










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.22 no.70 Murcia abr. 2023 Epub 26-Jun-2023
https://dx.doi.org/10.6018/eglobal.531691
Originals
Perception of the nursing staff about the culture and patient safety
1Autonomous University of Coahuila. Saltillo, Coahuila. Mexico
2High Specialty General Hospital ISSSTE Saltillo, Coahuila. Mexico
Introduction:
Patient safety is the reduction of risk in the presentation of injury, disability or death during health care. The complexity of health systems, the work environment, the patient's own situations and the hospital infrastructure predispose to the occurrence of adverse events (AE).
Objective:
To determine the relationship between patient safety culture, hours worked per week and the incidents in the last year of the nursing staff of a second level public hospital in the city of Saltillo, Coahuila.
Methods:
Descriptive correlational, sample of 113 nurses. Collection through a digital link, for the nursing staff that met the inclusion criteria. A social and labor data questionnaire and the Hospital Survey on Patient Safety Culture instrument were applied. The analysis was based on descriptive and inferential statistics.
Results:
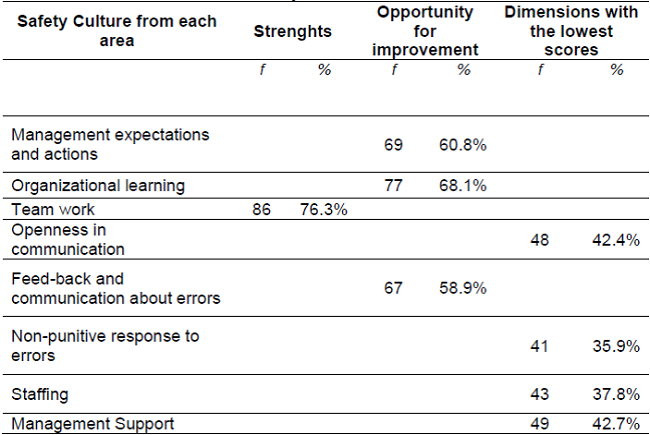
The patient safety culture lacks strength in most of the dimensions, with opportunities for improvement: management expectations and actions (60.8%), organizational learning (68.1%), feedback and communication about errors (58.9%) and only teamwork refers strength (76.3%). Lower scoring dimensions: openness in communication (42.4%), management support 42.7%, staffing 37.8 and non-punitive response to errors 35.9%.
Conclusions:
It is important to take this information into account so that strategies can be planted and developed to provide safe hospital care. Management action is important in the continuity of patient safety actions.
Key words: Patient safety; Adverse event; Hospital nursing staff
INTRODUCTION
Health systems are becoming more complex and stressful every day, the demand for care from the population has increased, professionals who offer health care must ensure patient safety. Currently, 134 million adverse events are reported per year with 2.6 million deaths, as a result of unsafe care; 15% of hospital expenses are a consequence of the occurrence of adverse events and four out of ten patients suffer damage that can be prevented in 80% WHO 1.
The concept of patient safety has varied as time progresses, first it was taken out only to point out the human errors that caused harm to the patient, later it focuses on the organizational situations in the institutions to understand the incidents that occurred 2. The culture of patient safety in the multidisciplinary team is reflected in a better quality of care and allows the creation of strategies for continuous improvement 3.
Therefore, care in the health care of hospitalized patients continues to have priority on the health agenda, in 2007 the WHO released the "Nine solutions for patient safety" (p.304), to reduce damages related to health care that cause great costs in health institutions 4.
Thus, patient safety represents a series of processes of the work organization that reduce the possibility of adverse events AE, as a consequence of the medical attention given to hospitalized patients. 5.
An adverse event (AE) is considered when an unforeseen and involuntary incident occurs during the patient's hospital stay. In addition, it can lead to disability, impaired health or death. Its occurrence is due to the complexity of the disease and the capacity of the professionals who are in charge of caring for patients. 6.
On the other hand, international and national organizations are always attentive to creating strategies to improve the safety of hospitalized patients by carrying out actions that are carried out by health institutions and professionals. The increase in AEs is expressed in the morbidity and mortality that occurs in the population served, such as: presentation of patient falls, misidentification of patients, pressure ulcers and lack of medication, among others. (7.
