










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.20 n.61 Murcia Jan. 2021 Epub Feb 01, 2021
https://dx.doi.org/10.6018/eglobal.418881
Originals
Fall and demographic and clinical factors in older adults: follow-up study
1 Doctor of Science. Professor, Medical-Surgical Department, School of Nursing, University of São Paulo. Brazil. betofhon@usp.br
2PhD in Nursing. Full Professor, Department of General and Specialized Nursing, Ribeirão Preto School of Nursing, University of São Paulo.
Objective:
To analyze the demographic and clinical factors related to falls of older adults living at home in a five-year follow-up
Materials and methods:
Retrospective quantitative and longitudinal study conducted between 2007/2008 and 2013 with 262 Brazilians participants over 65 years old. We used the demographic profile, Mini-Mental State Examination, self-reported diseases, falls and their characteristics, Edmonton Frail Scale, Lawton and Brody Scale, Functional Independence Measure instruments. We performed descriptive analysis, Chi-squared, Wilcoxon test and mixed model test.
Results:
Most participants were women, aged between 65 to 79 years, schooling between 1 to 4 years and retired. The prevalence of falls was 21.8% and 37.8% in both evaluations. We verified that the chance of suffering a new fall increases for each additional disease of the older adult. In addition, for each point to more on the frail scale, the older adult has a greater chance of falling. On the other hand, for each medication withdrawn, the chance of falling decreases 10%.
Conclusion:
The fall was associated with clinical factors in older adults, therefore constant evaluations must be carried out to identify this event and its triggers.
Keywords: Aged; Accidental falls; Frailty; Longitudinal studies; Health personnel; Accident consequences
INTRODUCTION
Life expectancy is increasing worldwide as is the number of people aged 60 years and over. Data from the World Population Prospects show that in 2019 one in 11 people in the world was over 65 (9%), and by 2050, the projection is one in six (16%). In addition, the number of people aged 80 and over is projected to triple, from 143 million in 2019 to 426 million in 2050 1.
With the aging process, physiological changes of older people can lead to multiple syndromes; falling is one of them. The World Health Organization (WHO) reports that this is the second leading cause of death from non-accidental injuries, with an estimated 646,000 fatal falls per year in the world 2, which can be considered a public health issue.
The prevalence of falls can affect approximately 24% to 50% of older adults over 60 years old3. In addition, in the United States, one older adult falls every 20 minutes 4, costing $50 billion dollars in medical expenses in non-fatal falls and $754 million dollars in fatal ones5.
In Brazil, the Informatics Department of the Unified Health System - DATASUS, reported that between 2007 and 2017 this was the cause of death of 11,078 individuals over 60 years old diagnosed according to ICD-10. We identified 7,996 deaths, among which 1,192 were people between 60 and 69 years old, 2,023 deaths were people between 70 and 79, and 4,781 were deaths of people over 80 years old6.
The decrease may be the result of the interaction between the intrinsic factors and those related to the individual himself 7, the presence of acute or chronic diseases, and extrinsic factors 8. We identified in the literature that most falls occur during daily activities 7, and recurrent falls can lead to the fear of falling syndrome 9.
The fall can be caused by the aging process linked to other factors that can lead older people to a partial or total disability, harming their autonomy and independence. The role of the health professional is to observe older adults and detect what triggers their fall in order to prevent them. Therefore, our study aimed to analyze demographic and health factors related to falls in older people who live at home in a five-year follow-up.
MATERIALS AND METHOD
This is a retrospective longitudinal study carried out from October 2007 to March 2008 (T1), and from July to December 2013 (T2) in the city of Ribeirão Preto, São Paulo, Brazil.
Probabilistic sampling was used (two-stage cluster method). For the first phase, the census sector was considered as the Primary Sample Unit (PSU). From the 600 sectors of the city, 30 with probability proportional to the size of the number of addresses were randomly chosen. In the second phase, the street and blocks of the sectors in each sector were also chosen randomly.
