










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.22 no.69 Murcia ene. 2023 Epub 20-Mar-2023
https://dx.doi.org/10.6018/eglobal.512211
Originals
Clinical and sociodemographic profile of users with chronic diseases in primary health care
1Federal University of Rio Grande do Norte, Natal, RN, Brazil
2Rio Grande do Norte Research Support Foundation, Natal, RN, Brazil
3Nursing Department, Federal University of Rio Grande do Norte, Natal, RN, Brazil
Objective:
to describe the clinical and sociodemographic life and health profile of users with chronic non-communicable diseases in Primary Health Care.
Method:
cross-sectional study with 80 users with chronic diseases in Rio Grande do Norte. A validated form was applied between January 2018 and March 2020. The results were analyzed with relative and absolute frequencies and a 95% confidence interval.
Results:
female users (87.5%), elderly people (51.3%), brown people (53.8%), informal employment (53.75%), incomplete elementary school (62.6%), income greater than one minimum wage (51.3%) prevailed. They were totally dependent on health care from the Unified Health System (93.85%) and were monitored by the Family Health Strategy (91.2%). As for health, the chronic diseases Hypertension (82.5%) and Diabetes Mellitus (56.3%) stood out; however (68.8%) the participants had no history of hospitalization due to a complication of the chronic disease.
Conclusion:
aging is an important factor for the presence of chronic diseases, including hypertension and diabetes mellitus. Users had unfavorable socioeconomic characteristics, such as low levels of income and education, which can compromise their quality of life and negatively influence the self-care actions. The total dependence on the public health system draws attention, this should direct health actions and strategies to combat and control chronic diseases.
Keywords: Primary Health Care; Non-Communicable Diseases; Health Profile; Hypertension; Diabetes Mellitus
INTRODUCTION
The last decades of the 20th century were marked by major changes in its age structure, resulting from the demographic transition process due to the aging of the population, accompanied by the epidemiological transition process characterized by the increase in morbidity and mortality indicators from chronic non-communicable diseases (CNCD), which pose a major challenge to health systems1)(2)(3.
Chronic non-communicable diseases such as diseases of the cardiovascular system and neoplasms, are long-term diseases associated with the development of limitations and disabilities, generating organic changes and changes in life habits with the need for specific care, which involve health promotion actions and adoption of healthier lifestyle1,4.
In addition, these diseases are included as causes of premature death, promotion of work disability, financial impact on the family and decrease in productivity, thus generating negative impacts on the individual's quality of life1)(2)(3)(4.
It is interesting to note that with the aging process and the population's lifestyle and changes in disease burdens, new health demands are observed, such as greater need for health services, longer hospital stays and constant monitoring4)(5. Individuals with socioeconomic vulnerability, and with less access to health services are the most exposed to the risks of diseases6, making it imperative to urgently meet these demands by health services.
Evidence shows that in Brazil, CNCD are responsible for 75% of health care expenditures in the Unified Health System (SUS), making them a challenge for public management, with a consequent increase in demand for specific care and rising costs for the SUS, due to the chronicity of these diseases1.
In this context, in response to this demand, Primary Health Care (PHC) stands out as the best level of care focused on promotion and prevention on chronic conditions, given that its model is based on care integral and continuous, with preservation of the bond, co-responsibility and the longitudinality of care2.
Health care in PHC for the care of users with chronic diseases focuses on health promotion, prevention and control of complications, encouraging behavioral changes in lifestyle, which, although they do not promote healing, allow maintaining the disease under control and/or in better conditions, providing better quality of life and reduced impacts on the individual's functionality7. In this way, PHC can direct its actions towards comprehensive care capable of restoring health status, quality of life and the autonomy of the users and/or the community2.