In the organizational environment, it is important that the management personnel be the first to become aware of the importance of offering safe and quality care and influencing other health personnel. The health team offers close care in patient care, so it is a responsibility to be up-to-date in everything that refers to patient culture and safety. This favors the reduction of risks for an AE to occur, it is important to provide safe care by obtaining knowledge, actively participating in all those actions that are carried out to see why the AE occur and to gain experience in the use of preventive measures and prevent the occurrence of these events. 8.
The processes of hospital certification and accreditation of the quality of care are carried out by external non-governmental organizations through a series of minimum standards, to carry out an evaluation of the care that is offered. 9Thus, the culture of patient safety is shown in the attitudes, values, beliefs and individual or group behaviors of health professionals that is related to better results in the care offered. (3) (9) (10.
Therefore, providing safe care implies creating an environment of trust, empathy and an organizational climate where actions are carried out that result in quality nursing care. Also take into account elements such as workload and communication to avoid less missed nursing care and the presentation of AE 11.
A series of elements are involved in patient safety that have to do with the patient himself, the interventions that are carried out with him and the infrastructure where care is offered, a perspective of a safe environment must be had. International institutions work for patient safety, among them are: the Council of Europe, the European Commission, the International Joint Commission with arguments such as promoting the culture in patient safety care, the notification of incidents and in the health professionals patient identification and assertive communication among others. The aforementioned is teamwork that encourages a culture of patient safety throughout the organization 12.
The nursing staff assumes an important role to advance the culture of patient safety in hospital care, facing a series of challenges such as lack or scarcity of resources and inadequate organizational infrastructure. In addition, there is a lack of capacity and competence in clinical decisions due to the lack of consistency in the content of the curriculum in terms of knowledge about patient safety 13.
On the other hand, there is an unfavorable and insecure environment such as the overwhelming number of patients to attend to, coupled with poor communication and work stress. Also sometimes a leadership with a lack of commitment, supervision, operational management and participation in decision-making on the safety culture. There are also clinical governance, accreditation and clinical risk management processes that are seen as more workload for staff. In addition to the handling of incidents from an individual and non-systemic way, the reporting of errors where there is no follow-up or feedback, the training that is given just to complete a class without active participation of the staff, the lack of a preventive approach before it occurs an incident, as well as the realization of teamwork with the absence of well-defined functions and roles and adequate interactions in a harmonious work environment 13.
After this, it can be seen that the attitude towards the presentation of an incident has to do with determining a notification method that allows not only to identify its incidence but also to know what it is due to. Health institutions must create a series of strategies to offer an adequate identification and care in the presentation of AE, so notifying and analyzing AE is part of managing a series of actions to respond to the problems presented and have better knowledge in decision-making for patient care and safety. Also consider the importance of having an information system to identify and monitor the presence of AE, avoiding acting punitively before the report 14,15.
OBJECTIVE
To determine the relationship between the culture of patient safety, the hours worked per week and the incidents in the last year of the nursing staff of a second level public hospital in the city of Saltillo, Coahuila.
METHODS
A descriptive correlational study was carried out in 158 nursing professionals assigned to a secondary care hospital. The sampling was non-probabilistic for convenience and taking the total population as a reference, the sample was calculated with an estimation error of .05 and a confidence interval of .95, obtaining a sample of 113.
Approval was requested by the Research Committee and the Research Ethics Committee of the Faculty of Nursing, Saltillo Unit of the Autonomous University of Coahuila. Once accepted, the permit was processed at the hospital unit, which was chosen for its accessibility and response time during the COVID-19 pandemic.
Once the application of the project was authorized by the health institution, it was distributed and supervised through one of the research collaborators to those who met the eligibility criteria, the data was collected from February to September 2020.
Within the inclusion criteria, the operative nursing staff who worked in the various care services, basic or temporary, with a current contract in the health institution, had at least six months working in the service surveyed and who agreed to participate in the service were included. voluntarily in the study. The shifts were considered: morning, evening, night and accumulated shift.
