










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkEnfermería Global
versão On-line ISSN 1695-6141
Enferm. glob. vol.21 no.65 Murcia Jan. 2022 Epub 28-Mar-2022
https://dx.doi.org/10.6018/eglobal.482911
Originals
Uncertainty expression in surgical patients of organ removal: a cross-sectional study
1 Máster en Enfermería. Doctoranda del Programa de Posgraduación en Enfermería de la Universidad de Brasilia (UnB). Brasil. Campus Universitario Darcy Ribeiro, Facultad de Ciencias de la Salud, Brasilia-Distrito Federal Brasil. thaismmgomes@gmail.com
2 Doctora en Enfermería. Docente del Programa de Posgraduación en Enfermería de la Universidad de Brasilia (UnB). Brasil. Campus Universitario Darcy Ribeiro, Facultad de Ciencias de la Salud, Brasilia-Distrito Federal Brasil.
Introduction:
The surgical treatment of organ removal seems to meet a number of pathologies that emerge as health needs of populations. In this context, the state of uncertainty is installed.
Method:
Cross-sectional study developed with patients admitted to the surgical outpatient clinic of a university hospital. Sociodemographic and clinical variables were collected, in addition to applying Mishel uncertainty in illness scale.
Results:
The profile of medical diagnoses in the 60 participants showed that the most frequent diseases were the neoplasms. As for the scale application, 68% of the participants presented scores greater than or equal to 80 points. The value found for the Cronbach’s Alpha was 0.842. The surgical procedures abdominal hysterectomy and mastectomy, which were the most prevalent for the participants, are associated with uncertainty domains.
Conclusions:
High levels of uncertainty demonstrated the need for the management of this condition. The psychosocial aspects of surgical treatments are disregarded at the expense of the clinical restoration, circumstances that neglect the patient’s emotional suffering. The improvement of communication between the health professional and the patient can influence to prevent the manifestation of the lack of information, one of the forms of expressing uncertainty. Aspects such as the patient’s socioeconomic profile, educational level and income must be taken into account in the surgical treatment of organ removal. The uncertainty experienced by these patients needs to be better known and widely disseminated to gain prominence in the health care setting.
Keywords: Uncertainty; Surgery; Surgical Procedures, Operative; Nursing Theory; Nursing
INTRODUCTION
The surgical treatment of organ removal seems to meet a number of pathologies that emerge as health needs of populations, being considered a procedure that causes feelings of anxiety and uncertainty in patients. When the patient experiences the uncertainty resulting from a disease or treatment, it may result in stress that affects the mind, body and social relations. In addition, after completion of a surgical procedure, the patient may feel pain, momentary or permanent loss of function of the organ and some level of care dependency that interfere in his/her activities of daily living, not being uncommon the fear of disease relapse, fear of post-surgical limitations and psychological distress 1,2.
The surgery can be considered as an aggression. Starting from the physiological and anatomical aspects involved related to the incision, which breaks the skin integrity, bleeding and the organ removal. On the other hand, regarding the psychological phenomena involved, fear, distress, doubt, uncertainty and expectation arise. However, the psychological aspects of surgical treatments are often disregarded, considered by the multidisciplinary team as secondary 3,4.
Conflicting feelings are present in those patients who undergo the organ removal. The surgical treatment is often necessary as an intervention in the treatment of diseases. There are many feelings, expectations and perceptions involved. The patient may create expectations about the results of a surgical intervention, leading to emotional damage that interferes in the patient’s physiological functioning, affecting his/her general well-being 5. The surgery can be accompanied by anxiety, doubts and longings regardless of the surgery size. Surgical intervention is considered a threat to the patient, because, in addition to breaking the physical integrity, it causes major emotional impacts and fragility caused by fear 5.
In this context, the state of uncertainty is installed. The uncertainty in illness was presented by a nursing theorist called Merle Mishel, who developed the Theory of Uncertainty in Illness (6. The uncertainty is defined as the inability to assign meanings to events related to illness 6. The theory emphasizes that, with the onset of illness uncertainty, there is need to reorganize and search for coping strategies, as well as adaptation 6. Studies affirm that the establishment of uncertainty may lead to a feeling of lack of control over life events and negative feelings, which include isolation, loss of identity, hopelessness and demoralization 7)(8)(9. High levels of uncertainty associate with reduced skills, such as processing of new information, understanding of outcomes and adaptation to the disease diagnosis 10. Currently, the model of illness uncertainty has been widely used and recognized by the literature, addressing different contexts of health problems 10.