The epidemiological profile of the users assisted informs us about the occurrence and involvement of CNCD, as well as the need for PHC to act in the prevention and control of these diseases based on the identification of determinants present in the lives of users. It is care that avoids and/or delays the onset of complications and disabilities, in addition to premature death related to chronic non-communicable diseases. Therefore, it is essential to identify the socioeconomic and health characteristics in the population that are directly related to the risk factors for diseases and chronic conditions8.
Therefore, it is necessary to prioritize the recognition of the socioeconomic and morbidity and mortality profiles of the population served, as well as the identification of the health services used by users, indispensable for the minimization of existing barriers and the operationalization of care through health promotion actions, risk prevention and injuries, to meet an epidemiological surveillance plan to control chronic diseases.
Given the above, the objective of this study was to describe the clinical and sociodemographic profile of life and health of users with chronic non-communicable diseases in Primary Health Care.
METHOD
This is a quantitative, descriptive and cross-sectional study, guided by the tool Strengthening the Reporting of Observational Studies in Epidemiology (STROBE). This article comes from the post PhD project “Self-care of users with Chronic Non-Communicable Diseases and its relationship with socioeconomic conditions in the context of Primary Health Care”.
The study was carried out from January 2018 to March 2020, in the ascribed area of the Family Health Unit (FHU), located in a neighborhood with a population of 110 thousand inhabitants located in the Western Sanitary District, in the municipality of Natal, Rio Grande do Norte. Regarding the community in question, the presence of an adult population in the reproductive phase of work, with people over 60 years of age on the rise, in addition to high rates of unemployment, crime and low levels of education and income is highlighted9.
Eighty users participated in the research. These were chosen in a sample defined by non-probabilistic sampling technique of the intentional type; the inclusion criteria were age greater than 18 years, registered in an area of the Family Health Unit, diagnosed with at least one CNCD, and in good cognitive conditions to maintain dialogue during the interview.
The initial contact with the users took place in the FHU waiting room, while they were waiting for care, with the support of the service's nurses; data collection, through a structured interview using a validated form10, containing questions about sociodemographic variables, history of the disease, requirements and competences of self-care and care of health professionals. At times, the interview took place at the users' home, and in these cases, there was a prior planning of the unit and support from family members.
The data collected, related to the socioeconomic variables of race/color, marital status, sex, religion, profession, education, income and housing conditions, in addition to clinics and health care services, were tabulated and organized in an Excel spreadsheet. Subsequently, they were analyzed using the Statistical Package for Social Science (SPSS) version 20.0. The descriptive statistical analysis of the data was presented by relative and absolute frequencies, and their respective confidence intervals (95% CI), in simple Tables.
The study met the requirements of Resolution 466, of December 12, 2012, which regulates the standards for the development of research with human beings, and received approval from the Research Ethics Committee of the Federal University of Rio Grande do Norte (CEP-UFRN), under opinion number 3,002,347.
RESULTS
Among the participating users, 43 (53.8%) were brown, 31 (35.8%) were married, 70 (87.5%) were female, 50 (62.5%) were Catholic, 43 (53.75%) with informal employment, 50 (62.6%) with incomplete elementary education and 41 (51.3%) with income greater than one minimum wage, as seen in Table 1.
As for age, 39 (48.8%) of users were between 18 and 59 years old, with a mean age of 58.4 years; among the interviewed users, the youngest was 25 years old and the oldest, 85 years old, representing the minimum and maximum ages of the population studied.
Table 1. Sociodemographic characterization of users with non-communicable chronic diseases treated at the Family Health Unit (n=80). Natal, RN, Brazil, 2020.