The information was obtained through a digital link on the Microsoft Forms platform that included informed consent, socio-labor data card such as age, sex, marital status, schooling, shift in which he works, service where he performs his functions, seniority in the institution and time spent working in the surveyed service. As well as, to measure the perception that the nursing staff has about the culture and safety of the patient, the Hospital Survey on Patient Safety Culture instrument was used, presented by the Agency for Healthcare Research And Quality, (AHRQ) of the United States and adapted to the Spanish by researchers in quality management from the University of Murcia, Spain from the Hospital Survey on Patient Safety.
The questionnaire uses 5 response options ranging from strongly disagree to strongly agree (16). It has been validated in different countries and has a Cronbach's Alpha that varies from 0.64 to 0.68. Likewise, it is structured with 12 dimensions of 3 to 4 questions per dimension: 1. Frequency of notified events; 2. Perception of security; 3. Expectations and actions of the management/supervision of the unit/service that favor safety; 4. Organizational learning/continuous improvement; 5. Teamwork in the unit/service; 6. Openness in communication; 7. Feed-back and communication about errors; 8. Non-punitive response to errors; 9. Staffing; 10. Hospital management support in patient safety; 11. Teamwork between units; 12. Problems in shift changes and transitions between services/units.
The interpretation of the results is taken into account from the analysis of the answers because there is a meaning for each item, as well as for each dimension. The original version and the adapted version are handled as a questionnaire. self administered. On the other hand, the questions in the questionnaire are expressed in positive and negative. The survey responses were recoded into the following sections: negative (strongly disagree, disagree); neutral (neither agree nor disagree) and positive (agree, strongly agree).
Lastly, to classify the dimension as strength, the following criteria are used:
≥ 75% of positive responses (“agree/strongly agree” or “almost always/always) to questions formulated in the positive.
≥ 75% negative responses (“disagree/strongly disagree” or “never/rarely”) to questions formulated in the negative
To classify the dimension as an opportunity for improvement, the criteria are:
The data was analyzed with the statistical package Statical Package for Social Sciences (SPSS) version 25 for Windows. Descriptive statistics of frequencies, proportions and percentages were used. The normality test was performed, obtaining a significance of less than .05. Therefore, a nonparametric statistic with Spearman's correlation coefficient was used.
The study was carried out in compliance with the Regulations of the General Law of Health in Research. In accordance with the Second Title, chapter I on the ethical aspects of research on human beings. In its articles 13, 14 in its sections IV, V, VI. 17 in its section I, 20, 21. With regard to informed consent, what is stipulated in the Helsinki Declaration of 1975 on the ethical principles for medical research on human beings is taken into account.
RESULTS
Regarding age, the participants showed an average age of 33 years ( χ̅ = 32.88; DE: 9.11),] Regarding age, the participants showed an average age of 33 years, in ages between 21 and 59 years; and in relation to marital status, the most prevalent were being single with 50.4% and married with 39.8%.
Regarding the labor variables, the shift in which they work, it was found that 51.3% work in the morning, 19.5% in the evening, 21.2% in the night and 8% in accumulated shift; Regarding the category, it was found that 41.6% are general, 31% auxiliary and 27.4% specialist; and in relation to the hours worked per week, an average of 40 hours was found ( χ̅ = 40.08; DE: 13.98).
According to the department where he currently performs his duties, the areas with the highest prevalence were the operating room with 31.9%, hospitalization with 14.2%, the Covid area with 10.6% and the emergency room with 9.7%.
According to the department where he currently performs his duties, the areas with the highest prevalence were the operating room with 31.9%, hospitalization with 14.2%, the Covid area with 10.6% and the emergency room with 9.7%.

For written incidents over the past year, an average of .62 was reported ( χ̅ = .62; DE: 1.55) and in turn the nursing staff qualifies in an average of 7 ( χ̅ = 7.39; DE: 2.23) the degree of patient safety in your service. Likewise, 88.5% regularly maintain contact with the patient.
On the other hand, the results in the dimension of the safety culture were, on the frequency of reported events, 68.7% and the perception of safety in 46.9% are without strength, but with an opportunity for improvement.
