










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkEnfermería Global
versão On-line ISSN 1695-6141
Enferm. glob. vol.20 no.64 Murcia Out. 2021 Epub 25-Out-2021
https://dx.doi.org/10.6018/eglobal.472321
Originals
Attitude and self-care practice in hansen's disease: construction and psychometric validation of measuring instruments
1 . Enfermera, Doctora en Enfermería, Profesora de las Facultades Nova Esperança , João Pessoa, Paraíba, Brasil. karenbrito.enf@gmail.com
2. Enfermera, Doctoranda em Enfermería, Universidad Federal da Paraíba , João Pessoa, Paraíba, Brasil.
3. Fisioterapia, Doctora en Enfermería, Profesora de las Facultades Nova Esperança , João Pessoa, Paraíba, Brasil.
4. Enfermera, Doctora en Enfermería, docente del curso de graduación en Enfermería de la Universidad Federal da Paraíba . Brasil.
Objective:
To build and test the content validity of the instrument, attitude, and practice of self-care in leprosy, with face, hands, and feet.
Method:
Methodological study of technology validation and quantitative approach. An instrument called Attitude and Practice of Self-Care in Hansen's Disease was developed, containing two constructs, three dimensions and 45 items. The validation used analysis through the evaluation of the internal consistency of each item / dimension and the Kappa inter-observer agreement index.
Results:
The validity index indicated the need for adjustments to the original composition of the scale, which now consists of 45 questions to 52, with the inclusion of a fourth dimension, showing high inter-agreement observers in the second version (K≥0.99).
Conclusion:
The scale has adequate psychometric properties, revealing potential for use in future studies.
Key words: Validation studies; Nursing; Hansen's disease
INTRODUCTION
Hansen's disease is recognized as an endemic disease with serious consequences for public health at global, national, and regional levels. Data from the World Health Organization (WHO) show an accentuated picture of the endemic in three countries, among which Brazil ranks second in the diagnosis of new cases1.
Additionally, the gap between the globally recommended targets and the detection coefficients found for Brazil, between the years 2013 - 2018, a total of 586,112 new cases of the disease were recorded with an increase in the number of relapse cases and active presence of the endemic, evidenced by the indicator of cases in children under 15 years old. Data from 2019 show that Brazil diagnosed 23,612 new cases of Hansen's disease, of which 1,319 (5.6%) were in children under 15 years old. Of those 39.3% already presenting some degree of physical disability (GIF 1 or GIF 2) already at the time of diagnosis 2)(3)(4.
Reflexively, the epidemiological picture has repercussions on health services at the three levels of the health care network - primary, secondary, and tertiary. Although it presents feasible diagnosis, free treatment and systematic monitoring recommended by the Ministry of Health (MH), intrinsic factors, such as the immunopathological response developed by the body against the disease and extrinsic factors, such as late diagnosis and inadequate assistance, hinder early actions, which culminate in the installation of injuries, disabilities, and physical deformities 5.
Considering the morbidity of the disease, Hansen's disease is the leading cause of permanent physical disability among infectious diseases. The risk of developing disabilities and deformities increases when multidrug therapy is started late and associated with inadequate clinical follow-up in the health services 6.
Among the difficulties in facing the disease and caring for individuals, there is the evidence that social inequality is directly related to increased susceptibility to Hansen's disease, since it produces unmet social needs that affect community health. In this context, the territorial extension of Brazil presents social heterogeneities among the regions and, therefore, specific needs among the services and, in these, among the users7. The historical and self-reported stigma factor is also added.
It is understood, therefore, that caring for individuals affected by Hansen's disease involves prioritizing strategies that fit into their psychosocial, cognitive, and pathological reality. Thus, self-care activities must be performed giving priority to what can be done at the patient's home, giving veracity and concreteness to the continuity of treatment in the patient's environment.
Under this prism, although there are recommended measures, the commitment to early case detection, contact assessment, evaluation of the degree of disability at diagnosis and follow-up every three months during treatment, health education and guidance on self-care measures, it is essential to evaluate the specific needs of individuals, as well as the development of coordinated services for the identification of inequalities and the most effective use of health resources8.
