










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.20 n.63 Murcia Jul. 2021 Epub Aug 02, 2021
https://dx.doi.org/10.6018/eglobal.470721
Originals
Information dynamics in nursing professionals based on social network análisis
1 Fundación San Juan de Dios. Centro Universitario de Ciencias de la Salud San Rafael-Nebrija. Universidad Nebrija. Madrid. España. gescobar@nebrija.es
2 Grupo de Investigación SALBIS. Facultad de Ciencias de la Salud, Universidad de León, Campus, Ponferrada. España.
3 Facultad de Ciencias de la Documentación. Departamento de Biblioteconomía y Documentación. Universidad Complutense de Madrid. Madrid. España.
4 Departamento de Ciencias Biomédicas. Facultad de Veterinaria. Universidad de León. Campus de Vegazana, León, España.
5 Departamento de Ingeniería Eléctrica y de Sistemas y Automática. Universidad de León, Campus de Vegazana, León, España.
Introduction
Knowledge is a necessary tool for scientific research and progress in any discipline. But scientific knowledge and information dynamics are not only sustained by individuals but are produced and maintained by groups of people working in the same environment where links and relationships can influence the process.
Aim:
To analyze the social networks of information source utilization, help/advice for knowledge transfer and the places where nursing professionals share information.
Method:
Analysis of social networks through a validated questionnaire. Professionals from 6 hospital units were recruited.
Results:
77 professionals participated with a mean age of 42.9 (SD:11.48). Peers were the most frequently used source of information (76 choices) compared to databases and scientific articles, which were the least selected (63 choices). Horizontal homophilous networks (professionals with similar status/interests) are the most frequent for obtaining information on research results (74 choices). The care unit is the most pointed environment for sharing information (50 choices).
Conclusions:
Professionals consider the knowledge of their peers as the main source for obtaining information on research results. Units with a certain degree of specialization use clinical practice guidelines and protocols as the main source of information. Nursing professionals use homophilic-horizontal networks to obtain information. The work environment in its different settings (unit, office, meetings) is the most used for sharing information on research results.
Key words: Social Network Analysis; Information sources; Knowledge Management; Nursing; Evidence-Based Practice; Research utilization
INTRODUCTION
Knowledge, conditioned by information dynamics, is a necessary tool for scientific research and the progress of any discipline 1. Tacit knowledge relates to experience-based elements that are used for problem solving 2,3 and explicit knowledge refers to formal information obtained through scientific literature and specialised documents, such as clinical practice guidelines, standardised protocols, scientific journals and books, among others 2.
The underestimation of tacit knowledge, together with the complexity of the care context of practice, are interrelated as possible causes of the gap between research results and clinical decision-making. This situation is visible in the refusal of some professionals to modify their practice when they must incorporate available evidence that does not relate to their experience. However, tacit knowledge is highly valued when it comes from experienced professionals 2. On many occasions, nursing professionals draw on the experience of other professionals to inform their practice and that experience may or may not be supported by research 4.
Effective knowledge is likely to depend on the combination of a tacit knowledge base, gained through clinical practice, with scientific or explicit knowledge. Thus, information sources for decision-making in nursing include both tacit and explicit knowledge 4. This reality allows us to affirm that even the most explicit knowledge is not devoid of tacit knowledge, since its use is carried out in a specific context, linked to ethical and moral principles, the individual's own culture and personal experiences 2.
Therefore, research utilisation can be understood as a process in which health professionals combine explicit, research-based knowledge with tacit, practice-based knowledge, i.e. both knowledge is brought together for use in the context of their daily work 5.
On the other hand, for more than 4 decades studies have established the existence of a great separation between research and clinical practice, which has meant that the results of research do not contribute to the improvement of care, as would be desirable in principle 6. This takes place in a context that directly involves the nursing professional in the use of research. Firstly, because nursing professionals are increasingly aware of and have access to evidence, and secondly, because the nursing role is acquiring dimensions never seen before in which research plays a transcendental role. Proof of this is the designation by the WHO and ICN of 2020 as the International Year of Nursing, which has given rise to the Nursing Now movement; focusing on the transcendental position of nursing in the different health scenarios and the responsibility that it acquires to generate solid evidence that can demonstrate the impact of care on the health of citizens, individuals, the community, among others 7.