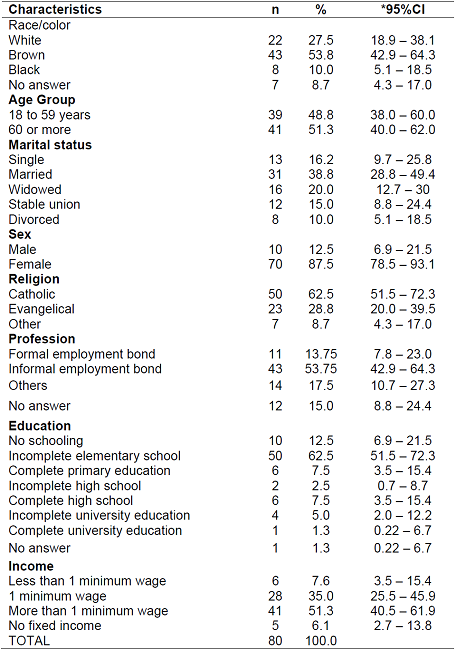
Source: Prepared by the authors, 2021.
n = number of participants;
*95%CI: 95% confidence interval.
Regarding housing status, 69 (86.3%) lived in their own home, 52 (65%) had basic sanitation, and 80 (100%) had electricity and running water.
Table 2. Characterization of housing for users with non-communicable chronic diseases, met at the Family Health Unit (n=80). Natal, RN, Brazil, 2020.
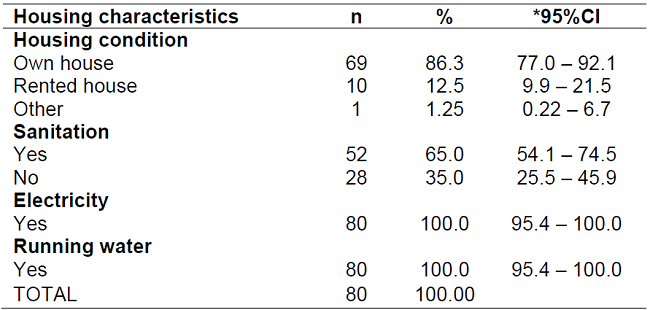
Source: Prepared by the authors, 2021.
n = number of participants;
*95%CI: 95% confidence interval.
As for the characterization of users' health, the results showed that, among the diseases mentioned, there were systemic arterial hypertension with 66 (82.5%), followed by diabetes mellitus, in 45 (56.3%) data shown in Table 3.
According to the care received from the health unit, 73 (91.2%) of the users interviewed were accompanied by professionals from the Units; with regard to registration and free access to medicines, 68 (85.1%) affirmed registration in a popular pharmacy and/or pharmacy of the Family Health Unit; another 55 (68.8%) denied previous hospitalization due to an CNCD, and still, 75 (93.8%) did not have a health plan, according to data recorded in Table 3.

DISCUSSION
CNCD are one of the biggest public health problems in the world. These are diseases that strongly interfere in the quality of life of individuals and in health services, in addition to being responsible for more than half of the deaths that occurred in Brazil in 201711.
Regarding the profile of users affected by CNCD, it was observed that the set of diseases and variables such as low income, low level of education and age affect the most vulnerable groups12. In Brazil, for example, it is clear that chronic diseases increase towards the most socially vulnerable segments6.
Related to the color of the participants, a study13 observed a higher prevalence of CNCD among individuals of brown race (57.4%). A similar prevalence is pointed out in this study if the socioeconomic characteristics are compared. This fact may be associated with the similarities of the population characteristics where data collection was carried out.
Regarding the age group, it is important to highlight that in the context of the aging process of the population, the multiplicity of health needs expressed by the elderly people, in the face of greater exposure to CNCD, demands that health services be able to adequately meet the needs of disease prevention and control, as well as being able to promote active and healthy aging, from a perspective of autonomy and well-being, with health promotion activities2.
The results also showed that (87.5%) of the female users were diagnosed with some type of CNCD. Such prevalence corroborates the literature, which points to studies in which chronic diseases were found mainly in women. And this circumstance may be related to the fact that women use health services more, as well as the fact that women have a greater perception of the signs and symptoms of diseases and, consequently, greater demand for health services, physicians, exams, among others6)(14)(15.