Based on the assumption that, in their individuality, people have different degrees of knowledge and adopt attitudes and practices that are often cognitively incoherent, there is a need for technologies that enable the knowledge of the behavior directed, or not, to self-care, that guide which actions should be guided, and that allow the monitoring and evolution of these individuals, as a tool for care.
Regarding the evaluation of self-care practices in Hansen's disease, although there is a reference to a study that addresses the subject through its research instrument 9, it was not found, in the main national databases, a study that addresses the existence of a validated instrument specifically for this purpose (evaluation of attitude and self-care practices in Hansen's disease).
Consequently, the justification for this study is based on the absence of valid instruments to measure attitude and practice of self-care in Hansen's disease. Thus, the construction and validation of a tool that serves this purpose may contribute to the organization of services and to the quality of care, as it enables health professionals to develop comprehensive care strategies and transform clinical practice.
Given the above, this study aimed to construct and test the content validity of the instrument "attitude and practice of self-care in Hansen's disease, with face, hands and feet".
MATERIAL AND METHOD
This is a technology construction and validation study, of the methodological development research type with a quantitative approach. It was carried out in João Pessoa/Paraíba/Brazil.
To construct the instrument named Attitude and Self-Care Practice in Leprosy - APAHansen, we first delimited the definitions of the constructs of interest: attitude and practice.
According to the theorist Everett Rogers10, the attitude and practice constructs are closely related, whereas they define attitude as the individual's values and beliefs about something, determining his actions, which assumes the condition of the practice construct, towards them influencing positively or negatively in the decision making for accepting them.
In a complementary way, attitude relates to the affective domain - emotional dimension, while practice is the decision making for doing and relates to the psychomotor affective and cognitive domain - social dimension11.
The process of construction and content validation of the instrument called Attitude and Self-Care Practice in Hansen's disease - APAHansen followed the theoretical framework of the author Raymundo12, which presents three consistent stages (each stage in turn addresses three phases) for scale validation: error collection, initial instruments, and final instruments. In this study, the three phases that make up the first stage of the process explained by the author12 were performed, namely: generation of items; analysis of redundancy added to the composition; content validation.
The first validation phase "Generation of items" covered the literature search for the formulation of items on self-care measures in Hansen's disease. We chose to develop the items of the form according to the practices recommended by the Ministry of Health guide for face, hands, and feet 13. This reference systematically approaches self-care measures directed to the three dimensions. It covers hydration and lubrication guidelines, correct nail cutting, type of shoe, care when exposed to the sun or to work routines, muscle strengthening exercises, among others.
Based on these propositions, the errors were grouped according to the similarity of the items and the consequent composition of the instrument. Thus, the two constructs - attitude and practice - were broken down into 45 items, being 3 attitudinal items and 42 practical items. The latter was subdivided into three dimensions - face, hands, and feet. They were also arranged in positive and negative affirmative sentences, under the same response scale (totally disagree, disagree, do not know, agree, totally agree).
In the second phase "Compositional Aggregate Redundancy Analysis" the items were formulated as statements, grouped according to construct similarity, and stated on a Likert scale format.
The Likert scale format was chosen because it allows a construct to be developed through statements about which respondents express their degree of agreement14. To avoid the order effect and the acquiescence effect, we chose to keep the positive items on the right and the negative items on the left, as well as to insert negative items into the instrument, compensating for both effects11
Then, in the third phase "Content Validation", the instrument was sent to a panel of judges with renowned theoretical and practical experience in the subject. This process took place between October and December 2016. The selection criteria used were health professionals with at least a master's degree, at least 5 years of experience in the area, and authorship of at least two scientific articles on the subject in the last five years.
The strategy for search and selection of judges was obtained through the Lattes Platform of the National Council for Scientific and Technological Development (CNPq), using the Hansen's disease filter. Under the inclusion criteria, 54 professionals were contacted, of which only 11 responded positively to the request for evaluation of the instrument. As the quantity was in accordance with Pasquali's definitions15, which defines as ideal a sample of 6 to 10 evaluators, without the need of sample calculation related to statistical inferences, we proceeded with this sample quantity.
