










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkEnfermería Global
versão On-line ISSN 1695-6141
Enferm. glob. vol.19 no.60 Murcia Out. 2020 Epub 21-Dez-2020
https://dx.doi.org/10.6018/eglobal.411601
Originals
Effectiveness Home based-Exercise using Mobile Application to Improve Cognitive Functions in Patients with Hypertension: A quesy experimental design
1Faculty member from Department of Nursing, Universitas Pendidikan Indonesia, Bandung, West Java, Indonesia.
2STIKep PPNI Jawa Barat. Indonesia. linlinlindayani@gmail.com
3Associate Professor from Department of electrical engineering, Universitas Negeri Jakarta, Jakarta, Indonesia.
Main Goal:
The purpose of this study was to determine the effect of home based-exercise using mobile application to improve cognitive functions in patients with hypertension.
Methods:
This study was conducted using a queasy experimental with one group pre-post test design at a public health center located in West Java, Indonesia on February to July 2019. A mobile-based exercise program was a walking activity at home every day for one month. The sample in the study was selected using convenience sampling to adults aged above 18 years old and diagnosed with hypertension. The Montreal Cognitive Assessment (MoCA) was used to measure cognitive function. A paired t-test used to analyze data with the significance level was set at 0.05.
Results:
A total of 120 participants were enrolled in this study. The mean age of the sample was 56.42 ± 10.6 years old, 70 (58.3%) were male, 61 (50.8%) had lower education level, and 77 (64.2%) were unemployed. The mean score of MoCA showed improved after intervention, from 23.3 ± 3.42 to 26.7 ± 2.78, p=0.010. In more detail, there were improvement after intervention in domain of naming (2.930.34 vs. 3.141.06, p=0.003), attention (2.39 ± 0.68 vs. 3.12 ± 1.04, p=0.001), and abstraction (1.56 ± 0.49 vs. 2.01 ± 0.89, p=0.043).
Conclusion:
Using a mobile-exercise App was effective, easy to do with low cost to improve cognitive function and prevent dementia in hypertensive patients.
Keywords: cognitive function; exercise; hypertention; mobile application
INTRODUCTION
Hypertension is a major risk caused of the death, accounted for 26.9% of deaths in 2015.1 Previous study have found that hypertension is associated with poor cognitive performance 2, about 46% of patients with hypertension experienced cognitive decline 3. Patients with hypertension have shown an impairment in some cognitive domain such as memory, executive function, and speed of information processing 2,3,4. A study conducted over 20 years showed a U-shaped relationship between cognitive impairment and diastolic blood pressure (DBP). 5 Patients with hypertension have a double risk of cognitive decline compared to the general population. 3 Furthermore, the study found uncontrolled hypertension and treatment of antihypertensive-affected lesions in white matter. 6 In addition, age, gender differences, years of hypertension, body mass index (BMI) is the risk of cognitive deficits. 7,8
Exercise is very important intervention for prevention and management of hypertension. The World Health Organization (WHO) defines exercise as a subcategory of planned, structured, repetitive and directed physical activity with the aim of increasing or maintaining one or more components of physical fitness. 1 Many studies have reported that exercise for patients with hypertension has significant health benefits, one of which is reducing blood pressure 9, increasing oxygen uptake9,10, decrease in body mass index, improve quality of life 9, and reduce depression 10. Exercise has a positive effect on cognitive function, specifically improving memory 12. Based on the results of previous studies, it was found that exercise can slow the rate of cognitive decline 12.
In the digit era, many innovations have been designed to help people physically active. Smartphone technology and cellular applications have shown promising results in physical activity and health promotion. 13 Evidence shows that pedometers, iStepLog, web-based, and text messages are effective for promoting exercise. 14 The results of previous studies reported that there were nearly 97,000 mobile health (mHealth) and fitness applications in 2012 and among the 300 most downloaded applications, 102 were related to exercise and physical fitness. 15 Indonesia is a country with the sixth largest internet user in the world. 16 However, the majority of internet used for social media and only a little is used for other positive things such as monitoring health and fitness conditions. Therefore, the purpose of this study was to determine the effect of mobile app-exercise to improve cognitive functions in patients with hypertension.
MATERIAL AND METHODS
Ethical Aspects
An ethical permission has obtained from the ethical committee at affiliated univeristy (042/KEPK/STIKep/PPNI/JABAR/VII/2019).