Sample errors were set at around 10%, and for fall prevalences up to 70%. Confidence intervals for estimated prevalences in later strata defined by gender and age considered 10% as the maximum error tolerance, with 515 participants as the final sample.
The inclusion criteria in T1 were: older adults with 65 years or older, of both gender, capable of verbal communication and living in the urban area; in T2, the criterion was to have participated in the first evaluation.
In T1, data were collected clockwise; in T2, the elderly or family member were called to schedule a home visit. For those older adults that telephone contact was not possible, it was necessary to send the researchers to the address and schedule a visit.
The participant had to fill in a form to identify personal data, self-reported diseases, the number of medication used according to the last prescription, number of falls in the last 12 months, their characteristics, causes, physical, psychological and social consequences.
The Mini-Mental State Examination (MMSE) was translated and validated in Portuguese10. The score varies from zero to 30, and the cut-off points were 20 for unschooled, 24 for those between 1 and 4 years of schooling, 26.5 for 5 to 8 years, 28 for 9 to 11 years, and 29 for those with schooling higher than 11 years.
The Functional Independence Measure (FIM) was validated 11 in Portuguese. Among the activities evaluated are the performance of 18 joint activities related to self-care, transfers, locomotion, bowel and bladder control, communication and social cognition including memory, social interaction and problem solving, with a score between 18 and 126 points.
The Lawton and Brody Scale identifies the Instrumental Activities of Daily Living (IADL), validated for the Brazilian context 12. Its score ranges from seven to 21 points, characterizing the participant as fully dependent, partially dependent and independent.
The Edmonton Frail Scale (EFS), created by the Canadian Initiative on Frailty and Aging (CIF-A) group, was validated and replicated for Brazil 13. The scale evaluates nine domains represented in 11 items and presents a score from zero to 17 points; the higher the score on the scale, the higher the level of frailty.
For the analysis of the information, we used the Statistical Package for the Social Sciences Program - SPSS v. 25.0. Descriptive statistics were used, and for the quantitative variables, we used the measure of central tendency (mean) and dispersion (standard deviation); and for the categorical, we used frequencies and percentages.
The normality test was performed for quantitative variables such as EFS, FIM, IADL, self-reported diseases and number of medications. When this parameter was not identified, the Wilcoxon non-parametric test was used. Chi-squared test was used for categorical variables.
In the final analysis, the fall variable was divided into yes and no, and the exploratory variables considered in the final model were gender (male and female), marital status divided into with partner (married) and without partner (single, widowed and divorced). Time, in this case, is 2013, and among the health variables are the self-reported diseases, the number of medications used, the scores of the EFS, FIM and IADL. For all statistical tests, the significance value was ≤0.05.
The study was approved by the Research Ethics Committee of the Ribeirão Preto College of Nursing of the University of São Paulo, protocol No. 0851/2007 for T1 and protocol No. 1392/2011 for T2.
RESULTS
The sample was composed of 515 participants in T1 and 262 in T2. Among the losses in the course of the five years, we verified that 127 (24.7%) died, 83 (16.1%) refused to participate in T2, 8 (1.6%) were institutionalized, and 35 (6.8 %) moved to other cities.
Regarding the demographic profile in T2, the study showed that most participants were female, aged between 65 and 79 years, 1 to 4 years of schooling and retired. In addition, there was a predominance of widowers (Table 1).

In relation to the fall, of the 262 older adults, the prevalence was 21.8% in T1 and 37.8% in T2. We verified that in both phases there was a predominance of those who suffered just one fall (Table 2).
Table 2: Prevalence and number of falls of older adults living at home in 2007/2008 - 2013 follow-up. Ribeirão Preto, Brazil, 2019.

In the bivariate analysis, in T1, an association was found between fall and IADL, frailty and number of diseases. In T2, the fall was associated with frailty, number of diseases and number of medications (Table 3).
Table 3: Association between falls with demographic and health variables of older adults living at home. Ribeirão Preto, Brazil, 2019.