Operationally, each item of the instrument was evaluated by the judges according to its clarity (they are understandable, without ambiguities and with easy expressions, with coherence between the questions) and relevance (they are important and consistent with the attribute of measuring the attitude and practice of the subjects) within the dimensions and respective constructs. The answers were graded between agree, partially agree, and disagree, with room for suggested reformulations. After evaluating the items present in the instrument, there was one more question about the need for inclusion of a new item, about which the judges should give their opinion and discuss.
To analyze the data obtained by the content validation strategy, the Content Validity Index (CVI) was used. In this measure, the instrument was considered valid if, when computing the evaluations, it obtained an approval/agreement index above 80% (0.8)16. For items with CVI below this value, there was exclusion or reformulation, according to the judges' suggestion.
After all corrections and suggestions were made, the instrument was sent again to the 11 specialists who participated in the first moment of evaluation. The criteria for theoretical analysis and validation of the items were the same as previously adopted. After reviewing the evaluation criteria to finalize the process, the accepTable agreement rate among the judges was increased to 0.9017.
For data analysis, at the time of reevaluation, it was decided to perform an interobserver assessment, to measure the intensity of agreement between the judges, through the Kappa index (K). In this way, only the experts who judged the instrument in both moments were considered. The judges had 30 days to respond, since they were already familiar with the research proposal. However, only 08 experts sent their considerations within the deadline. Thus, the "K" index was measured for this sample, accepTable to the parameters adopted at the beginning of the process 15.
For the "K" measure, the following interpretation was considered: <0 - no agreement; 0 to 0.19 - poor; 0.20 to 0.39 - reasonable; 0.40 to 0.59 - moderate; 0.60 to 0.79 - substantial; and 0.80 to 1.00 - excellent/approximately perfect18. Corroborating with another author17, values ≥ 0.90 represent excellent/approximately perfect agreement. Thus, this was the parameter adopted. The study was approved by the Ethics Committee of the Universidade Federal da Paraíba of the Health Sciences Center (UFPB/CCS) through an addendum to a larger project developed in the research group (Opinion No. 0785/2016). The professionals involved signed the Informed Consent Form and the participants' anonymity was respected.
RESULTS
To build the instrument of attitude and practice of self-care in Hansen's disease, we first delimited the definitions of the constructs of interest: attitude and practice, having as reference the conceptions of the theorist Everett Rogers10.
In a complementary way, attitude relates to the affective domain - emotional dimension, while practice is the decision making for doing and relates to the psychomotor affective and cognitive domain - social dimension19.
In view of the constructs, the instrument's starting point for its construction was the 1st step "Generation of items" of the instrument. Its construction was based on the guidelines for self-care with face, hands and feet expressed in the technical manual of the Brazilian Ministry of Health13. This reference systematically addresses self-care measures directed to the three dimensions. It covers hydration and lubrication guidelines, correct nail cutting, type of shoe, care when exposed to the sun or to work routines, muscle strengthening exercises, among others.
Based on these propositions, the second step was to group the errors according to the similarity of the items and the consequent composition of the instrument. Thus, the two constructs - attitude and practice - were broken down into 45 items, being 3 attitudinal items and 42 practical items. The latter was subdivided into three dimensions - face, hands, and feet. They were also arranged in positive and negative affirmative sentences, under the same response scale (totally disagree, disagree, don't know, agree, totally agree). Finally, the instrument was named: Attitude and self-care practice in Hansen's disease: face, hands, and feet - APAHansen.
In the third phase, the items of the instrument were submitted to analysis of representativeness, content validation, by a committee composed of 8 judges, five nurses, one anthropologist, one physician, and one occupational therapist. This committee was 100% female (100%), over 50 years old (62.5%), with more than 20 years of experience in the field (75%). Among the judges, 62.5% had a doctoral degree, 25% a post-doctoral degree, and one a master's degree. All presented themselves as experts for the evaluation of the construct, evidenced by meeting the selection criteria.
Regarding the specialists' judgment about the clarity and relevance of the items in the preliminary version of the instrument, none of them was evaluated as disagreeing/inadequate. All items obtained agreement within the established level (CVI ≥ 0.80) concerning relevance. Only items A, B, C (attitude construct) and 1.9 (practice construct) showed CVI ≤ 0.75 regarding clarity, indicating the need for reformulation.