Design, study site, period
This study was conducted using a quesy experiemental with one group, pre-post test design to determine the effect of home-exercise using mobile application to improve cognitive functions in patients with hypertension. This study was piloted at one public health center located in Bandung, West Java, Indonesia on February to July 2019.
Study Protocol
The program was created and developed based on the results of team discussions, a literature review, and the American Hearth Association recommendations for hypertension. A mobile-based exercise program was a walking activity at home every day. Participants must do walking exercises with moderate to severe intensity, 40- <60% VO2max or HR (220-age) with frequency of 3 sessions a week for 30 minutes per section. Each session consisted of 5 minutes of warming up, walking exercises with moderate intensity, and 5 minutes of cooling. The intervenstion was conducted for one month.
Before the intervention begins, researchers conducted individual education and counseling programs about the program, including; benefits of walking, how to do walking exercises, preparation before doing exercises (eg measuring blood pressure before exercise, wearing comforTable clothes), monitoring risk for hypertension, procedures for using mobile application, content that need to fill every finish doing a walking exercise/diary books (date & time running, pulse heart before, during, and after walking, complaints of symptoms).
In addition, to monitor their intensity and compliance, we provided diary books, monitor in the mobile application, and weekly phone. During the intervention program, every week of research assistance made a phone visits to collect data (transfer of information and diary books), and follow up on their current program (eg assessing their problems and how they face problems during training) and encourage them to continue to do walking exercises. In addition, research assistants will monitor risk for hypertension, as if participants feel uncomforTable during exercise (eg feeling dizzy), they can stop to exercise and if symptoms continue to develop, we provided an advise to participants to visit the hospital for further examination.
Population, Inclusion And Exclusion Criteria
Participants in the study were adult diagnosed with hypertension.The inclusion criteria were those who had MoCA score less than 25 17, do not do regular exercise (three times a week in the last 6 months), and able to walk. Pariticpants were excluded if they had known condition that affected cognitive function such as stroke, dementia, renal failure, history of drug or alcohol abuse or head injury. The number of samples was calculated using G-Power Software Version 3.1.6 using the F test assuming α = 0.05, medium effect size = 0.12 18, power level = 0.80, so the minimum total sample to be recruited was 120. A convenience sampling methods was used to select participants. Samples were selected when they were in the right place and time of data collection.
Measures
Participants was measured the outcome before and after intervention. Measurement included demographic characteristics, clinical information, and cognitive function. The demographic information were collected during registration. This information included age, level of education, occupation, and montly income. Clinical variables included systolic blood pressure, diastolic blood pressure, smoking history, drinking alcohol. The procedure for measuring blood pressure is done before and after the patient has performed the test, and during the sitting position with the legs not crossed, the feet are flat on the floor, and the left arm is supported at the heart level. In addition, blood pressure was measured using a validated oscillometric noninvasive blood pressure device (OMRON Gold Wireless Bluetooth®). This device is upper Arm home blood pressure monitor is a horizontally designed, dual-display monitor, that stores up to 120 readings for two users (60 readings each) and features a morning hypertension indicator and averaging feature; includes a wide-range D-ring cuff (fits arms 9" to 17" in circumference). The systolic and diastolic values will be used to calculate the average blood pressure. All blood pressure measurements will assess the average value used for analysis.
The Montreal Cognitive Assessment (MoCA) is a cognitive screening instrument developed by Nasreddine et al (2005) in Bahasa Indonesia version. 17 The MoCA test is conducted for 10 minutes to measure seven cognitive domains, including executive functions, naming, verbal memory registration and learning, attention, abstraction, delay recall memory, and orientation. MoCA scores range from 0 to 30, higher scores reflect good global cognitive function. The Indonesian version of MoCA has been validated and showed a good correlation with the MMSE score, the Pearson correlation coefficient between the scores was 0.71 (p<0.005). 19 MoCA-INA showed good validity based on the Transcultural World Health Organization ( WHO ) method with total kappa value between 2 physicians ( inter-rater ) is 0.820. 20
Data Collection Procedure
Research approval was obtained before data collection from the Institutional Review Board in Bandung. For the recruitment of subjects, the researcher informed the inclusion and exclusion criteria to nurses and doctors at the public health centerlocated in Bandung. Participants who meet the inclusion criteria was identified from the doctor and informed to the researcher. Then, we invited prospective participants in a quiet room to explain the purpose of the study, procedures for collecting data, and protecting their rights, for example respecting their autonomy and protecting their confidentiality. When participants understood and agreed to the participants in this study, they needed to sign an informed consent form. After the participant signs the consent form, the researcher conducted an education and personal consultation about the intervention program and collect data at the beginning for the main demographic characteristics and variables.