The importance of campaigns for the promotion, recovery and empowerment of men's health is highlighted. In this sense, the Ministry of Health edits the National Policy for Integral Assistance to Men's Health (PNAISH) with the aim of promoting a closer relationship between men and health services, especially those aimed at PHC. This measure, associated with a health service that is receptive to the demands of these users, may reflect a greater use of the services offered in PHC and consequently influence the reduction of injuries and diseases16.
Regarding the education variable, it can be seen that most of the interviewed users had incomplete elementary education. Similar results were found in the literature17 which indicate that most individuals surveyed had high school (30.3%), followed by elementary school (25.6%). Such findings were related to the fact that low levels of education can impair the prevention of CNCD and their risk factors, since it makes it impossible for the individuals to seek knowledge to promote health18, as well as other forms of prevention of diseases.
Other similar results(19) indicated the high level of education as a factor to be appreciated in the context of CNCD prevention, since these people tend to follow a healthier diet, reduce tobacco use, and perform more physical activities. Therefore, among health professionals, schooling is considered an important factor in the development of health education activities in PHC20.
The most prevalent CNCD are: cardiovascular diseases, cancer, Diabetes Mellitus and chronic respiratory diseases. They are responsible for more than half of all deaths in the world. Data from the National Health Survey (NHS) reveal that almost half of the population declares to be affected by at least one CNCD15. Hypertension is the most cited condition. This disease is characterized by sustained blood pressure levels above the normal blood pressure standard and is usually associated with organ functional alterations and/or metabolic alterations21.
Diabetes Mellitus, in turn, corresponds to a set of metabolic alterations resulting from problems in the action and/or secretion of insulin. As a result, there is a serum hyperglycemia that, if left untreated, can cause acute or chronic complications in the cardiovascular, kidney and neurological systems. When associated, these two conditions present greater risks for the development of kidney disease, coronary heart disease, heart failure and cerebrovascular accident21.
The PHC, through its health teams, develops actions to promote self-care, enabling the expansion of learning, as well as changes in lifestyle. In this way, aiming to train individuals for self-care so that they can present better clinical results, in their health status and better quality of life21)(22)(23. Therefore, PHC should encourage the development of practices that enable the reduction of modifiable risk factors, such as overweight, obesity, sedentary lifestyle and smoking24.
Difficulty in accessing health services for the population of this study was not an important risk factor, since 91.2% of respondents said they were accompanied by professionals from the Family Health Unit. In addition, 94.3% reported free access to medication for the treatment of chronic diseases, corroborating the results of a similar study25. However, the WHO26 highlights the difficulty in accessing and using health services as the main barrier to coping with CNCD.
Regarding hospitalization for complications of chronic disease, 68.8% of the interviewed users did not need hospitalization, which may be a reflection of the coverage given through the assistance model of the Family Health Strategy (FHS), since that this model demonstrates lower rates of hospital admission27. It is a model aimed at prevention and health promotion, being guided by a multidisciplinary team with the participation of the community, which, once capillarized to the community, is able to benefit the most vulnerable users, preventing them from being referred to other levels of health care unnecessarily24.
In the results of a national cross-sectional study, a majority of users were female, of mixed race, married or in a sTable relationship, without health plan, with social classification C and only with elementary education. As for the frequency of chronic diseases, hypertension, dyslipidemia, osteoarticular diseases (such as arthritis/arthrosis), depression and diabetes were the most cited by users23. These results, when compared to those of this study, identify similarities related to socioeconomic characterization and diseases evidenced by most users affected by CNCD.
These findings made evident the need to act on the conditioning factors and social determinants of health, in order to resolve inequalities and enable an integral and longitudinal approach to risk factors and CNCD28.
The importance and impact that PHC can have on the care of users with CNCDs is clear, highlighting prevention and health promotion practices. However, it is necessary to improve the monitoring of chronic diseases in PHC, in order to enable better planning and monitoring of the treatment of these users.
CONCLUSION
The clinical and socioeconomic profile observed was characterized by elderly people with high prevalence of hypertension and diabetes mellitus as the main CNCD, but without a history of hospitalization due to a chronic disease complication. These users had low levels of income and education that can compromise their quality of life and negatively influence the self-care actions.