Still on the Theory of Uncertainty in Illness, health professionals are defined as important information providers 11. Evidence characterizes the lack of information as a great generator of uncertainty. On the other hand, the provision of information is an important strategy frequently used to face this condition 12. It is noteworthy that in the act of communicating information to the patient, it is essential to provide them with the ability to interpret, assimilate and reproduce them; it is up to the health professional to search for effective strategies to make himself understood. Studies describe flawed experiences between health system information providers and the patient during treatment, that is, reporting the practice of partial information or even the lack of it 11,13. These studies also reveal the need for synchronism between the communication between the health professional and the patient. After all, while one is thinking about how to manage the side effects inherent to the treatment, the other may be wondering how long it will take to recover or survive. In this sense, it is essential to harmonize the purpose of communication 11,13.
Therefore, the objective of this study is to investigate the uncertainty in illness, according to Mishel’s theory, in surgical patients of organ removal.
METHOD
Design
Cross-sectional, descriptive and exploratory study.
Study Population and Context
There was selection of 63 patients admitted to the surgical clinic of a university hospital in Brazil in the year 2017. The Hospital is a public institution the provides care free of charge through the Unified Health System (UHS). It has a Center of High Specialty in Oncology and the research was developed at the Surgical Outpatient Clinic that meets the following surgical specialties: Cranio-maxillofacial, general, pediatric, thoracic, vascular and neurosurgery. The surgical clinic meets pre and postoperative patients and has 39 beds installed. During data collection, there was a wide range of surgeries that involved the removal of part of or whole organs.
The sample number of participants was obtained through a sample calculation, considering the flow of patients hospitalized at the University Hospital for surgery of organ removal in the year prior to the data collection. The sample calculation resulted in 66 patients considering 95% confidence interval and 10% accuracy. Due to the period available for data collection, it was possible to collect 60 patients. Sample calculation used the R ® software version 3.4.
The participants were selected by convenience sample. The inclusion criteria were patients aged greater than or equal to 18 years, of both sexes, in postoperative period exceeding 24 hours who underwent surgery that involved removal of an organ, in full intellectual and mental conditions to answer the questions. The exclusion criteria were patients who did not meet the concept of organ removal used in the research.
Variables
Sociodemographic and clinical variables were collected to identify the sample profile. In this study, there stands out the importance of clinical variables that allowed identifying the profile of surgeries of removal of organs in the sample. Furthermore, data were collected using Mishel Uncertainty in Illness Scale - MUIS 14.
Data collection
The participants were selected from medical records and were instructed on how to participate in the research. There was the application of the data collection instrument built by the researchers, validated by three experts in the areas of surgery and systematization of nursing assistance, all with minimal training of ten years in nursing, active professors and in the care with clinical or surgical patients and with experience in the implementation of the nursing process. The instrument included sociodemographic and clinical questions. The MUIS was also used, validated for Portuguese, whose psychometric properties analyzed in the validation process were content validity (judges’ committee), the construct validity (confirmatory factor analysis and comparison of the means of the factors and the total scores according to the sociodemographic variables of the target audience), the reliability (test-retest and Cronbach's alpha) 15. This validated scale contains 30 Likert-type items, and, the higher the patient’s score, the greater the degree of uncertainty in illness, ranging from 30 to 150 points 14,15.
The MUIS aims to measure the uncertainty in illness through the items divided into areas, namely: ambiguity, complexity, inconsistency and unpredictability, of which the statements represent the forms of manifestation of uncertainty. The data collection lasted three months and four days, performed by one of the authors. The interview and application of the scale lasted around 2 hours comprising the mentioned steps. After this step, the patient’s medical records were consulted for further information.
Data analysis
Descriptive statistical analysis of sociodemographic and clinical data through measures of central tendency, mean and median, and of dispersion (standard deviation), simple and absolute frequencies of quantitative variables. The software Excel® 2016 was used. The score of MUIS was obtained by the sum of the scores for each item. There was also the evaluation of the frequency of responses related to the scale. To assess the reliability of the scale items, the Cronbach’s Alpha was used, considering values equal to or above 0.70 as accepTable.
