient and consensus on the actions.
Financial assistance: Internal announcement 2017. Research groups support. Vicerrectoría de Investigación, Pontificia Universidad Javeriana.
REFERENCES
1. Gómez E. Introducción, epidemiología de la falla cardiaca e historias de las clínicas de falla cardiaca en Colombia. Rev Colomb Cardiol. 2016;23:6-12. https://doi.org/10.1016/j.rccar.2016.01.004 [ Links ]
2. Tamayo DC, Rodríguez VA, Rojas MX, Rincón M, Franco M, Ibarra MT, et al. Costos ambulatorios y hospitalarios de la falla cardiaca en dos hospitales de Bogotá. Acta Med Colomb. 2013;38(4):208-212. http://actamedicacolombiana.com/ojs/index.php/actamed/article/view/205 [ Links ]
3. Díaz R, Díaz J, Fuenmayor-Ojeda V, Parejo JA. Insuficiencia cardíaca aguda: análisis clínico epidemiológico. Med Interna. 2018;34(4):224-236. http://www.svmi.web.ve/ojs/index.php/medint/article/view/491 [ Links ]
4. León-González R, García-Esquinas E, Paredes-Galán E, Ferro-Martínez AI, González-Guerrero JL, Hornillos-Calvo M, et al. Alfabetización en salud y resultados de salud en pacientes muy ancianos con insuficiencia cardiaca. Rev Esp Cardiol. 2018; 71(3):178-184. https://doi.org/10.1016/j.recesp.2017.05.029 [ Links ]
5. Contel JC. La atención integrada y el reto de la cronicidad. Enferm Clin. 2018; 28(1):1-4.https://doi.org/10.1016/j.enfcli.2017.12.002 [ Links ]
6. Millaruelo-Trillo JM. Importancia de la implicación del paciente en el autocontrol de su enfermedad: paciente experto. Importancia de las nuevas tecnologías como soporte al paciente autónomo. Aten Primaria. 2010;42 Supl 1:41-47. https://doi.org/10.1016/S0212-6567(10)70007-X [ Links ]
7. De Paz-Ranz S. Escuela de familias y pacientes en una unidad de ictus. Rev Astur Ter Ocu. 2018;13:26-31. https://www.therapeutica.es/index.php/numeros-publicados/ultimo-numero/item/download/245_eea4837c87f816a9a3062c07f0e15095 [ Links ]
8. Lorig K. Chronic Disease Self-Management Program: Insights from the Eye of the Storm. Front Public Health. 2015;3:153. Artículo corregido y publicado de Front Public Health. 2014;2:253. https://doi.org/10.3389/fpubh.2015.00153 [ Links ]
9. González-Mestre A. Autonomía del paciente con enfermedades crónicas: de paciente pasivo a paciente activo. Enferm Clin. 2013;24(1):1-98. https://doi.org/10.1016/j.enfcli.2013.11.005 [ Links ]
10. Griffiths C, Foster G, Ramsay J, Eldridge S, Taylor S. How effective are expert patient (lay led) education programmes for chronic disease?. BMJ. 2007; 334(7606):1254-1256. https://doi.org/10.1136/bmj.39227.698785.47 [ Links ]
11. Holden RJ, Schubert CC, Mickelson RS. The patient work system: An analysis of self-care performance barriers among elderly heart failure patients and their informal caregivers. Appl Ergon. 2015;47:133-150. https://doi.org/10.1016/j.apergo.2014.09.009 [ Links ]
12. Ministerio de la Protección Social. Buenas Prácticas para la Seguridad del Paciente en la Atención en Salud. Bogotá: Ministerio; 2010. http://www.acreditacionensalud.org.co/ea/Documents/Guia%20Buenas%20Practicas%20Seguridad%20del%20Paciente.pdf [ Links ]
13. Badia Rafecas, W., et al. ¿El programa Paciente Experto Catalunya® mejora la adherencia al tratamiento anticoagulante oral?. Revista ROL de Enfermería. 2018;41(3): 210-216. https://medes.com/publication/134752 [ Links ]
14. Miro O, Gil V, Javaloyes O, Llorens P. Acerca de las guías europeas de insuficiencia cardiaca de 2016. Rev Clin Esp. 2018;218(3):158-159. https://doi.org/10.1016/j.rce.2017.10.008 [ Links ]