With respect to the safety culture at the service level, in the adjoining Table (Table 2), it can be seen that there is an opportunity for improvement with respect to the expectations and actions of management 60.8%, organizational learning 68.1%, communication about errors 58.9%; and 76.3% refer strength in teamwork. However, there are dimensions that scored lower such as: openness in communication represented by 42.4%, non-punitive response to errors with 35.9%, staffing with 37.8% and the perception of receiving support from part of the management in patient safety is referred to by 42.7%.
Regarding the opportunity to improve the culture of patient safety throughout the hospital, 50.4% reported teamwork between units and 50% reported the existence of problems in shift changes and transitions between services.
Regarding the category in which they work, a statistically significant positive correlation was obtained with the hours per week (rs= .211; p= .025), with the perception of safety (rs= .191; p= .043) and with the Feedback and communication on errors (rs= .273; p= .003). Likewise, it should be noted that the general nurses perceive the level of patient safety in their service at 9 and the specialists at 8 due to the workload and responsibility in the administration of drugs, which which is different in the auxiliaries that are dedicated to providing general care such as changing beds, hygienic care of the patient, assistance during the bath, among others. In Table 3, it is possible to observe the dimensions of the patient's safety culture and its relationship with the hours per week, where a statistical significance was shown; that is to say that the greater the hours of work, the greater the perception of security (rs= .316; p= .001), feedback and communication about errors (rs= .285; p= .002) and the non-punitive response to errors (rs= .280; p= .003).
In context with the above, it is observed that the higher the incidents reported in the last year, the higher the frequency of reported events. (rs= .216; p= .022), the expectations and actions of management/supervision (rs= .201; p= .033), organizational learning/continuous improvement (rs= .200; p= .033), openness in communication (rs= .274; p= .003) and the feed-back and communication about errors (rs= .243; p= .009).
Table 3. Patient safety culture, hours worked per week and incidents reported in the last year.
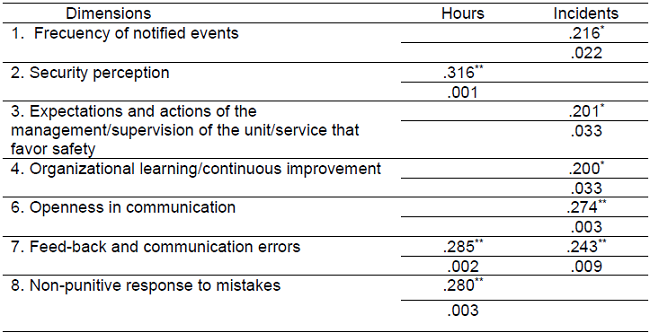
Note:** The correlation is significant at the .001 level n= 113
In summary, the results show that the patient safety culture lacks strength in most dimensions, but with an opportunity for improvement. However, the level of responsibility by category is a factor that influences patient safety, especially at the undergraduate and specialty level, who are responsible for drug administration. Likewise, the participants relate this lack of culture to the little support they receive from their superiors, to not receiving punishment for the mistakes made and to the fact that teamwork between units and shifts is weak at the hospital level.
DISCUSSION
Patient safety is a set of values and standards that must be carried out in an organization and represents a fundamental element in clinical practice 12.. Considering that efforts are made continuously to reduce the presentation of adverse events (AE), every hospital must have a protocol to record and report any incident that occurs in the institution, carry out actions that offer assistance, receive information and offer attention to preserve the prestige of the institution and the trust of the right holder18.
The nursing professional directly or indirectly cares for the patient in the hospital environment according to the category they have within the hospital, such as specialist, general or auxiliary, so it is necessary to identify all those elements that affect them and carry out actions that improve safety in patient care 7.
In this study, the teamwork dimension reached 76.3%, representing the only strength. This coincides with what was found by Santiago-González et al; which also equates this dimension as a strength to prevent the presentation of Adverse Effects in patient care. In addition, it must be considered that teamwork guarantees the willingness of the staff to implement strategies that favor the reduction of risks, as well as causing damage to the hospitalized patient. The other dimensions presented opportunity for improvement in both studies 19.