Most users are totally dependent on the SUS and have access to the health service, based on monitoring with the family health team, which should guide health actions and strategies to combat and control chronic diseases.
Regarding the limitation of this research, the sample size is highlighted, due to the majority of the interviews being conducted only with the users present at the Family Health Unit. In addition, as this was a cross-sectional study, the findings did not allow the establishment of causal relationships, due to the cross-sectional design used.
Another limiting factor was the impossibility of a longer time for the data collection period due to the health emergency related to the COVID-19 pandemic decreed in March 2020 by the WHO.
REFERENCIAS
1. Wanderley RMM, Cunha DGP, Felisberto MAS, Oliveira BRS, Bittencourt GKGD, Amaral AKFJ, Silva AO. Avaliação da condição de saúde da pessoa idosa na atenção básica. Rev. enferm. UFPE on line [Internet]. 2019 [acesso em 10 mar 2021]; 13(2): 472-482. Disponível em: https://pesquisa.bvsalud.org/portal/resource/pt/biblio-1010347 [ Links ]
2. Schenker M, Costa DH. Advances and challenges of health care of the elderly population with chronic diseases in Primary Health Care. Cien Saude Colet. [Internet]. 2019 [acesso em 10 mar 2021]; 4(4):1369-1380. Disponível em: https://doi.org/10.1590/1413-81232018244.01222019 [ Links ]
3. Mendes EV. O cuidado das condições crônicas na atenção primária à saúde: o imperativo da consolidação da estratégia da saúde da família [Internet]. Brasília: Organização Pan-Americana da Saúde; 2012 [acesso em 30 mar 2020]. 512 p. ISBN: 978-85-7967-078-7. Disponível em: https://bvsms.saude.gov.br/bvs/publicacoes/cuidado_condicoes_atencao_primaria_saude.pdf [ Links ]
4. Figueiredo AEB, Ceccon RF, Figueiredo JHC. Chronic non-communicable diseases and their implications in the life of dependente eldery people. Ciência & Saúde Coletiva [Internet]. 2021 [acesso em 06 out 2021]; 26(1):77-88. Disponível em: https://doi.org/10.1590/1413-81232020261.33882020. [ Links ]
5. Veras RP, Oliveira M. Aging in Brazil: the building of a healthcare model. Cien Saude Colet. [Internet] 2018 [acesso em 10 mar 2021]; 23(6):1929-1936. Disponível em: https://doi.org/10.1590/1413-81232018236.04722018 [ Links ]
6. Barbosa RL, Silva TDCS, Santos MF, Carvalho FR, Marques RVDA, Matos Júnior EM. Perfil sociodemográfico e clínico dos idosos de um Centro de Convivência. Rev Kairos [Internet]. 2018 [acesso em 10 mar 2021]; 21(2): 357-373. Disponível em: https://doi.org/10.23925/2176-901X.2018v21i2p357-373 [ Links ]
7. Malta DC, Bernal RTI, Lima MG, Araújo SC, Silva MMA, Freitas MIF, Barros MBAB. Noncommunicable diseases and the use of health services: analysis of the National Health Survey in Brazil. Rev Saude Publica [Internet]. 2017 [acesso em 10 mar 2021]; 51(1): 4s. Disponível em: https://doi.org/10.1590/S1518-8787.2017051000090 [ Links ]
8. Cruz MF, Ramires VV, Wendt A, Mielke GI, Martinez-Mesa J, Wenhrmeister FC. Simultaneidade de fatores de risco para doenças crônicas não transmissíveis entre idosos da zona urbana de Pelotas, Rio Grande do Sul, Brasil. Cad Saude Publica [Internet]. 2017 [acesso em 10 mar 2021]; 33(2): e00021916. Disponível em: https://doi.org/10.1590/0102-311X00021916 [ Links ]