15. Hall JA, Dornan MC. Meta-analysis of satisfaction with medical care: Description of research domanin and analysis of overall satisfaction levels. Soc Scie Med. 1988; 27(6):935-939. https://doi.org/10.1016/0277-9536(88)90012-3 [ Links ]
16. Molano D. Carolina H. Papel de la enfermería en las unidades de falla cardiaca y educación en falla cardiaca, Rev Colomb Cardiol. 2016;23(S1):31-33. http://dx.doi.org/10.1016/j.rccar.2016.01.009 [ Links ]
17. Salvadó-Hernández C, Cosculluela-Torres P, Blanes-Monllor C, Parellada-Esquius N, Méndez-Galeano C, Maroto-Villanova N, et al. Insuficiencia cardiaca en atención primaria: actitudes, conocimientos y autocuidado. Aten Primaria. 2018;50(4): 213-221.https://doi.org/10.1016/j.aprim.2017.03.008 [ Links ]
18. Barrios K. El conocimiento libre para la transformación universitaria. Congreso Iberoamericano de Ciencia, Tecnología, Innovación y Educación; 2014 Nov 12-14. Buenos Aires: Organización de Estados Iberoamericanos (OEI); 2015. p 1-11. https://www.oei.es/historico/congreso2014/memorias2014.php [ Links ]
19. Molina-Escribano F, Castaño-Moreno E, Massó-Orozco J. Experiencia Educativa con un Paciente Experto. Rev Clin Med Fam. 2008;2(4):178-180. http://www.revclinmedfam.com/articulo.php?art=11 [ Links ]
20. González Assumpció Mestre. La autonomía del paciente con enfermedades crónicas: De paciente pasivo a paciente activo. Enferm Clin. 2014;24(1):67. https://doi.org/10.1016/j.enfcli.2013.11.005 [ Links ]
21. Barreiro M, Velasco E, Renilla A, Torres F, Martín M, De la Hera JM. Grado de conocimiento sobre su enfermedad cardiaca entre los pacientes hospitalizados. Rev Esp Cardiol. 2013;66(3):229-30. https://doi.org/10.1016/j.recesp.2012.07.022 [ Links ]
22. Pesquera-Cabezas R, López-López LM. Un ejemplo innovador en políticas de salud. Gac Sanit. 2016;30(2):158-159. https://doi.org/10.1016/j.gaceta.2015.11.008 [ Links ]
23. Torres-Gonzáles GC, León-Manco RA. Nivel de satisfacción de los pacientes atendidos en el Servicio de Ortodoncia de una Clínica Dental Docente peruana. Revista Estomatol Herediana. 2015;25(2):122-132. https://doi.org/10.20453/reh.v25i2.2458 [ Links ]
24. Santana de Freitas J, Bauer de Camargo Silva AE, Minamisava R, Queiroz Becerra AL, Gomes de Sousa MR. Calidad de los cuidados de enfermería y satisfacción del paciente atendido en un hospital de enseñanza. Rev Latino-Am Enfermagem. 2014;22(3):454-460. https://doi.org/10.1590/0104-1169.3241.2437 [ Links ]
25. Gómez-Ramírez OJ, Carrillo González GM, Cárdenas DC. Encuesta de satisfacción con el cuidado de la salud en las personas con enfermedad crónica. Enferm glob. 2016;15(4):321-330. https://doi.org/10.6018/eglobal.15.4.226851 [ Links ]
26. Ampuero CE. Calidad del servicio y fidelización del paciente en la clínica oftálmica instituto de la visión en el distrito de San Borja 2016 [Tesis de pregrado]. Lima: Universidad Inca Garcilaso de la Vega; 2016: p. 29-31. http://repositorio.uigv.edu.pe/handle/20.500.11818/1714 [ Links ]
27. Diaz M, Gil F. Experiencia con una Nueva Metodología de Enseñanza: Aprendizaje Preferencial Complementario. España: Universidad de Las Palmas de Gran Canaria; 2010: p. 284-285. http://www2.dis.ulpgc.es/~mdiaz/ExperienciaAPC.pdf [ Links ]
28. Acero-Pereira C, Hidalgo MV, Jiménez L. Adult Learning Processes in Non-Formal Education Contexts. Universitas Psychologica. 2018;17(2):155-164. https://doi.org/10.11144/Javeriana.upsy.17-2.paac [ Links ]
Received: February 05, 2019; Accepted: February 21, 2019
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