Regarding the expectations and actions of the management, the managers take into account the suggestions of the staff in their actions in favor of patient safety, in the present study this dimension represented 60.8%, lower than that reported in a study that I reach up to 70.01%. The support offered by the management is significant for patient safety, by showing interest in their managerial actions. Consequently, the management must reflect an adequate work environment and not act alone when errors occur 18.
The organizational learning dimension reached 68.1%, unlike what was found by other authors where this dimension is considered a strength and the percentage ranges from 82.94% to 100% respectively, the staff responded that changes are made in the organization and are valued to promote patient safety. Having this dimension as a strength reflects that we are working with a series of actions to improve and implement measures focused on patient care and thus avoid or reduce risks 18,19.
The dimension of feed-back and communication of errors presented 58.9%, also finding an opportunity for improvement different from what was reported in another study that, with respect to this aspect, obtained a lower score of 43.9%, referring to the problem of the report of the error. mistake. It is necessary to recognize when an unintentional incident has occurred and report the repercussion it has, this represents a commitment from several points of view: proposing alternative solutions, knowing the causes for which it occurred and, above all, based on the errors learn from them (20. In other studies, this dimension presents a higher percentage ranging from 65% to 75.3%21,22.
Within the dimensions with the lowest score are:
The trust that health personnel have with their managers favors the support of the implementation of an information system, so that health personnel express their situations that arise in the procedures that are carried out without fear of punitive actions 23. Regarding the openness dimension in communication, in this study it reaches only 42.4%, lower than the study carried out by Rivera et al, where 87.2% was obtained 24.
Regarding the non-punitive response to errors, it is another dimension with an opportunity for improvement, finding similarities with the study by Cruz et al and Fonseca-Mesa et al, in the field of patient safety when errors are made It should be taken into account that they are involuntary. Likewise, it should be avoided to create a culture where personnel are blamed and sanctions are reflected in their file. In addition, it is necessary to avoid generating fear and distrust of the personnel who work, since as a consequence there may be little disposition towards the indications of the direction 25,26.
Staffing reflects the sufficiency of staff and workload, product of the nurse/patient indicator, with an impact on the quality of daily care, in this study it presented only 37.8%. This is similar to what was reported in other studies, who mention that it is also necessary to take into account the seriousness of the patient and the time of care that they need, as well as the type of hiring that the human resource has (base or substitute) because the ability and dexterity in carrying out the procedures will be different (26,27. In another study, workers also stated that the lack of personnel caused fatigue and stress, coupled with negative feelings such as the desire to quit their job or not find meaning in the activities they perform. Therefore, there is an insufficiency in the care offered to the patient and, consequently, in the safety of their hospital stay 28.
Managers represent a fundamental element that is characterized by articulating services, staff and patients, this favors the culture of safety in health care. In addition, they must be attentive to the needs of patients to promote quality of care. In the dimension support for hospital management in patient safety, the study reported that the staff perceived dissatisfaction with the treatment received by their superiors, these findings are consistent with the article by Macedo et al., where dissatisfaction was shown for part of the nursing staff commenting that the management staff saw more for the benefit of the service than the benefit of the patients, so their answers had negative connotations (29.
Regarding the general perception of the patient safety culture, this study reports 50.4% teamwork between units throughout the hospital and 50% the existence of problems in shift changes and service transitions. Different from the 61.3% and 62.02% respectively reported in another study that presented a higher score in this dimension, however, in both studies there is an opportunity for improvement (30.
Regarding limitations, this study was affected by the SARS-CoV-2 pandemic, in Mexico the first case was presented on February 27, 2020, as of this date hospital environments are affected by the increase in cases of the disease. The study subjects were nursing professionals with patient care, so there is a need to collect information through a digital platform.
CONCLUSIONS
According to the objective of the study, it was found that regarding the results obtained regarding the perception of the nursing staff on the culture of patient safety, they show that most of the dimensions have an opportunity for improvement. , although some dimensions were characterized by having the lowest scores such as: openness in communication represented by 42.4%, non-punitive response to errors with 35.9%, staffing with 37.8% and the perception of receiving the support from management in patient safety, referred to as 42.7%.
It is significant to take into account the managerial action that must continuously stimulate and motivate the operating personnel through actions that lead to promoting patient safety. In addition to taking the approach of the quality management model in health with a culture that favors the implementation of an organizational change.