For the correlations between the most prevalent surgeries in the sample and the uncertainty domains, the Mann-Whitney statistical tests were used. Results were considered statistically significant at p ≤ 0.05. This correlation analysis considered the means obtained in each MUIS domain, namely: Lack of clarity, Ambiguity, Lack of Information and Unpredictability. The mean obtained were also applied, considering all the scale items, which was named Total. The statistical tests were obtained through the software R v3.4 ®.
Ethical considerations
The project was approved by the Research Ethics Committee at the Health Sciences School of the University of Brasília - CEPFS/UnB, under CAAE 55134615.7.0000.0030, opinion number 2.177.498. For the research execution, the Informed Consent Form - ICF was made available for the participant. The participants could quit the study at any stage of the research.
RESULTS
During the data collection period, 63 patients were selected, however, three patients gave up during the interview. Among the 60 remaining patients, 47 (78.3%) were females and 13 (21.7%) males. The age ranged from 18 to 87 years, the mean was 51.9 (±16.4) years. Table 1 summarizes the sociodemographic characteristics of the sample.

Pardo is defined as people with a mixture of skin colors, be it this mulatto miscegenation (descendants of whites and blacks), cabocla (descendants of whites and amerindians), cafuza (descendants of blacks and indians) or mixed race.
Table 2 presents the descriptive statistical measures needed to test the relationship between the uncertainty domains and the educational level of the study participants.

Associations between the Uncertainty domains and all sociodemographic and clinical variables in the study were tested. From the Mann-Whitney test, only between the education variable and the Uncertainty domains, statistical significance was found for the domains “Lack of clarity” (p = 0.001), “Lack of information” (p = 0.01) and also in the “Total Uncertainty” (p = 0.002). The “total” corresponds to the significance test of the four domains as a whole, that is, all items of the MUIS scale.
Although only educational level presents a statistically significant difference for uncertainty, the sociodemographic profile of patients obtained shows a predominance of low family income (p > 0.05). Most participants were retired, with family income ranging from 1 to 2 minimum wages (41.7% of participants).
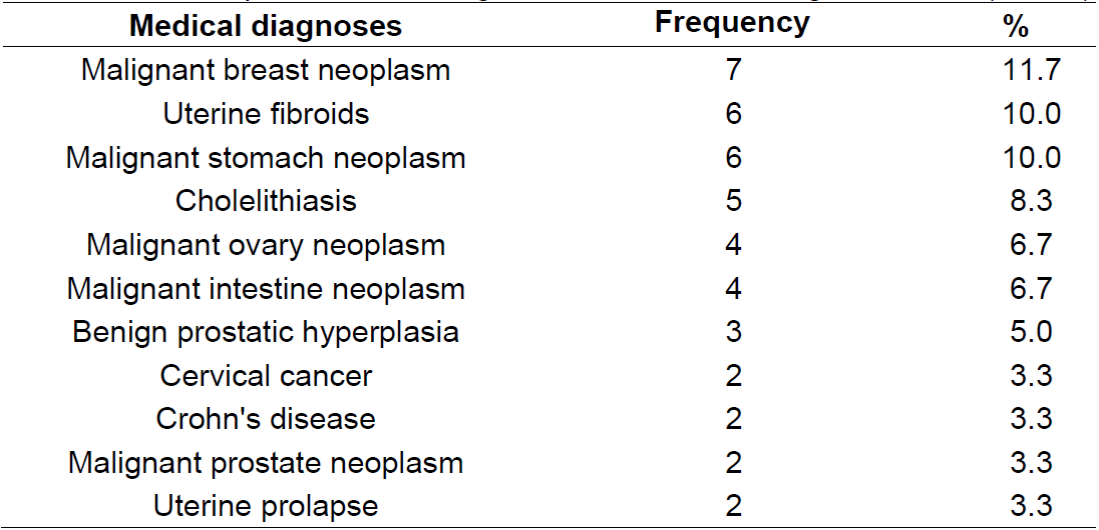
Among the 28 medical diagnoses of participants, the ten described in Table 3 were the most frequent, identifying an important heterogeneity of diagnoses that motivated the surgical procedures. The profile of medical diagnoses of participants reveals that the most frequent diseases were the neoplasms.