9. Barbosa IR, Gonçalves RCB, Santana RL Social vulnerability map for the municipality of Natal (Northeast Brazil) at a census sector level. J Hum Growth Dev [Internet]. 2019 [acesso em 10 mar 2021]; 29(1): 48-56. Disponível em: http://dx.doi.org/10.7322/jhgd.157749 [ Links ]
10. Santos RS. Autocuidado apoiado aos hipertensos: construção de um protocolo. Natal/RN. Tese [Doutorado em Enfermagem na Atenção à Saúde] - Programa de Pós-Graduação em Enfermagem da Universidade Federal do Rio Grande do Norte; 2016. [ Links ]
11. Malta DC, Andrande SSCA, Oliveira TP, Moura L, Prado RR, Souza MFM. Probability of premature death for chronic non-communicable diseases, Brazil and Regions, projections to 2025. Rev Bras Epidemiol [Internet]. 2019 [acesso em 10 mar 2021]; 22: E190030. Disponívem em: https://doi.org/10.1590/1980-549720190030 [ Links ]
12. Malta DC, Moura L, Prado RR, Escalante JC, Schimidt MI, Ducan BB. Mortalidade por doenças crônicas não transmissíveis no Brasil e suas regiões, 2000 a 2011. Epidemiol Serv Saude [Internet]. 2014 [acesso em 10 mar 2021]; 23(4):599-608. Disponível em: https://doi.org/10.5123/S1679-49742014000400002 [ Links ]
13. Melo SPSC, Cesse EAP, Lira PIC, Rissin A, Cruz RSBLC, Batista Filho M. Doenças crônicas não transmissíveis e fatores associados em adultos numa área urbana de pobreza do nordeste brasileiro. Cien Saude Colet. [Internet]. 2019 [acesso em 10 mar 2021]; 24(8):3159-3168. Disponível em: https://doi.org/10.1590/1413-81232018248.30742017. [ Links ]
14. Barros MBA, Francisco PMSB, Zanchetta LM, César CLG. Tendências das desigualdades sociais e demográficas na prevalência de doenças crônicas no Brasil, PNAD: 2003- 2008. Cien Saude Colet. [Internet]. 2011 [acesso em 10 mar 2021]; 16(9):3755-3768. Disponível em: https://doi.org/10.1590/S1413-81232011001000012 [ Links ]
15. Malta DC, Bernal RTI, Carvalho QH, Pell JP, Dundas R, Leylando A, et al. Women and evaluation of inequalities in the distribution of risk factors for Chronic non-communicable diseases (NCD), Vigitel 2016-2017. Rev Bras Epidemiol [Internet]. 2020 [acesso em 10 mar 2021]; 23: E200058. Disponível em: https://doi.org/10.1590/1980-549720200058 [ Links ]
16. Alves NA, Coura AL, França ISX, Magalhães IMO, Rocha MA, Araújo RS. Access of first contact in the primary health care: an evaluation by the male population. Rev Bras Epidemiol [Internet] 2020 [acesso em 10 mar 2021]; 23: E200072. Disponível em: https://doi.org/10.1590/1980-549720200072. [ Links ]
17. Silva KN da, Serafim AS, Rodrigues L de S, Oliveira JL de, Rodrigues G, Cavalcante EGR, Filho JA da S, Pinto AGA. Morbidades autorreferidas por usuários de espaços comunitários de atividade física. Av. enferm. [Internet]. 2020 [acesso em 10 mar 2021]; 38(2):182-90. Disponível em: https://doi.org/10.15446/av.enferm.v38n2.82514. [ Links ]
18. Melo LA, Lima KC. Factors associated with the most frequent multimorbidities in Brazilian older adults. Cien Saude Colet. [Internet]. 2020 [acesso em 10 mar 2021]; 25(10):3879-3888. Disponível em: https://doi.org/10.1590/1413-812320202510.35632018. [ Links ]