Data analysis
Descriptive and inferential analysis statistics were used to explain demographic data and main variables. Differences in results between before and after the intervention was evaluated using an pair t test. The significance level was set at 0.05. Data will be analyzed using SPSS version 22 for windows.
RESULTS
Overall, 120 participant were enrolled in this study. We conducted a test of normal distribution and the results showed that data of cognitve function was normally distributed based on the nonsignificant Kolmogorov-Smirnov test. The mean age of the sample was 56.42 ± 10.6 years old. The majority of respondent were male 70 (58.3%), had lower education level 61 (50.8%), and unempoyed 77 (64.2%). The mean of body mass index was in the normal range (23.34 ± 4,4), systolic blood pressure 127.5 ± 11.9), and diastolic blood pressure was 81.92 ± 8.63. About one third of respondent were smoking and none of them drink alcohol (Table 1).

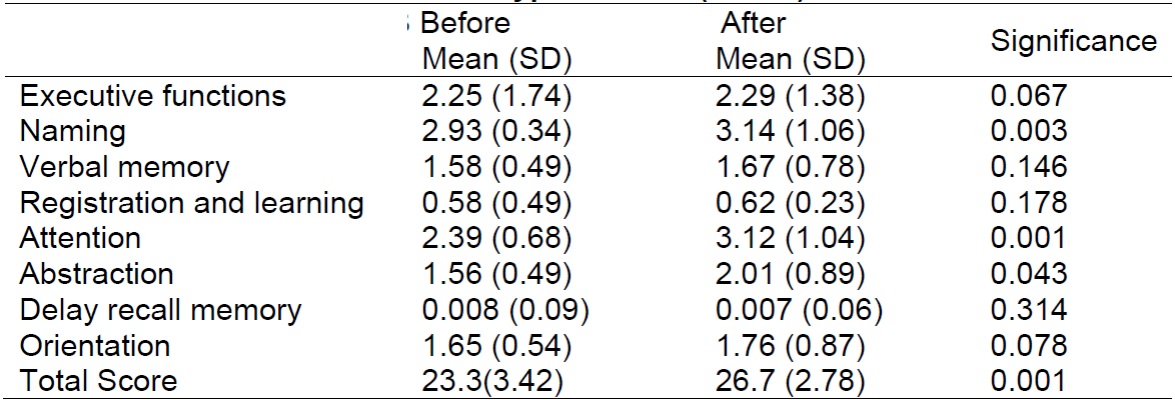
One hundred patients with hypertension completed all baseline data collection and were assigned to mobile-base walking intervention. Findings from pair t test showed that in walking intervention using mobile-base application, the mean score of MoCA showed improved after intervention, from 23.3 ± 3.42 to 26.7 ± 2.78 (p=0.010). In more detail, there were improvement after intervention in domain of naming (2.930.34 vs. 3.141.06, p=0.003), attention (2.39 ± 0.68 vs. 3.12 ± 1.04, p=0.001), and abstraction (1.56 ± 0.49 vs. 2.01 ± 0.89, p=0.043).
We did not found significant result for other cognitive domain such as executive function, verbal memory, registration and learning, deay recall memory, and orientation as measured by MoCA (Table 2).
DISCUSSION
Our study found that by using home based-exercise using mobile application can improve congnitive function in patients with hypertension. Previous evidence reported that the use of a pedometer was associated with a significant increase in physical activity (around 2,000 steps per day) and a reduction in body mass and blood pressure14. Pedometer is a low-cost application, allowing people to track their level of physical activity every day without the enhancements needed to be used like a commercial pedometer. In a pedometer, people must have a predetermined step target (10,000 steps) and a step diary as the main motivating factor for increasing physical activity. It also comes with daily feedback and a percentage of archived goals that can be additional motivational factors to change a person's lifestyle from sedentary to active health. Although the majority of participant were graduated from elemntary school, they had succefull installed the exercise App in their mobile phone. Therefore, utilize technology in the primary care for prevention of cognitive function among patients with hypertension is usefull and workable to enhance their exercise activity.