But to generate evidence and analyse its impact it is important to understand how nursing professionals manage scientific knowledge. It should also be borne in mind that scientific knowledge is not only held by individuals, but is produced and maintained by groups of people working in the same environment, where the links and relationships between professionals can influence the process 5,8.
Parcham et al. report that within the healthcare environment, different professional groups establish different social networks; pointing out how doctors, for example, tend to create informal horizontal networks, relating to professionals with similar status and interests; this is the so-called homophily effect, in order to obtain information from other doctors with more experience in their speciality. On the other hand, they reflect that nursing professionals tend to establish formal vertical networks, relating to professionals with different status and interests 9. Horizontal networks are more effective for making use of peer influence, while vertical networks are more effective for decision approval 10.
Studies that have explored how scientific knowledge is identified, circulated, evaluated and used in healthcare organisations suggest that before it can contribute to organisational change initiatives, it must be incorporated into the self-knowledge constructed and shared by the people who make up the organisation. Knowledge then depends on its circulation in interpersonal networks, and will be disseminated if these social links are taken into account and any barriers are identified and overcome 11.
To capture the professional relationships or networks that coexist in healthcare organisations, a methodology is available to identify the structures of relationships that are generated during the use of information to influence knowledge: Social Network Analysis (SNA). SNA draws on theories and techniques to understand how social relationships influence behaviour 12.
The use of SNA is increasingly present in the health context and its applicability is wide. Focusing on the field of health education, studies have been published that focus on aspects related to the acquisition of healthy lifestyles in the context of peer interaction. A study conducted in a school setting with adolescents explored the relationship between socioeconomic status and obesity, analysing peer contact patterns taking this parameter into account 13. Along the same lines, the study by Quiroga et al. focused on adolescent friendship networks and alcohol consumption, to support the design of preventive strategies taking into account how certain variables (socioeconomic status, overweight, alcohol consumption, friendship patterns) influence the formation of social networks that mediate the acquisition of healthy lifestyles 14.
In the hospital setting, a study in palliative care used the SNA to explore how the communication process between nurses, patient and environment unfolds. This made it possible to understand certain behaviours and to plan strategies for improvement 15. Or studies such as the one conducted by Creswick & Westbrook in which they explored the advice networks of nursing professionals regarding the use of medication16.
Therefore, if we assume that it is a proven fact that health professionals influence the process of implementation of scientific knowledge in clinical practice, as they form part of professional subcultures that intervene in the dissemination of ideas and knowledge17, SNA can help to understand certain phenomena related to the dissemination and use of evidence in nursing professionals, which have to do with interpersonal relationships; and with this, to analyse the context in which these connections and dynamics for obtaining information take place.
The aim of this proposal is to analyse the social networks for the use of information sources, help or advice for the transfer of knowledge and the places where nursing professionals share information.
MATERIAL AND METHODS
The scope of the study is the Móstoles University Hospital (Autonomous Community of Madrid, Spain) during 2018. This hospital centre participated in the Sumamos Excelencia( scientific evidence implementation project, being the centre with the most participating units 18.
The study subjects are nursing professionals belonging to six units of this hospital. Five of them had participated six months earlier in the project described above, but not the sixth (understand as control unit).
The inclusion criteria for the nursing professionals of the participating units were permanent professionals on staff related to the care process who had been part of the Sumamos Excelencia( implementation project; management professionals who participated in the implementation project and professionals who agreed to participate in the study. Professionals with temporary contracts of less than 3 months were excluded.
We started with a stratified probability sampling by units to recruit at least one medical, one surgical, one critical care and one mixed unit. In the units that participated in the implementation project, non-probability purposive sampling was performed to include all professionals who met the criteria. In the case of the control unit, the sampling was consecutive non-probability sampling including all the professionals in the unit who decided to participate once the project had been explained. The sample size was conditioned by the number of professionals working in the participating units and participating in the implementation project.
To collect the information, a questionnaire was created and validated (content validity index) consisting of 7 items plus a set of socio-demographic and professional variables19. According to the objective of this proposal, the method of the three items addressed is presented.