Due to the results found, it is recommended that this information be taken into account to create strategies that allow the development of a work environment where there is a culture of safe care. At the same time, motivate and make staff aware of behaviors committed to patient safety.
Likewise, the opportunities for improvement in the dimensions are a guideline to assess compliance with safe practices in the various processes and procedures that take place in the hospital. Nursing staff is the one that stays the longest in patient care, so they can perceive when AEs occur that have to do with the care that is being provided. Therefore, knowledge of the culture of patient safety and the quality by which care is provided is essential.
It is important to continue researching patient safety in a hospital care to reduce risks, as well as errors in patient care that can cause deterioration in health, disability or death, it is also necessary to sensitize hospital management to that a series of strategies be developed in a shared commitment with the staff to improve the culture of patient safety.
REFERENCIAS
1. Organización Mundial de la Salud (OMS). Seguridad del paciente [Internet]. OMS. Septiembre 2019. [consultado en octubre, 2020]. Disponible en: https://www.who.int/es/news-room/fact-sheets/detail/patient-safety [ Links ]
2. Waterson P, Carman E-M, Manser T, Hammer, A. Hospital Survey on Patient Safety Culture (HSPSC): a systematic review of the psychometric properties of 62 international studies. BMJ open [Internet]. 2019 [consultado en marzo 2021]; 9: e026896. Disponible en: https://bmjopen.bmj.com/content/bmjopen/9/9/e026896.full.pdf [ Links ]
3. Okuyama, JHH, Galvao TF, Silva, MT. Healthcare professional's perception of patient safety measured by the hospital survey on patient safety culture: a systematic review and meta-analysis. The Scientific World Journal [Internet]. 2018 [consultado en abril 2021); vol (2018). https://downloads.hindawi.com/journals/tswj/2018/9156301.pdf [ Links ]
4. Villalonga N, Hidalgo W, Diaz S, Mansilla C, Stremel JL, Halac, A. Metas internacionales para la seguridad del paciente. Intervenciones de Enfermería en la mejora en la atención del niño internado. Med. Infant. [internet]. 2019 [consultado en octubre 2020]; 26 (3): 304-309. Disponible en: https://www.medicinainfantil.org.ar/images/stories/volumen/2019/xxvi_3_304.pdf [ Links ]
5. Melchor NM, Ramírez AM, Pérez TOR, Abad JAS, García AMV, Santos FS. et al. Conocimiento de las "Metas Internacionales para la Seguridad del Paciente" en personal que labora en un hospital de pediatría de tercer nivel de atención. Enfermedades Infecciosas y Microbilogía, [Internet]. 2020 [consultado en febrero 2021]; 39(1), 12-18. Disponible en: https://www.medigraphic.com/cgibin/new/resumen.cgi?IDARTICULO=92156 [ Links ]
6. Achury D, Rodríguez S, Díaz JC, Gómez J, Gómez A, Díaz JE. et al. Caracterización de los eventos adversos reportados por enfermería en unidades de cuidado intensivo en Bogotá (Colombia). Revista Salud Uninorte, [Internet]. 2017[consultado en septiembre 2020]; 33(2), 105-117. Disponible en: https://www.redalyc.org/pdf/817/81753189005.pdf [ Links ]
7. Moreno B, Febré N. Efecto de un programa de intervención educativa sobre el conocimiento de seguridad de pacientes en estudiantes de pregrado de enfermería. Ciencia y enfermería, [Internet]. 2017[consultado en diciembre 2019]; 23(1), 97-108. Disponible en: https://scielo.conicyt.cl/scielo.php?pid=S071795532017000100097&script=sci_arttext&tlng=n [ Links ]