According to Mishel 9, the total score for each patient can vary between 30 and 150, whose higher value represents greater uncertainty in illness. Nevertheless, 11 (18%) patients reached score higher than or equal to 100, 13 (22%) patients greater than or equal to 90, 17 (28%) patients higher than or equal to 80, 10 (17%) patients higher than or equal to 70, 8 (13%) patients higher than or equal to 60 and 1 (2%) below 60. The range with greater prevalence of patients was that whose scores were higher than or equal to 80, with 17 patients. The lower record was only one patient for the range below 60. Each participant presented a response for each item, and all responded to all items.
The reliability of the scale was verified through the evaluation of its internal consistency. The value found for the Cronbach’s Alpha coefficient was 0.842.
Table 4. Relationship between abdominal hysterectomy surgery and the Uncertainty domains (n = 60).

* p < 0.05.
Concerning the surgical procedures the participants underwent, there stood out Hysterectomy and Mastectomy surgeries. Hypothesis tests were applied to all 28 surgical procedures arising from the study, however, Hysterectomy and Mastectomy were those that presented the most significant results, represented in Table 4 and Table 5, respectively.
Through the p values depicted in Table 4, there was statistically significant relationship only for the domain “Lack of information” about the Hysterectomy, thus being higher in the group that did not undergo this surgery.
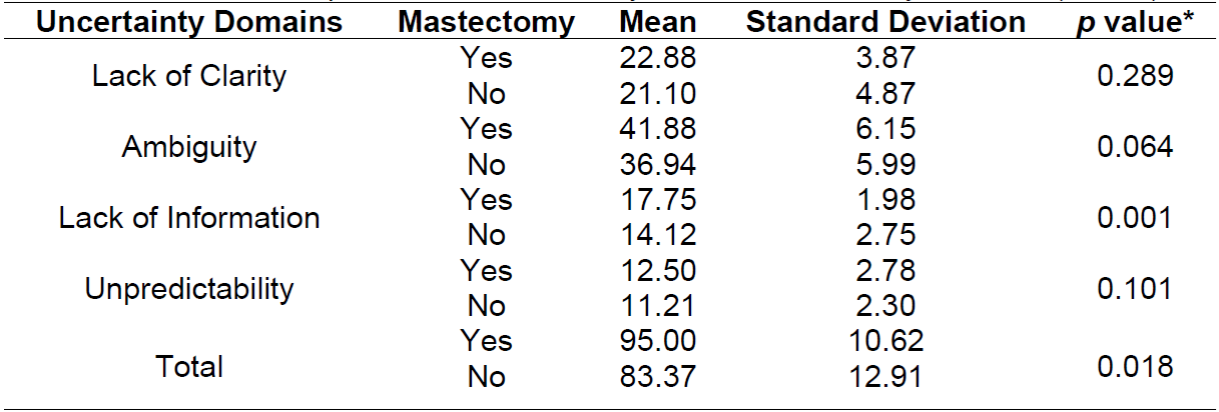
In the case of mastectomy, Table 5, there was a statistical relationship with the domain “Lack of information” and “Total Uncertainty” domains, which evaluate the four domains simultaneously, among those patients submitted to mastectomy.
DISCUSSION
Regarding the application of MUIS, it proved to be a tool of great applicability to measure uncertainty 7)(8)(11)(16)(17)(18. The score obtained for the study participants was very expressive, because 75% of them presented significant scores of the experience of uncertainty, in which the lowest score was 57 and the highest, 108 points. The following studies showed similar scores. The study of Hagen et al. 7) applied to patients with breast cancer to assess the uncertainty obtained a moderate degree of presence of uncertainty among the participants, with a scale that ranged from 33 to 165. Another study involving gastrectomized patients revealed that the participants showed a high level of uncertainty 19.
The reliability of the scale items describes how the instrument applied is able and accurate. The value of Cronbach’s Alpha (0.842), which measures the internal consistency of the items generally for the domains, was considered good as proposed by the literature 9. This corroborates the value of Alpha found in a study of validation of the MUIS scale for chronic patients in Italy 8. The literature also contains parameters of variation of Alpha in a range from 0.74 to 0.92 11.
A survey of survivors of breast cancer used the MUIS, obtaining total Cronbach’s Alpha equivalent to 0.849 9. In another study of the application of MUIS, the Cronbach’s alpha coefficient of the scale items was considered accepTable with a value of 0.72 20.