The mechanism for improving cognitive function through actual exercise is not yet known clearly. Postulates that have existed are neurobiological mechanisms including angiogensis, neurogenesis, and synaptogenesis 4. Exercise increases brain-derived neurotrophic factor (BDNF) levels, which play an important role in neuroplasticity and neuroprotection. Evidence in human studies shows that exercise can increase serum BDNF levels in the brain, hippocampal, prefrontal, and cingulate volumes, and improve memory 21. Future studies included a biomarker to understand the effect of execrcise to the cognitive function is warranted to conduct in Indonesia.
Several studies have been conducted to see the greater benefits of exercise on improving cognitive function. Studies conducted on healthy elderly report that exercise programs carried out for 12 months routinely show more memory improvement. 22 In a systematic review of the effectiveness of exercise in healthy elderly people on improving cognitive function, the exercise program (partly running) with moderate intensity, 30% - <70% VO2 reserve, 3 times per week, for 8 to 42 weeks has an effect positive on cognition 17. Therefore, promoting exercise to all patients with hypertention is very important not only to control their blood pressure but also to prevent from cognitive decline.
This study has some limitation. First, we did not have a control group thus another covariate that may affected the cognitive change were not measured. Second, although all participant had successful installed exercise App in their mobile phone, majority of our respondent were graduated from elementary school thus sometime had difficulty to used mobile App. However, this study has several strengths, first, this is first study conducted in low income country to utilized the digital application to help people organized their exercise and this study conducted in one of the biggest cities in Indonesia that may be can represent condition of hypertensive patients in Indonesia in general. Therefore, future studies conducted using more rigorous methods is warranted to see the true effect of this technology. Second, we used MoCA instead of MMSE that considered as more validated questionnaire to measure cognitive function.
CONCLUSIONS
In conclusion, our study highligth that the used of mobile-App for exercise is promosing approch to enhance physical activity, thus improve their cognitive function. Future study using rigors method exploring effect of mobile-App for exercise is very important to provide stronger evidence. Health care professional may try to utilize technology in providing care, particularly in promoting exercise.
REFERENCES
1. WHO. World Health Statistic 2015. WHO: Geneva. Retrieved from http://www.who.int/gho/publications/world_health_statistics/2015/en/ [ Links ]
2. Scullin, MK, Gordon, BA, Shelton, JT, Lee, JH, Head, D, & McDaniel, MA Evidence for a detrimental relationship between hypertension history, prospective memory, and prefrontal cortex white matter in cognitively normal older adults. Cognitive Affection Behaviour Neuroscience. 2013;13(2): 405-416. doi:10.3758/s13415-013-0152-z [ Links ]
3. Vicario, A, del Sueldo, MA, Zilberman, JM, & Cerezo, GH. Cognitive evolution in hypertensive patients: a six-year follow-up. Vascular Health and Risk Management. 2005; 7: 281-285. doi:10.2147/vhrm.s18777 [ Links ]
4. Kohler, S, Baars, MA, Spauwen, P, Schievink, S, Verhey, FR, & van Boxtel, MJ Temporal evolution of cognitive changes in incident hypertension: prospective cohort study across the adult age spAn Hypertension. 2011; 63(2): 245-251. doi:10.1161/hypertensionaha.113.02096 [ Links ]
5. Taylor, C, Tillin, T, Chaturvedi, N, Dewey, M., Ferri, CP, Hughes, A, Stewart, R. Midlife hypertensive status and cognitive function 20 years later: the Southall and Brent revisited study. Journal of the American Geriatrics Society. 2013; 61(9):1489-1498. doi:10.1111/jgs.12416 [ Links ]