The overall CVI of the instrument was 0.91 for clarity and 0.96 for relevance of the items, showing satisfactory content validity. The item-by-item results are presented in Table 1.
Table 1. Content validity index of the scale obtained through the judges' assessment of the adequacy of the constructs to the psychometric criteria: clarity and relevance (n=8). João Pessoa, Paraíba, Brazil, 2017.

Legend: Items A to C - refer to the ATTITUDE construct; Items 1.1 to 3.20 - refer to the PRACTICE construct.
Source: Research Data, 2017.
As seen in Table 1, of the total 45 items, 20 showed a perfect agreement index (CVI = 1.00) for clarity and 32 for relevance. The items of the Attitude construct were the ones that presented the greatest need for adjustments. Although only 4 items of the instrument presented CVI below the established standard (CVI < 0.80), the suggestions for adaptation were accepted, also for those items that did not get perfect agreement, since they were very relevant to reach a better understanding of the instrument. The exception to the adjustments were the items with negative statements (2.7, 2.8, 3.9, 3.11, and 3.14).
The attitudinal items were scored as less clear (CVI≤ 0.75), and the suggestions to divide them between questions about observation and care (Is it necessary to observe the face daily? / Is it necessary to care for the eyes and nose daily?) were considered. A similar direction was adopted regarding practical item 1.9 (Do you wear a hat/bonnet and sunglasses when exposed to the sun) (Table 1).
In Chart 1, the items evaluated as "partially agree/with changes", the requirements related to the problem and the suggestions for improvement or reformulation are presented.
Chart 1. Suggestion of the judges about the items considered adequate with changes. João Pessoa, Paraíba, Brazil, 2017.

Source: Research Data, 2017.
In addition to the adjustments postulated above, the inclusion of two items to the Practice Construct ("Wear’s eye protection [mask] when sleeping" and "Cuts his nails in a straight shape"); change in the scaling of the instrument through temporal adverbs; and a third construct: limitations for self-care were recommended.
The alternative answers were considered a distorting factor to understanding, because they make it difficult to make a judgment. As for the scale of answers, the number of options was kept at five, but adjustments were made to the options: 1 "Never"; 2 "1 to 2 times a week"; 3 "Don't know"; 4 "3 to 6 times a week"; 5 "Always".
The third construct - "limitations to self-care" - was postulated through a question at the end of the instrument, with a dichotomous answer, for which a second question is asked - which ones? - when the answer is positive - "yes".
These suggestions served as a basis for adapting the initially proposed instrument, which contained 45 items in its primary version, to 52 items, which was then submitted to a second evaluation by the judges.
Regarding the judges' considerations to the "relevance" requirement, it is observed that the disagreements occurred on the negative questions. However, these suggestions were not incorporated, since the inclusion of this statement format is a strategy used in scale development, and the CVI remained above the proposal (CVI ≥ 0.80).
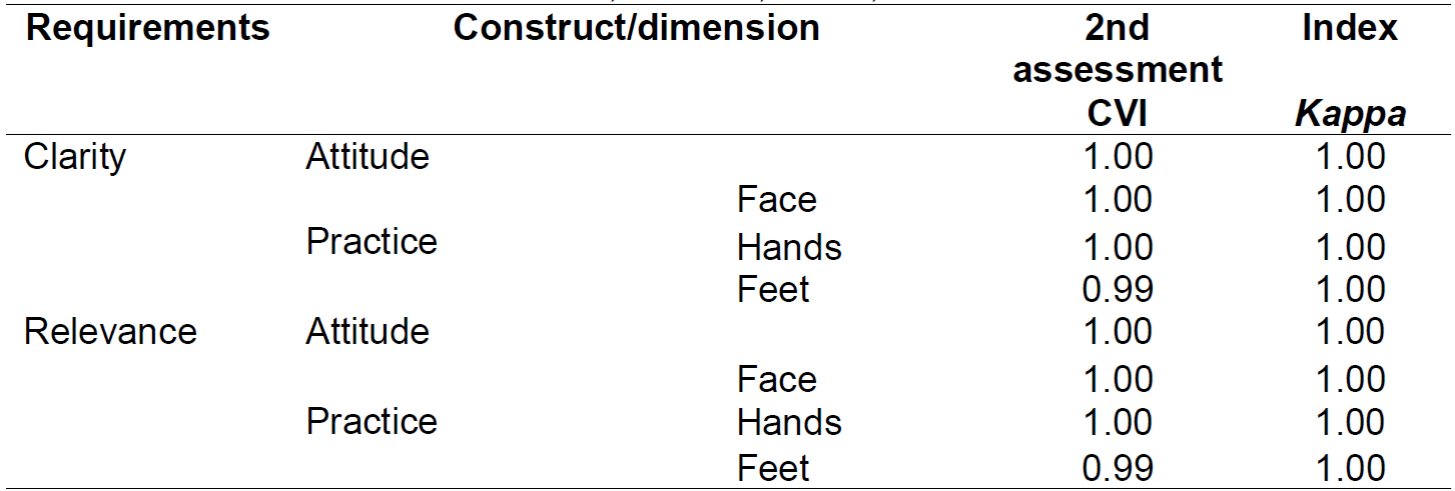
In the judges' final opinion, based on the requirements of clarity and relevance, all items obtained a CVI between excellent and perfect. In this step, besides this measure, Kappa index was also calculated between the two evaluations performed by each judge, showing perfect classification, or total agreement, for both constructs in the face, hands, and feet dimensions, as shown in Table 2.
DISCUSSION