The profile of medical diagnoses for the study participants shows that the most frequent diseases were the neoplasms. In Brazil, the different types of cancer that have affected the population result from the demographic and epidemiological transition 16. Factors are strongly associated with the occurrence of certain neoplasms, such as the precarious socioeconomic conditions, associated with breast, prostate, colon and rectum cancer, strongly evidenced in this study 16.
The diagnosis of cancer involves complex situations that can generate feelings such as anxiety, fear, anguish, loneliness, lack of control of the situation and loss of self-identity, associated with a high level of uncertainty 19. According to the Theory of Uncertainty in Illness, the appearance of neoplasms enables the use of resources such as antecedents of uncertainty, providers of structure and recasting of the cognitive scheme 11.
As for the surgical procedures abdominal hysterectomy and mastectomy, which were the most prevalent for the participants, their results are significantly associated with uncertainty domains: the lack of information as p = 0.048 and the p values from the lack of information (p = 0.001) and total (p = 0.018).
Initially, for abdominal hysterectomy surgery, the domain “Lack of information” obtained higher averages, for those who did not undergo the abdominal hysterectomy surgery.
Although there was no statistical difference of uncertainty between the group that underwent hysterectomy and the one that did not, in the item “Lack of information”, the mean values were very close. This result assumes that there was a greater provision of information to patients who underwent the uterus removal, compared to other surgical procedures. A study with hysterectomized women reported good supply of information and positive results in the postoperative period 21.
For the participating patients, the surgical procedures arising from the need to extract a tumor or even to cease problems such as constant bleeding and pain, represented the way out for experienced problems, often for long periods. The organ removal imposes the need to live with this absence, which generates many insecurities and uncertainties 22. In the present study, there was a diversity of surgical indications that brought in a variety of situations, which, in general, resulted in a degree of uncertainty.
The literature has also reported the benefits in performing a hysterectomy, translating important ambivalence of feelings regarding this surgical procedure. Many women undergo the uterus removal due to episodes of anemia, fatigue, headaches and constant bleeding, interfering in their quality of life, exposing them to awkward situations 23. Therefore, the surgery can also be seen as a possibility of healing and resolution of problems, and in such cases, the organ removal is more easily accepted, and the expression of uncertainty does not associate with the lack of information, since they feel more confident in this case 24.
The mastectomy performed in the study participants were motivated by cancer and, in one of the cases, breast infection. Regardless of the surgical motivation, this procedure generates serious psychological, social and physical impacts in women 9. The change caused in the body image, through the experience of an absence of a visible part of the body, can influence the relationship with the family, with the sexual partner and herself. Added to this is the constant fear of the disease relapse and the unpredictability of the future 25.
A qualitative study with women in the pre-operative mastectomy revealed that the medical instructions prior to the surgical procedure are concentrated only in the steps proposed by the surgery, consequently showing weakness in professionals’ approach of the person. In addition, they did not consider the person as an integral being, as a subject with feelings and anguish, with doubts and uncertainties, who requires time and careful attention 26. Regarding the nurse’s evaluation, this was seen as someone who asks questions to gather information about the patient’s health status and gives instructions regarding the surgical preparation 26.
Faced with this vision, not only does the nurse need to collect data and provide instruction, but also be attentive to the management of anxiety, fear and suffering, embracing with qualified listening, covering aspects such as postoperative recovery, access to counselling by the multiprofessional team, possibility of recovery of body image and other necessary care. In this way, the nurse has the potential in the pre-operative to make the surgery a more peaceful and less traumatic moment, which will affect the surgical recovery 27.
The lack of information prevents the formation of the cognitive scheme, which is the personal interpretation of the individual regarding his/her disease, treatment and hospitalization 6.
Another factor related to a possible cause for the relationship between the lack of information and uncertainty obtained in this study is the educational level of the participants. One study reported that patients with gynecological cancer that had higher education showed lower levels of uncertainty than those with less education, due to their ability to understand better the information about their condition. These data corroborate the results obtained in this study, after all, the participants comprise mostly people with low schooling and with significant levels of uncertainty 22,25. Educational levels can adversely affect communication between patient and health care provider, and can create barriers to understanding treatment options and symptom management.
According to the Disease Uncertainty Theory, there is an inversely proportional relationship between educational level and uncertainty 6. In a study 13, using the theory, it was found that both low education and low income were predictive factors for high levels of uncertainty, corroborating the current study. It is noted that a low purchasing power influences the decrease in the patient's quality of life and can cause increased uncertainty.