8. Leblanch TIF, Solis SS, Castillo JB, Cespedes MEG, Difour MVF. Acreditación hospitalaria una transformación necesaria. Revista Cubana de Tecnología de la Salud [internet]. 2021[consultado en agosto 2021]12(2), 199-210. Disponible en: http://www.revtecnologia.sld.cu/index.php/tec/article/view/1920 [ Links ]
9. Martínez CR, Aguedo J, Areiza SM, Giraldo PDM. Seguridad del paciente y su percepción en los profesionales de la salud. Civilizar Ciencias Sociales y Humanas [internet]. 2017[consultado en septiembre 2020] 17(33), 277-291. Disponible en: https://dx.doi.org/10.22518/usergioa/jour/ccsh/2017.2/a17 [ Links ]
10. Rodríguez DEC, Carvajal NEJ. Cultura de seguridad del paciente en enfermeros de atención primaria. Rev cubana Enferm [Internet].2018[consultado en junio 2020] 34(1). Disponible en: http://www.revenfermeria.sld.cu/index.php/enf/article/view/1245 [ Links ]
11. Hessels AJ, Paliwal M, Weaver SH, Siddiqui D, Wurmser TA. Impact of Patient Safety Culture on Missed Nursing Care and Adverse Patient Events. J Nurs Care Qual. 2019 oct/Dec;34(4):287-294. doi: 10.1097/NCQ.0000000000000378. PMID: 30550496; PMCID: PMC6561834. [ Links ]
12. Rocco C, Garrido A. Seguridad del paciente y cultura de seguridad. Revista Médica Clínica Las Condes [Internet]. 2017. [Consultado diciembre del 2020] 28(5), 785-795. Disponible en: https://doi.org/10.1016/j.rmclc.2017.08.006 [ Links ]
13. Farokhzadian J, Dehghan N, Borhani F. The long way ahead to achieve an effective patient safety culture: challenges perceived by nurses. BMC Health Serv Res. 2018 Aug 22;18(1):654. doi: 10.1186/s12913-018-3467-1. PMID: 30134980; PMCID: PMC6106875. doi: 10.1186/s12913-018-3467-1 [ Links ]
14. Maldonado XAN, Nascimento ERPD, Lazzari DD. Profesionales de enfermería y la notificación de los eventos adversos. Texto Contexto Enferm [Internet]. 2020. [consultado en junio 2021] 29 e20190282. Disponible en: https://www.scielo.br/j/tce/a/psgyFmjZRFRkZ89B9k6PKqd/?lang=es&format=html [ Links ]
15. Sosa EA, Montes MED, Beltrán L.P.P. Sistema de gestión del conocimiento para la seguridad del paciente y análisis de eventos adversos en IPS, profesionales independientes y transporte asistencial. CIFE: Lecturas de Economía Social [Internet]. 2021. [consultado agosto 2021]; 23(38). Disponible en: https://doi.org/10.15332/22484914.613416. [ Links ]
16. Gascón-Cánovas, J. J., Saturno-Hernández, P. J., Pérez-Fernández, P., Vicente-López, I., González-Vicente, A., Martínez-Mas, J. (2005). Cuestionario sobre seguridad de los pacientes: versión española del Hospital Survey on Patient Safety. Madrid: Ministerio de Sanidad y Consumo. https://www.mscbs.gob.es/organizacion/sns/planCalidadSNS/docs/CuestionarioSeguridadPacientes1.pdf [ Links ]
17. Martínez Reyes, C. R., Agudelo Durango, J., Areiza Correa, S. M. Giraldo Palacio, D. M. Seguridad del paciente y su percepción en los profesionales de la salud. Civilizar ciencias sociales y humanas. 2017;17(33), 277-291. https://doi.org/10.22518/usergioa/jour/ccsh/2017.2/a17 [ Links ]
18. Maya, A. M. S., & Marin, D. M. R. Patient Safety Culture Observed at Six Surgical Centers in Antioquia, Colombia/Cultura de la seguridad del paciente en seis centros quirúrgicos de Antioquia/Cultura da seguranca do paciente em seis centros cirurgicos em Antioquia. Revista Cuidarte. 2020;11(2), NA-NA. http://dx.doi.org/10.15649/cuidarte.1040 [ Links ]
19. Pérez L. Evaluación de la cultura de seguridad del paciente en un quirófano. Rev cubana de enfermer. [Internet].2017. [consultado en diciembre 2020]; 33(2):348-60. Disponible en: http://scielo.sld.cu/pdf/enf/v33n2/enf15217.pdf [ Links ]