The construction of a measurement instrument requires preparation of items that will represent the behavior through the construct of interest20. However, it is essential that these instruments have reliability and validity to minimize the possibility of subjective judgments12. Thus, the recognition of the quality of the instruments becomes a fundamental aspect for the legitimacy and credibility of the research results, which reinforces the importance of the validation process21).
Nesse sentindo tem sido frequente a realização desses processos por pesquisas em enfermagem 21)(22)(23, no entanto, não foi evidenciado pelas pesquisadoras desta pesquisa, artigos que com perspectiva similar a apresentada relacionada a atitude e prática de autocuidado na hanseníase. In this sense, it has been frequenting the accomplishment of these processes by nursing research 21)(22)(23, however, it was not evidenced by the researchers of this research, articles with similar perspective to the one presented related to attitude and practice of self-care in Hansen's disease.
The choice of Raymundo's conceptual model12 and the content analysis technique allowed us to identify and arrange relevant topics to cover the constructs (attitude and practice) and dimensions of self-care with face, hands, and feet in Hansen's disease.
Regarding the two constructs listed for the composition of the instrument, it is worth mentioning that they were arranged together in the same assessment, because attitudes and self-care practices are complex axes of the same adherence process. In general, the instrument assumes that the attitude directs the practice, being the one related to values and/or beliefs that influence decision making, a conjecture pointed out by other studies on the subject 24,25).
Thus, the three items A/B/C (which, after the first assessment by the judges, became six) were arranged with the objective of identifying attitudes, which determine actions influencing positively or negatively the decision to adhere to the practice, identified through items 1.1 to 3.2010. The judges' considerations about these items consisted in differentiating the issues between observation and care.
The action of observing refers to considering something with attention, while the action of caring is related to the effort of dedicating time (to something) with a certain objective. In this sense, the changes improve the instrument and make it more convergent with the objectives it proposes.
Some items of the construct practice (2.7; 2.8; 3.9; 3.11; 3.14), although reaching CVI ≥ 0.80, received suggestions for reformulation due to their low relevance. It is understood that these are considered practices that should be avoided, as they have great potential to worsen the deformities and physical disabilities of individuals affected by Hansen's disease. In this way, describing them in a positive way would imply in the inversion of the answer scale, a characteristic that is not recommended by the pertinent literature11 because it may cause confusion among the respondents. Thus, the response scales should clearly present a direction continuum.
The change in the response scale (from an agreement scale to a time scale) in the practice construct seems to contribute to clarify the meaning of self-care actions, since it is defined as "procedures, techniques and exercises that the patient himself, duly guided, can regularly perform (emphasis added) at home and in other environments"25)(26)(27.
A study by Galan and collaborators on the evaluation of self-care practices in Hansen's disease, points out that not everyone can adequately practice self-care, showing difficulties in incorporating this activity as a daily life practice. This finding24, corroborates and justifies the request of the experts.