A study on uncertainty with patients who had vulvar neoplasms and who underwent mutilating surgery involving organ removal, highlights that greater uncertainty is also correlated with: advanced age, married family status, lower education, lower income, lower quality of life, less social support and insufficient information 28. Although this study only involved women, the greater predominance of women in the current study allows us to correlate previous findings with the results obtained so far in relation to: advanced age, married marital status, less education, lower income and insufficient information. Although the Uncertainty in Disease Theory does not mention what may be a limitation of the model, the patient's monthly income and sociodemographic profile may be associated with events related to uncertainty.
Many times, when the patient seeks the nurse to have his/her doubts answered, the nurse explains that the medical professional is responsible for answering them, denying his/her competence, often justified by the lack of time and several activities requested by other patients between calls and procedures. This reality cannot be a habit, because demanding time for the communication with the patient whenever requested is an activity as important as the follow-up of the surgical wound 29. It is also important to offer the necessary structure for this professional to offer the necessary care to the patient, the correct dimensioning of professionals, material, physical resources and multiprofessional support are measures that help in the performance of these functions 30.
Nursing can intervene to reduce the patient’s degree of uncertainty as it provides information about his/her condition. Offering educational, social and structural support is an important requirement for patients to know and understand the entire context in surrounding them, that is, to provide coping mechanisms 13. Another research reveals that the more the patient is informed, the greater the chances of major changes and good treatment results, and that the number of contacts between the doctor and the patient, in addition to the entire multidisciplinary team, influences the success of the treatments 31.
Knowledge is the main way for patients to manage uncertainty. That is why the information provided by nursing and the entire multidisciplinary team is so important. The information needs to be personalized and adapted to the cultural level, as it helps the patient to develop his/her understanding and experience of the meaning of the disease in order to obtain more strategies to face the changes implied by this condition. 12.
As a limitation, there stands out the heterogeneity of participants, which hinders the extrapolation of results found, which is possible only with similar studies. Another limitation is that the study sample size was small, associated with a convenience sample from a treatment center. Circumstances that stress the need for expanding the research to other treatment centers.
CONCLUSIONS
As conclusions, through the application of MUIS, the study demonstrated the presence of elevated levels of Uncertainty, verified by the patients’ scores, highlighting the need for managing this condition. The results obtained also revealed that the psychosocial aspects of surgical treatments are disregarded at the expense of the clinical restoration, circumstances that neglect the patient’s emotional suffering.
There is still the need for improving communication between the health professional and the patient, to prevent the manifestation of the lack of information, one of the forms of the expression of uncertainty. Aspects such as the patient’s socioeconomic profile, educational level and income must be taken into account in the surgical treatment of organ removal.
The uncertainty experienced by these patients needs to be better known and widely disseminated so that these aspects gain prominence in the health care setting.
REFERENCIAS