Item 1, validated in Spanish by Escobar Aguilar G et al, deals with the use of research, according to item 6 of the Estabrooks questionnaire 20,21. This item generates a mode 2 network, characterised by being formed with two sets of nodes, which allows for exploring and generating the social network of use of the most common information sources related to research. Item 2, following the methodology used by Burt and Cross et al. 21,22, explores social networks of help and/or advice for knowledge transfer. It also results in a mode 2 network, which generates the network of help and/or advice for knowledge transfer. Item 7 was developed ad hoc for this study to find out the usual places where information related to research results is shared. As in the previous items, a mode 2 network is obtained to explore places where research information is shared.
Participation was facilitated by an online questionnaire, with an initial and a reminder mailing, to achieve a better response rate.
After the end of the participation period, the collected data were processed, the SNA method was applied and the graphs were created with the Pajek software to visualise the dynamics of the group of professionals 23. Each resulting network will be characterised by the inventory of nodes in each group or mode, the number of relationships between both modes and the density of the network whose measure allows us to know the proportion of relationships that occur against the number of possible relationships. In a mode 2 network, the maximum number of possible relationships results from multiplying the number of nodes in each set. The resulting value of the density is a value ranging from 0 to 1, with a value of 0 identifying a disconnected network and a value of 1 identifying a network with complete relationships 24.
RESULTS
The participation of the six units, Resuscitation, ICU, Oncology, Gynaecology, Delivery Service and Psychiatry (as control unit) amounted to 77 professionals, which means an overall participation rate of 71.96%. The socio-demographic profile shows a participation of 9 men (11.7%) and 68 women (88.3%) with a mean age of 42.9 (SD:11.48). From a professional perspective, 6 people have less than 5 years of experience (8%), between 6 and 10 years a total of 3 people (4%), between 11 and 20 years 35 participants (45%), between 21 and 30 years 23 of them (30%) and finally 10 people over 30 years (13%). 73 people (95%) were employed in care, compared to 4 professionals in management (5%).
Figure 1 is a graph in which the participants (77 nodes in grey) and the units with which they are linked (6 nodes in different colours) are grouped into clusters. In the Resuscitation unit a response rate of 97% was achieved (33 participants or nodes), in ICU the rate was 100% (8 nodes), in Oncology the rate was 70% (7 nodes), in Gynaecology the rate was 90% (9 nodes), in Delivery Service the rate was 34.8% (8 nodes) and in Psychiatry the rate was 54.5% (12 nodes).

Information sources to obtain research results
Item 1 explores the information sources that are used by participants to obtain information and/or advice on research results. The resulting network, Figure 2, is made up of two sets. In one of them, the participants (77 nodes in grey); in the other, the information sources used: peers; databases or scientific articles (DBs); clinical practice guidelines or protocols (Guidelines); Internet, social networks or websites (Internet); books; sessions, courses or congresses (Sessions) (6 nodes in red). In turn, it is also a weighted network. The weighting is the importance that each participant assigns to each source when deciding how often they use it. The different shades of grey assigned to the links reflect this weighting, the more intense the grey, the greater the frequency of use.

The relationships between the nodes included in both modes are directional, starting at the participants and ending at the sources. In this network, 424 relationships occurred; according to the frequency of use of the source (0 never, 1 rarely or not used; 2 sometimes, 3 frequently, 4 or 5 always), 38 relationships have a value equal to 0, therefore, sources never used; 88 relationships have a value of 1, then sources rarely used; and the rest, 336, have a value higher than 1, for the rest of the uses.
The network density is 0.92, a value very close to unity. This is unusual in single-mode networks, but in this network, it occurs as a consequence of being a question posed so that all participants would assign a frequency to each source.