The practices for self-care are routine, however, performing them sporadically does not make them relevant to the problem of Hansen's disease. In this sense, the individual needs to understand what exactly each action consists of, why it is important for his or her condition specifically, and what possibilities for improvement can be achieved from his or her commitment. They must also be easy to apply and feasible in relation to their motor and financial conditions.
What is observed in the practice of care are "people" on the margins of ready-made orientations, when in the transversality of professional responsibility, the integrality of the subject being cared for should exist.
Concerning the incorporation of instruments adapted for the routine self-care practices of people with Hansen's disease, the research by Maia and collaborators28 revealed relevant contributions to the care of this clientele concerning feelings, perceptions, and significant contents about the social, family, and individual dimensions and the stigma associated to Hansen's disease.
Cavalcante and collaborators29 emphasize in a review about health technologies for the promotion of self-care in leprosy patients, that these are understood as a set of resources developed based on scientific knowledge and real experiences, therefore acting as a transformer of health conditions and re-signifying care practices.
Still on the judges' suggestions regarding the inclusion of the construct "limitations for self-care", this was added to the instrument, since the scientific literature cites a diversity of factors that hinder or limit self-care24 , thus, the factors that make it difficult to cope with the disease affect self-care and, therefore, should be identified by the health team, which, knowing these coefficients, better directs the individual's care30,31.
In view of the above, the psychometric validity of the instrument is substantiated as to the evaluation of its content, that is, the representativeness of the items in relation to the content areas and the relevance of the objectives to be measured14.
Some difficulties were encountered in this study, among which were the small number of specialists who responded positively to the participation request and the high time (over 60 days) for returning the evaluations.
CONCLUSION
The Hansen's disease process, although potentially known in the scientific community, shelters investigative nuances that border the universe, among other points, of adherence to self-care practices. From this point of view, the development of technologies, strategies and permissive means to its understanding and stakeholders in the care process, culminate as facilitators in the evolution of the quality of care.
Based on this need to expand knowledge, the proposal of an instrument that enables the knowledge of previous practices of individuals, that elucidates the failures of these practices, and that operationalizes the systematization of adherence to self-care practices is not only pertinent but also significant.
The results indicated satisfactory content validity, with the total set of items showing CVI's of categories between great and perfect, while the Kappa index showed full agreement for permanence in the instrument.
The choice of the conceptual model allowed us to identify and arrange relevant topics to cover the constructs (attitude and practice) and dimensions of face, hand, and foot self-care in Hansen's disease.
We conclude, therefore, that the technology instrument "Attitude and Self-Care Practice in Hansen's disease: face, hands and feet - APAHansen", validated in this study, presents psychometric characteristics (clarity and relevance), that is, it is compatible with its proposed purpose, that is, to measure the attitude and practice of self-care in Hansen's disease.
It is understood that the process of instrument validation is complex and involves different stages and forms; therefore, the performance of content validity only presents itself as a limitation of this research, although, it should be said, it corresponded to the listed objectives.