*Chi-squared; † Wilcoxon Test; p<0.05
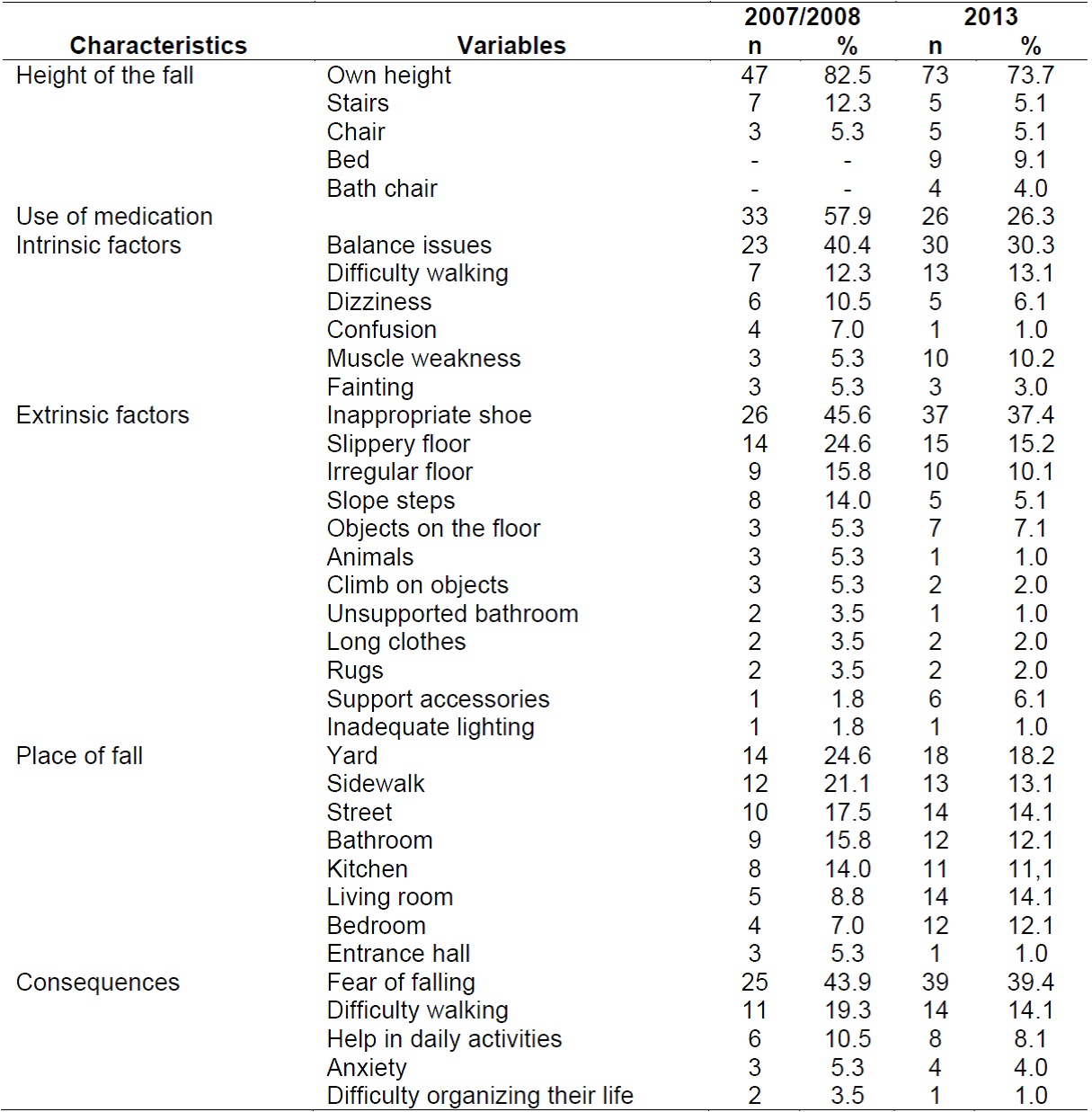
When comparing the characteristics of the fall, in T1, 82.5% of them were from their own height, 57.9% used medications, 40.4% presented balance issues, 45.6% were related to the use of inappropriate shoes, 24.6 % fell in their yard, and 43.9% were afraid of falling again.