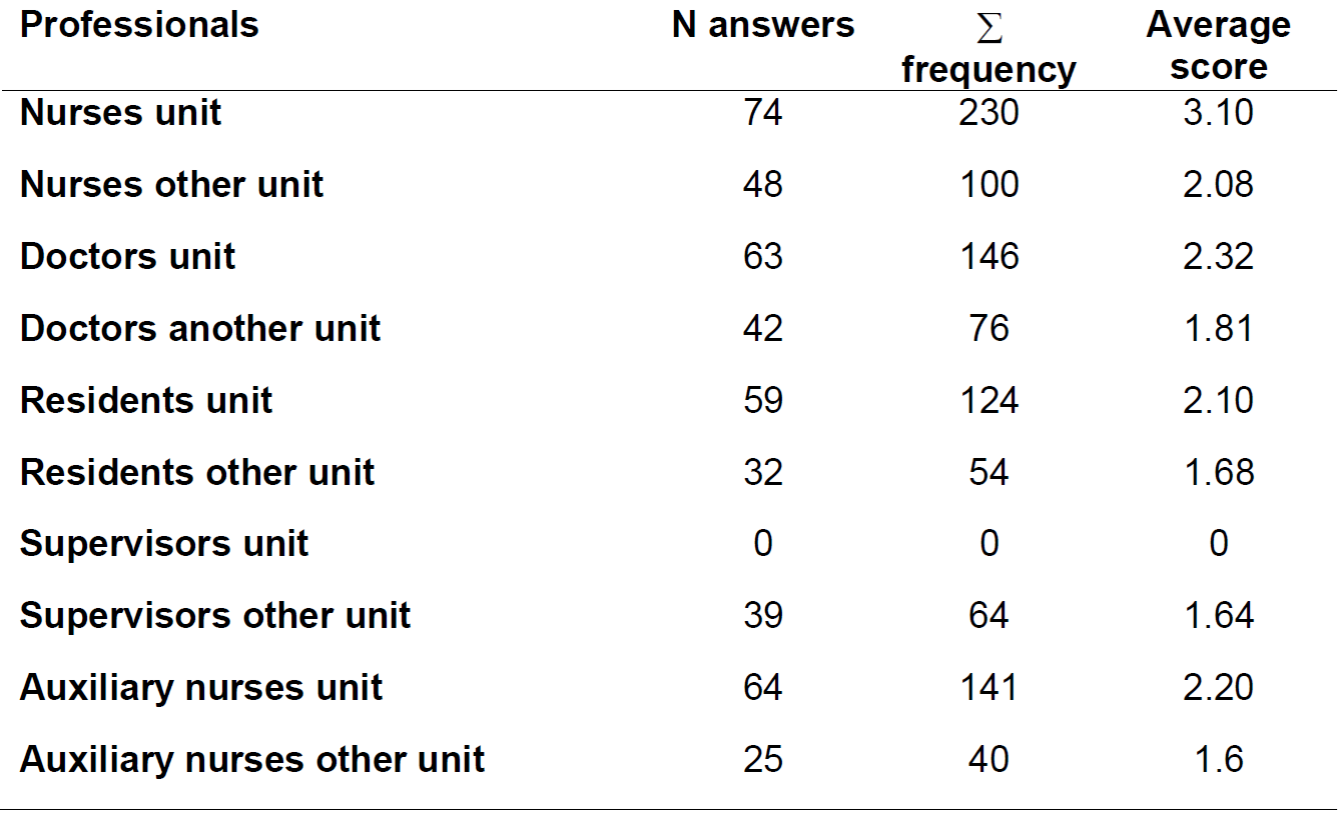
Peers was the source with the highest number of choices and the highest weighting, while the source of bibliographic databases and/or scientific articles was the least selected as a source of information. The distribution of all the sources consulted with the responses (descending order), both absolute and weighted, and the average score resulting from dividing the weighting (∑ frequency) by the number of responses, is shown in Table 1.

Considering the participants' units, in both Resuscitation and Psychiatry (control) the most used source was colleagues and the least used was databases or articles. In the rest of the units, ICU, Oncology, Delivery Service and Gynaecology, the most used sources were clinical practice guidelines or protocols and the least used were books, clinical sessions and databases or articles.
Professional groups as a source of information or for advice
Item 2 explores the groups of professionals consulted for information and/or advice on research results. This is an item where, in addition to multiple choice and its assessment, participants have the possibility of adding other units to which professionals are linked to obtain information and/or advice.
From this item we obtain the network shown in Figure 3 with its two modes, where one includes the participants (77 nodes in grey) and the second includes the professionals from whom information is obtained (10 in red). The link between the two modes is weighted and is visualised thanks to the different shades of grey assigned to the links that reflect this weighting, the greater the intensity of grey, the greater the frequency of use. The distribution of these values coincides with that expressed for item 1.