REFERENCIAS
1. Ministério da Saúde (Br). Boletim Epidemiológico. Caracterização da situação epidemiológica da hanseníase e diferenças por sexo, Brasil, 2012-2016. Brasília: DF; 2018. Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/saude_brasil_2018_analise_situacao_saude_doencas_agravos_cronicos_desafios_perspectivas.pdf [ Links ]
2. World Health Organization. Neglected tropical diseases. Leprosy: world focused on ending transmission among children. Geneva; 2018. [ Links ]
3. Ministério da Saúde (Br). Departamento de Informática do SUS [Internet]; 2019. [ Links ]
4. Ministério da Saúde (Br). Boletim Epidemiológico Especial. Hanseníase 2020. Brasília: DF; 2020. Disponível em: http://www.aids.gov.br/pt-br/pub/2020/boletim-epidemiologico-de-hanseniase-2020 [ Links ]
5. Neves TV, Valentim IM, Vasconcelos KB, Rocha ESD, Nobre MSRS, Castro JGD. Perfil de pacientes com incapacidades físicas por hanseníase tratados na cidade de Palmas-Tocantins. Revista Eletrônica Gestão & Saúde. 2016; 4(2). doi: 10.18673/gs.v4i2.22936. Disponível em: https://www.researchgate.net/publication/317407465_Perfil_de_pacientes_com_incapacidades_fisicas_por_hanseniase_tratados_na_cidade_de_Palmas-Tocantins [ Links ]
6. Moura EGS, Araújo APM, Silva MCR, Cardoso BA, Holanda MCS, Conceição AO, et al. Relação entre a Classificação Internacional de Funcionalidade, Incapacidade e Saúde (CIF) e a limitação de atividades e restrição à participação de indivíduos com hanseníase. Cad. Saúde Colet. 2017; 25 (3):355-361. Disponível em: https://www.scielo.br/scielo.php?pid=S1414-462X2017000300355&script=sci_abstract&tlng=pt [ Links ]
7. Leano HAM, Araújo KMFA, Rodrigues RN, Bueno IC, Lana FCF. Indicadores relacionados a incapacidade física e diagnóstico de hanseníase. Rev Rene. 2017; 18 (6): 832-9. Disponível em: http://www.repositorio.ufc.br/handle/riufc/28823 [ Links ]
8. Guthi VR, Sreedevi A. Health care needs of persons affected by leprosy in Kurnool division of Kurnool district. Int J Community Med Public Health. 2017; 4(7): 2474-81. Disponível em: https://www.researchgate.net/publication/328530157_Health_care_needs_of_persons_affected_by_leprosy_in_Kurnool_division_of_Kurnool_district [ Links ]
9. Ventin LMC, Ribeiro BF, Moura dos SDC, Delmondes NR, Pires DSS. Práticas de autocuidado em hanseníase: face, mãos e pés. Rev. Gaúcha Enferm. 2018; 39: e20180045. Disponível em: https://www.researchgate.net/publication/328418428_Praticas_de_autocuidado_em_hanseniase_face_maos_e_pes [ Links ]
10. Rogers EM. Diffusion of Innovations. 5th ed. Free Press; 2003. [ Links ]
11. Dalmoro M, Vieira KM. Dilemas na construção de escalas Tipo Likert: o número de itens e a disposição influenciam nos resultados? Rev Gestão Org. 2013; 6(3). Disponível em: http://www.spell.org.br/documentos/ver/31731/dilemas-na-construcao-de-escalas-tipo-likert--o--- [ Links ]
12. Raymundo VP. Construção e validação de instrumentos: um desafio para a psicolinguística. Letras de Hoje. 2009; 44(3): 86-93. Disponível em: https://revistaseletronicas.pucrs.br/ojs/index.php/fale/article/view/5768 [ Links ]
13. Ministério da Saúde (Br). Departamento de Vigilância Epidemiológica. Autocuidado em Hanseníase, Face, Mãos e Pés. Brasília: DF; 2010. Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/autocuidado_hanseniase_face_maos_pes.pdf [ Links ]
14. Costa FJ, Orsini ACR, Carneiro JS. Variações de Mensuração por Tipos de Escalas de Verificação: Uma Análise do Construto de Satisfação Discente. 2018. Revista Gestão.Org; 16 (2): 132-144. Disponível em: https://periodicos.ufpe.br/revistas/gestaoorg/article/view/69704 [ Links ]
15. Pasquali L. Instrumentação psicológicas: fundamentos e prática. Porto Alegre: Artmed; 2010. [ Links ]
16. Rubio DM, Ber-Weger M, Tebb SS, Lee ES, Rauch S. Objectifying content validity: conducting a content validity study in social work research. Soc Work Res. 2003; 27(2): 94-111.Disponível em: https://academic.oup.com/swr/article-abstract/27/2/94/1659075?redirectedFrom=PDF [ Links ]