6. Kuller, LH, Margolis, KL, Gaussoin, SA, Bryan, NR, Kerwin, D, Limacher, M, Robinson, JG. Relationship of hypertension, blood pressure, and blood pressure control with white matter abnormalities in the Women's Health Initiative Memory Study (WHIMS)-MRI trial. Journal of Clinical Hypertension. 2010; 12(3):203-212. doi:10.1111/J1751-7176.2009.00234.x [ Links ]
7. Wang, W, Lau, Y, Loo, A, Chow, A, & Thompson, DR. Medication adherence and its associated factors among Chinese community-dwelling older adults with hypertension. Heart & Lung: The Journal of Acute and Critical Care. 2014; 43(4): 278-283. doi: http://dx.doi.org/10.1016/Jhrtlng.2014.05.001 [ Links ]
8. Lo, AH, Woodman, RJ, Pachana, NA, Byrne, GJ, & Sachdev, PS. Associations between lifestyle and cognitive function over time in women aged 40-79 years. Journal of Alzheimers Dis. 2014; 39(2):371-383. doi:10.3233/jad-130971 [ Links ]
9. Cornelissen, VA, Fagard, RH, Coeckelberghs, E, & Vanhees, L. Impact of resistance training on blood pressure and other cardiovascular risk factors: a meta-analysis of randomized, controlled trials. Hypertension. 2011; 58(5): 950-958. doi:10.1161/hypertensionaha.111.177071 [ Links ]
10. Asikainen, TM, Miilunpalo, S, Oja, P, Rinne, M, Pasanen, M, Uusi-Rasi, K, & Vuori, I. Randomised, controlled walking trials in postmenopausal women: the minimum dose to improve aerobic fitness? Brith Journal of Sports Medicine. 2012; 36(3): 189-194. [ Links ]
11. Bernard, P, Ninot, G, Bernard, PL, Picot, MC, Jaussent, A, Tallon, G, & Blain, H. Effects of a six-month walking intervention on depression in inactive post-menopausal women: a randomized controlled trial. Aging Mental Health. 2015; 19(6):485-492. doi:10.1080/13607863.2014.948806 [ Links ]
12. Smith, PJ, Blumenthal, JA, Hoffman, BM, Cooper, H, Strauman, TA, Welsh-Bohmer, K, Sherwood, A. Aerobic exercise and neurocognitive performance: a meta-analytic review of randomized controlled trials. Psychosomatic Medicine. 2010; 72(3): 239-252. doi:10.1097/PSY.0b013e3181d14633 [ Links ]
13. Bort-Roig J, Gilson ND, Puig-Ribera A, Contreras RS, Trost SG. Measuring and influencing physical activity with smartphone technology: a systematic review. Sports Medicine. 2014; 44(5):671-86. doi: 10.1007/s40279-014-0142-5. [ Links ]
14. Lee LL, Kuo YC, Fanaw D, Perng SJ, Juang IF. The effect of an intervention combining self-efficacy theory and pedometers on promoting physical activity among adolescents. Journal Clinical Nursing. 2012; 21(7-8):914-22. doi: 10.1111/J1365-2702.2011.03881.x. Epub [ Links ]
15. Adamakis M. Nike+ Training Club, an ultimate personal trainer: mobile app user guide. British Journal of Sports Medicine. 2018; 52(13):e2. doi: 10.1136/bjsports-2017-098414. [ Links ]
16. Kominfo. Penguna Internet di Indonesia 2018. Available at: https://www.kominfo.go.id [ Links ]
17. Nasreddine, ZS, Phillips, NA, Bédirian, V, Charbonneau, S, Whitehead, V, Collin, I, Chertkow, H. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. Journal of the American Geriatrics Society. 2005; 53(4): 695-699. [ Links ]
18. Cohen, J A power primer. Psychological Bulletin.1992 112(1), 155-159. doi:.1037/0033-2909.112.1.155 [ Links ]
19. Rambe, AS, & Fitri, FI. Correlation between the Montreal Cognitive Assessment-Indonesian Version (Moca-INA) and the Mini-Mental State Examination (MMSE) in Elderly. Open Access Macedonian Journal of Medical Sciences. 2017; 5(7).doi:10.3889/oamjms.2017.202 [ Links ]
20. Husein N, Silvia L, Yetty R dkk. Uji Validitas dan Reabilitas Montreal Cognitive Assessment Versi Indonesia (MoCA-Ina) Untuk Skrining Gangguan Fungsi Kognitif. Neurona Neuro Sains. 2010;27(4):15-22. [ Links ]
21. Ruscheweyh, R, Willemer, C, Kruger, K, Duning, T, Warnecke, T, Sommer, J, Floel, A. Physical activity and memory functions: an interventional study. Neurobiol Aginng. 2012; 32(7):1304-1319. doi:10.1016/Jneurobiolaging.2009.08.001 [ Links ]
22. van Uffelen, JG., Chin, APM J, Hopman-Rock, M, & van Mechelen, W. The effects of exercise on cognition in older adults with and without cognitive decline: a systematic review. Clinical Journal of Sport Medicine. 2008; 18(6): 486-500. doi:10.1097/JSM.0b013e3181845f0b [ Links ]
Received: January 26, 2020; Accepted: July 04, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