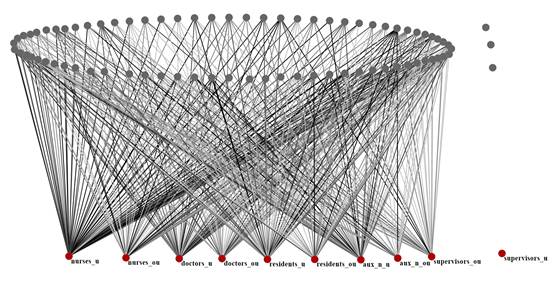
Between the two modes, 446 relationships occur, of which 146 have a value equal to 1 (which would be rarely) and the difference, 300, a value different from 1. The last group mentioned includes those responses in which the participants have not responded or those that indicate never (in both cases 0).
The density of the network is 0.58, and the value confirms that, among all the professionals, many of them were not valued on several occasions or were professionals from whom no information or advice is obtained.
Compared to them, the professionals from whom information is most frequently obtained and who are given the highest weighting are the nurses of the same unit. However, the professional never considered is the unit's supervisors (node of the second mode isolated in red). Three participants also appear isolated, grey nodes, a fact that can be interpreted as reflecting the fact that no group of professionals is a source of information for them. The distribution of all professionals consulted with both absolute and weighted responses and the average score resulting from dividing the weighting (∑ frequency) by the number of responses is shown in Table 2.
Table 2. Professionals consulted as a source of information: responses, weighted responses ( and average score
When the participants stated that other units were consulted for information and/or advice, for the profile of doctors in another unit, the Internal Medicine unit (11) was the most frequent; when it was indicated that other professionals were consulted who fit the profile of supervisors in other units, ICU supervision was the most frequent (13); when it was decided to reflect which other professionals were consulted within the profile of nurses from other units, ICU professionals were the most frequently consulted (12); when it was indicated that other professionals were consulted within the profile of auxiliary nurses from other units, again those from the ICU were the most frequent (6); when it was shown that other professionals were consulted within the profile of residents from other units, those from the delivery service were the most frequent (6).
Places where information is shared
Item 7 explores the places or settings where information related to the research results has been shared, limited to the last 12 months. For this item, participants are asked to limit their response to 3 choices in order of priority (1st, 2nd or 3rd).
From it we obtain the network included in Figure 4 with its two modes, where the one mode includes the participants (77 nodes in grey) and the second mode is the places where sharing takes place (9 in red). The use of the grey scale for the relationships in this network is not used for the intensities, as they would be expressed in the opposite direction. The first choices would be less intense and the third choices more intense. For this reason, they are all displayed with the same intensity.
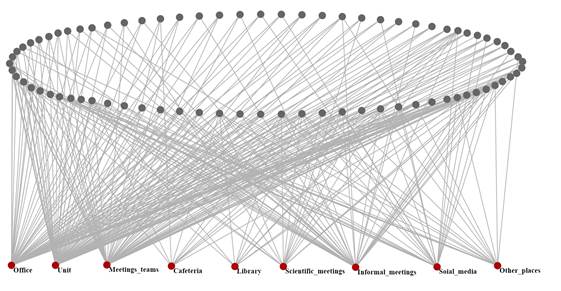
The relationships between the nodes included in both modes are directional, with the starting point at the participants, considering on this occasion that the maximum number of choices is 3 and that always as a destination, the places where information is shared are selected. There were 289 relationships, of which 105 have a value equal to 1 (first place) and 184 for second and third places.
The density of the network is 0.42, an expected value as a consequence of the wording of the question, maximum three choices out of all possible places or settings where information related to the research results has been shared. While the value should be close to 0.33 density in this network, for those three choices requested out of nine possible choices. But some participants assigned a position of 1, 2 or 3 simultaneously to more than three sources.
The unit is the most frequently reported first choice for information sharing, followed by the living room/office and thirdly by team meetings. Table 3 shows the pattern of participants' choices organised by location.