17. Coluci MZO, Alexandre NMC, Milane D. Construção de instrumentos de medida na área da saúde. Ciênc. Saúde Colet. 2015; 20(3):925-36. Disponível em: https://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232015000300925 [ Links ]
18. Landis JR, Koch GG. The measurement of observer agrément for categorical data. Biometrics. 1977; 33: 159-174. Disponível em: https://www.jstor.org/sTable/2529310?seq=1 [ Links ]
19. Marinho LAB, Costa MSG, Cecatti JG, Osis MJD. Conhecimento, atitude e prática do auto-exame das mamas em centros de saúde. Rev. Saúde Pública. 2003; 37 (5): 576-82. Disponível em: https://www.scielo.br/scielo.php?pid=S003489102003000500005&script=sci_abstract&tlng=pt [ Links ]
20. Souza AC, Alexandre NMC, Guirardello EB. Psychometric properties in instruments evaluation of reliability and validity. Epidemiol. Serv. Saude, Brasília. 2017; 26(3):649-59. Disponível em: https://www.scielo.br/scielo.php?pid=S223796222017000300649&script=sci_abstract [ Links ]
21. Lanza FM, Vieira NF, Oliveira, MMC, Lana FCF. Validação do instrumento de avaliação do desempenho da atenção primária nas ações de controle da hanseníase (PCAT-hanseníase): versão profissionais. HU Revista. 2018; v. (44)3:311-323. [ Links ]
22. Soares JEF, Soares NLS, Freitas BHBM, Bortolini J. Validação de instrumento para avaliação do conhecimento de adolescentes sobre hanseníase. Acta Paulista de Enfermagem.2018; 31 (5): 480-488. [ Links ]
23. Zanin LE,Melo DH, Carneiro SM, Gomes JM,Pinto VPT, Wilner LWB, Santos IR, Rodrigues AKM. Proposta e validação de um protocolo de triagem para identificar as manifestações fonoaudiológicas na hanseníase. Revista Brasileira em Promoção da Saúde.2016; 29(4):564-573. [ Links ]
24. Galan NGA, Beluci ML, Marciano LHSC, Ruiz RBP, Oliveira NGG, Bonini AG, Arakaki FR, Guimarães GS. Avaliação da prática do autocuidado domiciliar em hanseníase. Hansen Int. 2016; 41 (1-2):37-45. Disponível em: https://pesquisa.bvsalud.org/portal/resource/pt/biblio-972894 [ Links ]
25. Lima MCV, Barbosa FR, Santos DCM, Nascimento RD, D'Azevedo SSP. Práticas de autocuidado em hanseníase: face, mãos e pés. Rev Gaúcha Enferm. 2018;39:e20180045. Disponível em: https://www.researchgate.net/publication/328418428_Praticas_de_autocuidado_em_hanseniase_face_maos_e_pes [ Links ]
26. Ministério da Saúde (Br). Secretaria de Vigilância em Saúde. Diretrizes para vigilância, atenção e eliminação da hanseníase como problema de saúde pública. Brasília: DF; 2016. Disponível em: https://portalarquivos2.saude.gov.br/images/pdf/2016/fevereiro/04/diretrizes-eliminacao-hanseniase-4fev16-web.pdf [ Links ]
27. Carvalho PS, Brito KKG, Santana EMF, Lima SM, Andrade SSC, Nóbrega MM, Soares MJGO. Autocuidado em hanseníase: comportamento de usuários atendidos na rede de atenção primária à saúde. Enferm Bras. 2019;18(3):398-405. [ Links ]
28. Maia FB, Teixeira ER, Silva GV, Gomes MK. The use of assistive technology to promote care of the self and social inclusion in patients with sequels of leprosy. PLoS Negl Trop Dis. 2016;10(4);e0004644. [ Links ]
29. Cavalcante NMC, Cunha AMS, Lima ABA, Tavares CM. Desenvolvimento das ações de um grupo de autocuidado em hanseníase como ferramenta de promoção da saúde. Rev. APS. 2019; 22 (2): 468 - 478. [ Links ]
30. Shayeghian Z, Hassanabadi H, Aguilar-Vafaie ME, Amiri P, Besharat MA. A Randomized Controlled Trial of Acceptance and Commitment Therapy for Type 2 Diabetes Management: The Moderating Role of Coping Styles. PLoS ONE. 2016;11(12):1-14. [ Links ]
31. Mendonça SCB, Zanetti ML, Sawada NO, Barreto IDC, Andrade JS, Miyar LO. Construction and validation of the Selfcare Assessment Instrument for patients with type 2 diabetes mellitus. Rev. Latino-Am. Enfermagem. 2017; 25:e2890. [ Links ]
Received: March 10, 2021; Accepted: July 10, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