In T2, 73.7% fell from their own height, 26.3% used some type of medication, 30.3% had a balance issues, 37.4% wore inappropriate shoes, 18.2% indicated that they fell in their yard, and 39.4% reported being afraid of falling again (Table 4).
Table 4: Characteristics of the fall and its consequences in older adults living at home. Ribeirão Preto, Brazil, 2019.
In the regression of mixed models ,we observed that the participant has more chance of falling in T2 if compared with T1. Regarding the number of illnesses, we verified that for each additional illness, the chance of falling again increases.
In addition, for each extra point in the EFS, the older adult's chance of falling increases. On the other hand, for each medication withdrawn, the chance of falling is 10% lower (Table 5).

DISCUSSION
We verified that, for older adults, falling increases over time as the number of diseases and frailty get higher. Also, consuming fewer medications decreases the chance of falling.
Falling is the most frequent cause of injury in older adults, especially for older ones, which can lead to decreased functionality and death. In this study, the prevalence of falls was 21.8% in T1 and 37.8% in T2. An American study analyzed the prevalence of this event between 1988 and 2010, the authors identified that the prevalence of falls was 28.2% in the first evaluation and 36.3% in the second 14.
Another study conducted at home in England identified a prevalence of falls of 28.4% in the last two years 15. This increase is due to higher life expectancy and more activities of daily living at home and in the street 16.
The fall is linked to postural disturbances and to gravity, which are important to maintain postural balance 17. In addition, it is also linked to the nervous system that regulates the musculoskeletal system guaranteeing posture control, usually lost in the aging process18.
The study shows that the causes of falling in both evaluations were from their own height and from use of inappropriate shoes. The most common place of the fall was the yard and they were afraid of falling again. Studies with similar results were carried out in Peru 3 and the United States 19.
Falling from their own height is an unintentional event that results in the change of position of the individual to a lower level in relation to their initial position 20. The consequences of this type of fall, in most cases, can go unnoticed by the health professional.
The use of inappropriate shoes has been identified as a contributor to up to 45% of falls 21. Also, walking barefoot or in socks can also increase this risk. Additionally, wearing boots or high heels have been shown to increase risk and impair balance 22.
On the other hand, the fear of falling is a psychological phenomenon that leads to anxiety, depressive symptoms, psychological stress 23, decrease or loss of functional independence, and can cause social isolation in older adults 3.
The study showed that older adults have more chance of falling when the number of chronic diseases and the consumption of medication are higher. The growth rate of the population aged 60 and over is about three times higher in less developed countries due to decreased mortality and improvement in life expectancy. However, this growth increases the prevalence rates of non-communicable diseases and disability 24.
According to the Prescribing Cost Analysis in England, the total number of medication dispensed in 2015 was 1.08 billion, corresponding to an average of 19.9 medications per patient 25. A study with 5,213 older adults identified that 1,611 used more than four medications per day, and 569 reported having suffered from falls. In addition, the participants considered in polypharmacy suffered 18% more falls compared to those not in polypharmacy; and those who use more than 10 medications have a 50% rate of falling 26.
Older adults who use antidepressants, sedatives, or hypnotics and antiepileptics are more likely to experience recurrent falls. Additionally, polypharmacy increases 1.5 to 2 times the chance for recurrent falls in older adults considered older 27.
Regarding frailty, we verified that older adults have more chance of falling. A systematic review with meta-analysis identified 19 longitudinal studies, and in their evaluation, an association between fall and frailty was identified (OR 1.80, 95% CI, 1.51-2.13) 28. In addition, another study identified that the factors that influence falls in frail older adults are dizziness, difficulty walking, and fear of falling 7.