Many participants did not assign a seat to certain settings. This was the case for library (67), hospital cafeteria (67), scientific events/meetings (61), informal meetings (41), team meetings (27) and nursing office/office (20). For other places outside the hospital where information was shared, some participants also did not assign posts (61); when they were assigned, the places identified were outside the hospital or home on two occasions; specifically, cafeteria, own nutrition practice, informal meeting, midwifery teaching unit, changing room and other hospitals (La Paz). Something similar occurs with social networks (Whatsapp, Facebook) as a place to share information, which also accumulates as a place with a significant absence of post assignment (54); which is completed with which social network is used and which in descending order is Whatsapp (8), Facebook (4), Instagram (2) and Twitter (1).
DISCUSSION
Considering that the response rate of the study was 71.96%, studies with the SNA method obtained sample sizes similar to ours and a response rate between 77-90% 16,25.
Item 1, which explored the sources of knowledge used by nursing professionals to obtain information or advice on research results, showed that in the network of this item, peers were the most chosen source with the highest weighting, while the source that brings together bibliographic databases and/or scientific articles was the least selected as a source of information. This network makes visible the hegemony of tacit knowledge reflected by many authors in the literature 2,26. In other words, experiential knowledge continues to be an important source for problem solving; this coincides with authors who reflect that experience is placed as a priority information resource, being an indispensable element in the acquisition of expert nursing knowledge 27.
However, if this item is analysed considering the type of unit, other nuances emerge. Of the 6 units analysed, in 2 (Resuscitation and Psychiatry) the most frequently used source was colleagues (tacit or experiential knowledge that may or may not be based on research), but in the remaining four units (ICU, Oncology, Gynaecology and Delivery Service) they considered clinical practice guidelines and protocols to be the most common source of knowledge. This may be related to the degree of specialisation of certain units in which they work with these information sources based, in many cases, on research results. In this line, the impact of specialisation (specialists in training) and advanced practice on the development of evidence-based practice (EBP) and, therefore, on the use of research by nursing professionals is also being studied. The level of expertise implicit in these new roles is associated with greater skills in synthesising and applying research-derived information 28,29.
On the other hand, it is evident that electronic resources that allow immediate access to scientific information (databases or open access articles) continue to be an underused source. In this study, the average age of the sample is close to 43 years old, and it is likely that the lack of training related to access to electronic resources may be influencing the low choice of this source. This coincides with studies on the subject, in which the lack of knowledge and skills in the search and evaluation of published research studies is a barrier to the use of research 21,30.
Item 2 explored the groups of professionals consulted for information and/or advice on research results. Its network shows how nursing professionals in the unit itself become the main source of information and/or advice on research results. Then, homophilic (professionals with similar status and interests) and horizontal (between people with the same status) networks emerge. Previous studies indicate that nursing professionals tend to operate in vertical networks 8; this may mean a change in the importance or prestige given to knowledge from other professional Figures, such as doctors, and focus on colleagues of the same professional category 31.
Horizontal networks are more effective at diffusing peer influence and supporting both knowledge construction and reformulation; vertical networks are more effective at approving hierarchical decisions. This is reinforced by the fact that unit supervisors (professionals with different status and interests) were not, in any case, chosen as a source of information; as networks tend to be vertical and related to authority-based decisions among nurses with nurses of other status 10. However, the literature reflects that nurses in management roles report higher scores on attitudes, knowledge and skills towards EBP 32.
Adoption of scientific knowledge by individuals is more likely if they are homophilic, i.e. if they have similar socio-economic, educational, professional, and cultural backgrounds. Health professionals work within peer groups that share common values and beliefs, and individual behaviour can be strongly influenced by these elements 9.
Item 7 explored the places or settings in which information related to research results has been shared, limited to the last 12 months. The unit is the most chosen place to share information, with the second choice being the office/office and the third choice being team meetings. This shows that the work environment is the main setting for information sharing. A SNA study carried out in the context of an evidence implementation project points to team meetings as an ideal setting for information sharing, given that the overload of care in the units prevents adequate information sharing 33.
Perhaps the age of the sample may influence the lesser choice of places outside the work environment or the use of social networks to share information related to research results34.