1. Lee I-M, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Impact of Physical Inactivity on the World's Major Non-Communicable Diseases. Lancet [Internet]. July 21, 2012 [cited June 14, 2020];380(9838):219-29. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3645500/ [ Links ]
2. Carvalho R de, Bianchi ERF. Enfermagem em Centro Cirúrgico e Recuperação. In: Enfermagem em centro cirúrgico e recuperação. Barueri: Manole; 2016. [ Links ]
3. Gonçalves TF, Medeiros VCC. The preoperative visit as the anxiety mitigating factor in surgical patients. Rev. SOBECC, São Paulo. 2016; 21(1):22-7. Available from: https://sobecc.emnuvens.com.br/sobecc/article/view/38/pdf. DOI: 10.5327/Z1414-4425201600010004. [ Links ]
4. Oliveira TR, Souza JR. Avaliac¸a~o do impacto psicossocial do diagno´stico e tratamento do ca^ncer na vida de familiares cuidadores de pacientes em regime de internac¸a~o hospitalar. Tempus, Actas Sau´de Colet, Brasília. 2017 Mar;11(1), 215-227. Available from: http://docs.bvsalud.org/biblioref/2018/03/880750/lgbt-11-portug.pdf DOI: https://doi.org/10.18569/tempus.v11i1.2228 [ Links ]
5. Santos MMB dos, Martins JCA, Oliveira LMN. A ansiedade, depressão e stresse no pré-operatório do doente cirúrgico. Rev. Enf. Ref. [Internet]. 2014; serIV(3):7-15. Available from: https://rr.esenfc.pt/rr/index.php?module=rr&target=publicationDetails&pesquisa=&id_artigo=2461&id_revista=24&id_edicao=68 [ Links ]
6. Mishel MH. Uncertainty in Illness. Image: the Journal of Nursing Scholarship [Internet]. 1988 [cited June 14, 2020];20(4):225-32. Available from: https://sigmapubs.onlinelibrary.wiley.com/doi/abs/10.1111/j.1547-5069.1988.tb00082.x [ Links ]
7. Hagen KB, Aas T, Lode K, Gjerde J, Lien E, Kvaløy JT, et al. Illness uncertainty in breast cancer patients: Validation of the 5-item short form of the Mishel Uncertainty in Illness Scale. European Journal of Oncology Nursing 2015;19(2):113-19. https://doi.org/10.1016/j.ejon.2014.10.009 [ Links ]
8. Giammanco MD, Gitto L, Barberis N, Santoro D. Adaptation of the Mishel Uncertainty of Illness Scale (MUIS) for chronic patients in Italy. Journal of Evaluation in Clinical Practice 2015;21(4):649-55. doi:10.1111/jep.12359 [ Links ]
9. Hall DL, Mishel MH, Germino BB. Living with cancer-related uncertainty: associations with fatigue, insomnia, and affect in younger breast cancer survivors. Support Care Cancer [Internet]. April 12, 2014 [cited June 14, 2020];22(9):2489-95. Available at: https://europepmc.org/article/med/24728586?client=bot [ Links ]
10. McEwen M. Visão Geral de algumas teorias de enfermagem de médio alcance. Em: McEwen M, Wills EM, editores. Bases teóricas de enfermagem, Porto Alegre: Artmed; 2016, p. 246-54. [ Links ]
11. Mishel MH, Clayton M. Theories of uncertainty in illness. In: Smith MJ, Liehr PR (Eds.). Middle range theory for nursing. 2nd ed. New York: Springer; 2008. [ Links ]
12. Bailey Jr D, Stewart JL. Teoría de la incertidumbre frente a la enfermedad. In: Alligood MR, Tomey AM, editors. Modelos y teorías en enfermeira 7. ed, Madrid: España: Elsevier Science; 2011. 599-617. [ Links ]
13. Gómez-Palencia IP, Castillo-Ávila IY, Alvis-Estrada LR. Incertidumbre en adultos diabéticos tipo 2 a partir de la teoría de Merle Mishel. Aquichan [Internet]. 2015 Apr [cited 2020 Oct 26]; 15(2):210-218. http://dx.doi.org/10.5294/aqui.2015.15.2.5. [ Links ]
14. Mishel MH. The measurement of uncertainty in illness. Nursing Research 1981;30(5):258-63. https://doi.org/10.1097/00006199-198109000-00002 [ Links ]
15. Barbosa IV. Tradução, adaptação e validação da Mishel Uncertainty in Illness Scale for Family Members: aplicação em familiares de pessoas com paraplegia. Fortaleza. Tese [Doutorado em Enfermagem] - Faculdade de Farmácia, Odontologia e Enfermagem da Universidade Federal do Ceará; 2012. Available from: http://www.repositorio.ufc.br/handle/riufc/15629. [ Links ]
16. Brasil. Ministério da Saúde. Brasil. Instituto Nacional do Câncer José Alencar Gomes da Silva. Coordenação de Prevenção e Vigilância. Estimativa 2020: Incidência de Câncer no Brasil. Rio de Janeiro; 2019. Available from: https://www.inca.gov.br/sites/ufu.sti.inca.local/files//media/document//estimativa-2020-incidencia-de-cancer-no-brasil.pdf. ISBN 978-85-7318-389-4. [ Links ]