Frailty and falls are syndromes with multifactorial health conditions that occur when the accumulated effects of the deficit of different systems make the person more vulnerable. Both share the pathophysiological mechanisms, risk factors and are the result of adverse events 29. In China, in a study with 500 frail older adults, the authors verified a 41.5% prevalence of falls with a predominance of women and 80 year-olds and older, causing serious injuries30.
Among the limitations is the number of losses during follow-up; however the data shows the importance of a different view by the multi-professional health team. Another is the five-year interval between the two periods of fall evaluation, which hindered a more detailed analysis.
The results show the importance of the evaluation of older adults by a health professional to identify the fall and the demographic and clinical factors associated with this event, such as the frailty syndrome.
CONCLUSION
In this study, we identified that older adults' increasing risk of falling is associated with frailty and number of diseases. However, the chance of falling decreases if their medication is reduced.
Longitudinal studies are essential in the multidimensional evaluation of older adults, which indicates the importance of evaluation by a multi-professional health team. Local government investment is necessary for the prevention of falls, as well as the development of research for prevention, curative treatment and rehabilitation, in order to reduce disability and, consequently, the loss of independence.
REFERENCIAS
1. United Nation. Ageing. 2019. Fecha de consulta: 12 de diciembre de 2019. Disponible en: https://www.un.org/en/sections/issues-depth/ageing/ [ Links ]
2. World Health Organization. Falls. 2018. Fecha de consulta: 5 de diciembre de 2019. Disponible en: http://www.who.int/news-room/fact-sheets/detail/falls [ Links ]
3. Silva-Fhon JR, Partezani-Rodrigues R, Miyamura K, Fuentes-Neira W. Causas y factores asociados a las caídas del adulto mayor. Enfermería Universitaria. 2019;16(1):31-40. [ Links ]
4. Center for Diseases Control and Prevention. Older adult falls. 2016. Fecha de consulta: 8 de diciembre de 2019. Disponible en: https://www.cdc.gov/homeandrecreationalsafety/falls/index.html [ Links ]
5. Florence CS, Bergen G, Atherly A, Burns E, Stevens J, Drake C. Medical costs of fatal and nonfatal falls in older adults. J Am Geriatr Soc. 2018;66(4):693-698. [ Links ]
6. Sistema DATASUS. Informações de saúde. 2019 Fecha de consulta: 20 de diciembre de 2019. Disponible en: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sim/cnv/obt10uf.def [ Links ]
7. Callis N. Falls prevention: identification of predictive falls risk factors. Appl Nurs Res. 2016;29:53-8. [ Links ]
8. Ravindran RM, Kutty VR. Risk factors for fall-related injuries leading to hospitalization among community-dwelling older persons: a hospital-based case-control study in Thiruvananthapuram, Kerala, India. Asia Pac J Public Health. 2016;28(1):70S-76S. [ Links ]
9. Tomita Y, Arima K, Tsujimoto R, Kawashiri SY, Nishimura T, Mizukami S, et al. Prevalence of fear of falling and associated factors among Japanese community-dwelling older adults. Medicine. 2018;97(4):e9721. [ Links ]
10. Brucki SMD, Nitrini R, Caramelli P, Bertolucci PHF, Okatomo IH. Sugestões para o uso do mini-exame do estado mental no Brasil. Arq Neuropsiquiatr. 2003;61(3-B):777-781. [ Links ]
11. Riberto M, Miyazaki MH, Jucá SSH, Sakamoto H, Pinto PPN, Battistella LR. Validação da versão brasileira da medida de independência funcional. Acta Fisiatr. 2004;11(2):72-76. [ Links ]
12. Santos RL, Virtuoso Júnior JS. Confiabilidade da versão brasileira da escala de atividades instrumentais da vida diária. RBPS. 2008;21(4):290-296. [ Links ]