As lines of future work, it is important to note that within the field of EBP efforts are focused on generating evidence on the effectiveness of interventions; however, the ways in which evidence interacts with clinical experience and professional networks need to be addressed 4,35. Finally, it is important to note that having a control unit in place allowed us to determine whether being part of an evidence implementation project can produce the so-called "contagion effect" described by some authors; an effect whereby the adoption of knowledge can be influenced by the structure of the network that will adopt it, and includes the characteristics of the knowledge, the actors and the context 36. It is true that the unit of control has reflected different patterns in some aspects such as the sources of knowledge used by professionals to obtain information or advice on research results, but complementary statistical approaches would be needed to analyse the effect of the variable "type of unit" on the choice of the different professionals as information sources and the places where it is shared.
CONCLUSIONS
Nursing professionals consider the experiential knowledge of their peers as the primary source for information/advice on research findings. That expertise may or may not be supported by research. These professionals create homophilic-horizontal networks, by drawing on professionals with similar status and interests, from whom they obtain information and/or advice on research findings. It should be noted that professionals in management positions within the unit are excluded as a resource for such information and/or advice.
In units with a certain degree of specialisation, nursing professionals use clinical practice guidelines and protocols as their main source of information. While databases and scientific articles remain the least used source.
The physical work environment with its different options (unit, office, or meetings) is the most widely used for sharing information on research results.
REFERENCIAS
1. Ramírez A. La teoría del conocimiento en investigación científica: una visión actual. An la Fac Med. 2009;70(3):217-24. [ Links ]
2. Pérez-Fuillerat N, Solano-Ruiz MC, Amezcua M. Conocimiento tácito: características en la práctica enfermera. Gac Sanit [Internet]. 2019;33(2):191-6. Disponible en: http://dx.doi.org/10.1016/j.gaceta.2017.11.002 [ Links ]
3. Rycroft-Malone J, Seers K, Titchen A, Harvey G, Kitson A, McCormack B. Nursing and Health Care Management and Policy. What counts as evidence in evidence-based practice? J Adv Nurs. 2004;47(1):81-90. [ Links ]
4. Nilsen P, Ståhl C, Roback K, Cairney P. Never the twain shall meet? - a comparison of implementation science and policy implementation research. Implement Sci. 2013;8(1). [ Links ]
5. Neta G, Brownson RC, Chambers DA. Opportunities for Epidemiologists in Implementation Science: A Primer. Am J Epidemiol. 2018;187(5):899-910. [ Links ]
6. Crisp N, Iro E. Comment Nursing Now campaign : raising the status of nurses. Lancet [Internet]. 2018;1-2. Disponible en: http://dx.doi.org/10.1016/S0140-6736(18)30494-X [ Links ]
7. Parchman ML, Scoglio CM, Schumm P. Understanding the implementation of evidence-based care: A structural network approach. Implement Sci [Internet]. 2011;6(1):14. Disponible en: http://www.implementationscience.com/content/6/1/14 [ Links ]
8. Lau R, Stevenson F, Ong BN, Dziedzic K, Treweek S, Eldridge S, et al. Achieving change in primary care-causes of the evidence to practice gap: Systematic reviews of reviews. Implementation Science. 2016. [ Links ]
9. Dopson S. A view from organizational studies. Nurs Res. 2007;56(4):72-7. [ Links ]
10. Everett MG, Valente TW. Bridging, brokerage and betweenness. Soc Networks [Internet]. 2016;44:202-8. Disponible en: http://dx.doi.org/10.1016/j.socnet.2015.09.001 [ Links ]
11. Arias N, Calvo MD, Benítez-Andrades JA, Álvarez MJ, Alonso-Cortés B, Benavides C. Socioeconomic status in adolescents: A study of its relationship with overweight and obesity and influence on social network conFiguration. Int J Environ Res Public Health. 2018;15(9). [ Links ]