19. Sato TO, Fermiano TC, Bastião MV, Moccelin AS, Driusso P, Mascarenhas SHZ. Doenças Crônicas não Transmissíveis em Usuários de Unidades de Saúde da Família - Prevalência, Perfil Demográfico, Utilização de Serviços de Saúde e Necessidades Clínicas. Rev. Bras. Ciênc. Saúde [Internet]. 2017 [acesso em 10 mar 2021]; 21 (1): 35-42. Disponível em: https://pesquisa.bvsalud.org/portal/resource/pt/biblio-883138. [ Links ]
20. Dietrich A, Colet CF, Winkelmann ER. Perfil de Saúde dos Usuários da Rede de Atenção Básica Baseado no Cadastro Individual e-Sus. Rev. Pesqui. (Univ. Fed. Estado Rio J., Online) [Internet]. 2019 [acesso em 10 mar 2021]; 11(5):1266-1271. Disponível em: http://ciberindex.com/index.php/ps/article/view/P12661271. [ Links ]
21. Francisco PMSB, Segri NJ, Borim FSA, Malta DC. Prevalence of concomitant hypertension and diabetes in Brazilian older adults: individual and contextual inequalities. Cien Saude Colet. [Internet] 2018 [acesso em 10 mar 2021]; 23(11):3829-3840. Disponível em: https://doi.org/10.1590/1413-812320182311.29662016. [ Links ]
22. Borba AKOT, Arruda IKG, Marques APO, Leal MCC, Diniz AS. Knowledge and attitude about diabetes self-care of older adults in primary health care. Cien Saude Colet. [Internet]. 2019 [acesso em 10 mar 2021]; 24(1):125-136. Disponível em: https://doi.org/10.1590/1413-81232018241.35052016. [ Links ]
23. Marques MB, Coutinho JFV, Martins MC, Lopes MVO, Maia JC, Silva MJ. Educational intervention to promote self-care in older adults with diabetes mellitus. Rev Esc Enferm USP [Internet]. 2019 [acesso em 10 mar 2021];53:e03517. Disponível em: https://doi.org/10.1590/S1980-220X2018026703517. [ Links ]
24. Pereira HNS, Santos RIO, Uehara SCaceSA. Effect of the Family Health Strategy in reducing hospitalizations for chronic non-communicable diseases. Rev enferm UERJ [Internet]. 2020 [acesso em 10 mar 2021]; 28:e49931. Disponível em: https://doi.org/10.12957/reuerj.2020.49931. [ Links ]
25. Oliveira MA, Luiza VL, Tavares NU, Mengue SS, Arrais PSD, Farias MR. Access to medicines for chronic diseases in Brazil: a multidimensional approach. Rev Saúde Pública [Internet]. 2016 [acesso em 10 mar 2021];50(suppl 2):6s. Disponível em: https://doi.org/10.1590/S1518-8787.2016050006161. [ Links ]
26. WHO - World Health Organization. Global Health Estimates 2016: Deaths by Cause, Age, Sex, by Country and by Region, 2000-2016. Geneva: World Health Organization; 2018. [ Links ]
27. Maia LG, Silva LA, Guimarães RA, Pelazza BB, Pereira CS, Rezende WL, Barbosa MA. Hospitalizations due to primary care sensitive conditions. Rev Saude Publica [Internet]. 2019 [acesso em 10 mar 2021]; 53 (2). Disponível em: https://doi.org/10.11606/S1518-8787.2019053000403. [ Links ]
28. Malta DC, França E, Abreu DMX, Perillo RD, Salmen MC, Teixeira RA, Passos V, Souza MFM, Mooney M, Naghavi M. Mortality due to noncommunicable diseases in Brazil, 1990 to 2015, according to estimates from the Global Burden of Disease study. Sao Paulo Med J. [Internet]. 2017 [acesso em 10 mar 2021]; 135(3):213-21. Disponível em: https://doi.org/10.1590/1516-3180.2016.0330050117. [ Links ]
Received: February 22, 2022; Accepted: July 08, 2022
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