13. Fabricio-Wehbe SCC, Cruz IR, Haas VJ, Diniz MA, Dantas RAS, Rodrigues RAP. Reproducibility of the Brazilian version of the Edmonton Frail Scale for elderly living in the community. Rev Latino-am Enfermagem. 2013;21(6):1330-6. [ Links ]
14. Cigolle CT, Há J, Min LC, Lee PG, Gure TR, Alexander NB, et al. The epidemiologic data on falls, 1998-2010: more older Americans report falling. JAMA Intern Med 2015;175(3):443-445. [ Links ]
15. Gale CR, Cooper C, Sayer AA. Prevalence and risk factors for falls in older men and women: The English longitudinal study of ageing. Age ageing, 2016;45:789-794. [ Links ]
16. Pimentel WRT, Pagotto V, Stopa SR, Hoffmann MCCL, Andrade FB, Souza Junior PRB, et al. Quedas entre idosos brasileiros residentes em áreas urbanas: ELSI-Brasil. Rev Saude Publica. 2018;52(Supl 2):12s. [ Links ]
17. Cruz E, González M, López M, Godoy ID, Pérez MU. Caídas: revisión de nuevos conceptos. Revista HUPE. 2014;13(2):86-95. [ Links ]
18. Alfieri FM, Silva NOV, Kutz NA, Salgueiro MMHAO. Relações entre equilíbrio, força muscular, mobilidade funcional, medo de cair e estado nutricional de idosos da comunidade. Kairós Gerontologia. 2016;19(2):147-165. [ Links ]
19. Landers M, Oscar S, Sasaoka J, Vaughn K. Balance confidence and fear of falling avoidance behavior are most predictive of falling in older adults: prospective analysis. Phys Ther. 2016;96(4):433-442. [ Links ]
20. Moura RN, Santos FD, Driemeier M, Santos LD, Ramos LR. Quedas em idosos: fatores de risco associados. Gerontologia. 1999;7(2):15-21 [ Links ]
21. Boelens C, Hekman EE, Verkerke GJ Risk factors for falls of older citizens. Technol Health Care. 2013; 21(5): 521-33. [ Links ]
22. Van der Cammen TJM, Sterke CS, Halilovic A, Molenbroek J Influence of footwear on gait characteristics that are associated with increaser falls risk in older persons. The ergonomics open journal, 2016;9:43-49. [ Links ]
23. Santos SCA, Figueiredo DMPPreditores do medo de cair em idosos portugueses na comunidade: um estudo exploratório. Ciên saúde coletiva. 2019;24(1):77-86. [ Links ]
24. Kampfen F, Wijemunige N, Evangelista Jr B. Aging, non-communicable diseases and old-age disability in low and middle-income countries: a challenge for global health. Int J Public Health. 2018;63(9):1011-1012. [ Links ]
25. Health & Social Care Information Centre. Prescription Cost Analysis England 2015. 2016. Fecha de consulta: 30 de noviembre de 2019. Disponible en: https://files.digital.nhs.uk/publicationimport/pub20xxx/pub20200/pres-cost-anal-eng-2015-rep.pdf [ Links ]
26. Dhalwani NN, Fahami R, Sathanapally H, Seidu S, Davies MJ, Khunti K. Association between polypharmacy and falls in older adults: a longitudinal study from England. BMJ Open. 2017;7:e016358. [ Links ]
27. Ming Y, Zecevic A. Medications and polypharmacy influence on recurrent faller in community: a systematic review. Can Geriatr J 2018;21(1):14-25. [ Links ]
28. Fhon JRS, Rodrigues RAP, Neira WF, Huayta VMR, Robazzi MLCC. Queda e sua associação à síndrome da fragilidade no idoso: revisão sistemática com metanálise. Rev Esc Enferm USP. 2016;50(6):1005-1013. [ Links ]
29. Inouye SK, Studenski S, Tinetti ME, Kuchel GA. Geriatric syndromes: clinical, research, and policy implications of a core geriatric concept. J Am Geriatr Soc. 2007;55(5):780-791. [ Links ]
30. Pi HY, Hu MM, Jie Z, Peng PP, Nie D. Circumstances of falls and fall-related injuries among frail elderly under home care in China. International journal of nursing sciences, 2015;2(3):237-342. [ Links ]
Received: March 17, 2020; Accepted: July 04, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