12. Quiroga E, Pinto-Carral A, García I, Molina AJ, Fernández-Villa T, Martín V. The influence of adolescents' social networks on alcohol consumption: A descriptive study of Spanish adolescents using social network analysis. Int J Environ Res Public Health. 2018;15(9). [ Links ]
13. Xu J, Yang R, Reblin M, Clayton M, Ellington L. Using Social Network Analysis to Investigate Positive EOL Communication. J Pain Symptom Manag. 2018;56(2):273-80. [ Links ]
14. Creswick N, Westbrook JI. Who Do Hospital Physicians and Nurses Go to for Advice about Medications? A Social Network Analysis and Examination of Prescribing Error Rates. J Patient Saf. 2015;11(3):152-9. [ Links ]
15. Maya I. 7 Usos Del Análisis De Redes En La Intervención Comunitaria. Rev Hisp para el Análisis Redes Soc [Internet]. 2016;27(2):1-10. Disponible en: http://revista-redes.rediris.es [ Links ]
16. Escobar-Aguilar G, Moreno-Casbas MT, González-María E, Martínez-Gimeno ML, Sánchez-Pablo C, Orts-Cortés I. The SUMAMOS EXCELENCIA Project. J Adv Nurs. 2019;(75):1575-84. [ Links ]
17. Martínez-Gimeno ML, Ovalle Perandones MA, Marqués-Sánchez P, Escobar-Aguilar G, Fernández-Martínez N, García-García E, et al. Validez de Contenido de un cuestionario para explorar redes sociales de transferencia del conocimiento. En: XXIII Encuentro Internacional de Investigación en Cuidados. Investen-Isciii, editor. Barcelona; 2019. [ Links ]
18. Escobar Aguilar G, Martínez-Gimeno M, MedinaTorres M, Martín de Castro E, Murillo Pérez M, Blanco Abril S. Patrones de utilización de la investigación por los profesionales de enfermería de los hospitales de Madrid. NURE Inv. 2015;12(79). [ Links ]
19. Burt RS. Structural holes: The social structure of competition. 1992. [ Links ]
20. De Nooy W, Mrvar A, Batagelj V. Exploratory Social Network Analysis with Pajek: Revised and Expanded Edition for Updated Software. Third Edition. Third Edit. Cambridge University Press, editor. New York; 2018. [ Links ]
21. Merrill JA, Yoon S, Larson E, Honig J, Reame N. Using social network analysis to examine collaborative relationships among PhD and DNP students and faculty in a research-intensive university school of nursing. Nurs Outlook [Internet]. 2013;61(2):109-16. Disponible en: http://dx.doi.org/10.1016/j.outlook.2012.08.001 [ Links ]
22. Keith RE, Hopp FP, Subramanian U, Wiitala W, Lowery JC. Fidelity of implementation: development and testing of a measure. Implement Sci [Internet]. 2010;5(1):99. Disponible en: http://www.implementationscience.com/content/5/1/99 [ Links ]
23. Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organizations: Systematic review and recommendations. Vol. 82, Milbank Quarterly. 2004. p. 581-629. [ Links ]
24. Muñoz Jiménez D. From evidence-based nursing to healthcare practice: The evaluation of results as an integrating element. Enferm Clin. 2018;28(3):149-53. [ Links ]
25. Guadarrama-Ortega D. Barriers to the utilisation of research . Descriptive study performed on nurses at a hospital in the southwest of Madrid. Enferm Glob. 2016;(43):275-88. [ Links ]
26. Bond MO, Gaoue OG. Prestige and homophily predict network structure for social learning of medicinal plant knowledge. PLoS One [Internet]. 2020;15(10 October):1-27. Disponible en: http://dx.doi.org/10.1371/journal.pone.0239345 [ Links ]
27. Ruzafa-Martínez M, López-Iborra L, Armero Barranco D, Ramos-Morcillo AJ. Effectiveness of an evidence-based practice (EBP) course on the EBP competence of undergraduate nursing students: A quasi-experimental study. Nurse Educ Today [Internet]. 2015;38:82-7. Disponible en: http://dx.doi.org/10.1016/j.nedt.2015.12.012 [ Links ]
28. Yousefi Nooraie R, Lohfeld L, Marin A, Hanneman R, Dobbins M. Informing the implementation of evidence-informed decision making interventions using a social network analysis perspective; a mixed-methods study. BMC Health Serv Res. 2017;17(1):1-14. [ Links ]
29. IAB SPAIN. Radiografía del usuario de Redes Sociales Español (estudio IAB Spain). 2017. [ Links ]
30. Fitzgerald L, Harvey G. Translational networks in healthcare? Evidence on the design and initiation of organizational networks for knowledge mobilization. Soc Sci Med [Internet]. 2015;138:192-200. Disponible en: http://dx.doi.org/10.1016/j.socscimed.2015.06.015 [ Links ]
Received: February 26, 2021; Accepted: March 03, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