17. Bolívar Montes LA, Montalvo A. Uncertainty associated to parents of preterm infants hospitalized in neonatal intensive care units. Investigación y Educación en Enfermería, 2016;34(2):360-67. http://dx.doi.org/10.17533/udea.iee.v34n2a16. [ Links ]
18. Aldaz BE, Hegarty RSM, Conner TS, Perez D, Treharne GJ. Is avoidance of illness uncertainty associated with distress during oncology treatment? A daily diary study. Psychol Health. 2019 Apr;34(4):422-437. doi: 10.1080/08870446.2018.1532511. Epub 2019 Jan 4. [ Links ]
19. Jeon BH, Choi M, Lee J, Noh SH. Relationships between gastrointestinal symptoms, uncertainty, and perceived recovery in patients with gastric cancer after gastrectomy. Nursing & Health Sciences. 2016;18:23-29. Doi: 10.1111/nhs.12219 [ Links ]
20. Torres-Ortega C, Peña-Amaro P. Adaptación cultural de la escala de incertidumbre de Mishel en el paciente tratado con hemodiálises. Enfermería Clínica 2015;25(1):9-18. DOI: 10.1016/j.enfcli.2014.09.002 [ Links ]
21. Oliveira TMG de, Jesus CAC de. Incertezas vivenciadas por pacientes po´s-ciru´rgicos diagnosticados com neoplasias. Rev enferm UFPE on line, 2018 out;12(10):2873-82. Available from: https://pubmed.ncbi.nlm.nih.gov/26713368/ [ Links ]
22. Kuang K, Wilson SR. A Meta-Analysis of Uncertainty and Information Management in Illness Contexts. Journal of Communication, 2017;67(3):378-401. doi:10.1111/jcom.12299. [ Links ]
23. Barbosa ARS, Santos AN, Rodrigues TS. Experiência de mulheres que realizaram histerectomia: revisão integrativa. Revista Uningá. 2018; 55(2):227-41. Available from: http://34.233.57.254/index.php/uninga/article/view/2202 [ Links ]
24. Teixeira MR, Batista EC. Vivencias Cotidianas da Mulher Histerectomizada: Narrativas e Contextos. Rev. Enfermagem e Sau´de Coletiva. 2016; 1(2):91-107. Available from: https://www.researchgate.net/publication/320935572_Vivencias_Cotidianas_da_Mulher_Histerectomizada_Narrativas_e_Contextos_Daily_Lives_of_Hysterectomized_Woman_Narratives_And_Contexts. ISSN: 2448-394X. [ Links ]
25. Hilton BA. The relationships of uncertainty, control, commitment, and threat of recurrence to coping strategies used by women diagnosed with breast cancer. J Behav Med. 1989;12(1):39-54. DOI: 10.1007/bf00844748 [ Links ]
26. Pahlevan SS, Ahadzadeh AS, Perdamen HK. Uncertainty and quality of life of Malaysian women with breast cancer: Mediating role of coping styles and mood states. Applied Nursing Research 2017;38:88-94. doi: 10.1016/j.apnr.2017.09.012 [ Links ]
27. Viana DDA, Santana CCC de, Souza JRS. Análise das ações de enfermagem nas fases cirúrgicas da mastectomia. Revista Brasileira De Inovação Tecnológica Em Saúde. 2018;8(2):67-82. https://doi.org/10.18816/r-bits.v8i2.15556 [ Links ]
28. Raphaelis S, Mayer H, Ott S, Hornung R, Senn B. Effects of written information and counseling on illness-related uncertainty in women with vulvar neoplasia. Oncol Nurs Forum. 2018; 45(6):748-60. doi: 10.1188/18.ONF.748-760 [ Links ]
29. Takeshita IM, Araujo IEM. Communication strategies and interaction of the patient with the unconscious patient. Reme - Rev. Min. Enferm. 2011;15(3): 313-323. Avaliable from: http://www.reme.org.br/artigo/detalhes/40 [ Links ]
30. Gonçalves MAR, Cerejo MNR; Martins JCA. A influência da informação fornecida pelos enfermeiros sobre a ansiedade pré-operatória. Referencia 2017; IV(14): 17-26. Available from: http://www.index-f.com/referencia/2017/414017.php [ Links ]
31. Davison BJ, Goldenberg SL. Decisional regret and quality of life after participating in medical decision-making for early-stage prostate cancer. BJU International [Internet]. 2003 [cited 2020 Oct 26];91(1):14-7. Available from: https://bjui-journals.onlinelibrary.wiley.com/doi/abs/10.1046/j.1464-410X.2003.04005.x doi: 10.1046/j.1464-410x.2003.04005.x. [ Links ]
Received: June 09, 2021; Accepted: September 21, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