20. Santiago-González N, Morales-García D, Ibarra-Cerón M, López-Jacinto E. Cultura de seguridad del paciente en un hospital de alta especialidad. Rev de Enferm. Neurol. [Internet]. 2019. [consultado en diciembre 2020]; 18(3), 115-123. Disponible en: https://www.revenferneurolenlinea.org.mx/index.php/enfermeria/article/view/288/310 [ Links ]
21. Okuyama J, Galvão T, Crozatti, M, Silva, M. "Health professionals' perception of patient safety culture in a university hospital in São Paulo: A cross-sectional study applying the Hospital Survey on Patient Safety Culture." Sao Paulo Medical Journal. [Internet]. 2019 [ consultado en marzo 2020]; 137 (3), 216-222. https://www.scielo.br/j/spmj/a/rNSjsjkvkBS3bh4C9zKJNrg/?format=pdf&lang=en [ Links ]
22. Ramírez-Martínez M, González A. Cultura de seguridad y eventos adversos en una clínica de primer nivel. Enfermería universitaria [Internet]. 2017. [consultado en septiembre 2020] 14(2), 111-117. Disponible en: http://dx.doi.org/10.1016/j.reu.2017.02.006 [ Links ]
23. Ramírez de Ángel V, Pérez Castro, Vázquez J. Percepción de la cultura de seguridad del paciente en el Hospital Ángeles Metropolitano, mediante la aplicación de la encuesta de la Agencia para la Investigación Sanitaria y la Calidad (AHRQ), por sus siglas en inglés. Acta méd. Grupo Ángeles [revista en la Internet]. 2021 jun [citado 2022 Abr 17]; 19(2): 195-203. Disponible en: http://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S1870-72032021000200195&lng=es. Epub 23-Nov-2021. https://doi.org/10.35366/100442. [ Links ]
24. Tejada HS, Ayala B, Minchola SE. Seguridad del paciente hospitalizado en Essalud. ACC CIETNA: Revista de La Escuela de Enfermería. [Internet]. 17 de diciembre de 2020 [citado 17 de abril de 2022];7(2):85-92. Disponible en: https://revistas.usat.edu.pe/index.php/cietna/article/view/410 [ Links ]
25. Cruz J, Walit J, Veloza MC. La seguridad del paciente en un hospital de Bogotá, percepción del profesional de Enfermería. Investig. Andin. [Internet]. 2019. [consultado en noviembre 2020]; 21(39), 9-20. Disponible en: https://doi.org/10.33132/01248146.1552 [ Links ]
26. Fonseca-Mesa DA, Serpa-Pérez PC, Arias-Botero JH. Clima de seguridad del paciente en cuatro servicios quirúrgicos de Santander. Salud UIS[Internet]. 2021. [consultado en octubre 2020]; 53. Disponible en: https://revistas.uis.edu.co/index.php/revistasaluduis/article/view/10959/11325 [ Links ]
27. Rivas MS, Cardoso CN, Mella R, Giler SM. Análisis de la carga laboral del personal de enfermería, según gravedad del paciente. Rev cubana de enfermer. [Internet]. 2018. [consultado en diciembre 2020]; 34(2). Disponible en: http://revenfermeria.sld.cu/index.php/enf/article/view/2170/366 [ Links ]
28. Boussat B, Kamalanavin K, François P. The contribution of open comments to understanding the results from the Hospital Survey on Patient Safety Culture (HSOPS): A qualitative study. PLoS ONE[Internet].2018. [consulted in October 2020]; 13(4): e0196089. Available in: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0196089 [ Links ]
29. Macedo S M, Almeida A R, Borges F, Crozeta K, Peres A M, Assis F. Cultura de seguridad del paciente: evaluación de los enfermeros en la atención primaria a la salud. Enferm. glob. [Internet]. 2019 [citado 2021 Jul 19]; 18(56): 365-397. Disponible en: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1695-61412019000400013&lng=es. Epub 23-Dic-2019 [ Links ]
30. Ornelas PT. Cultura de la seguridad del paciente en hospitales de los servicios de salud del estado de Colima. Boletín Conamed [Internet]. 2018. [consultado en octubre 2020] 18 Disponible en: http://www.conamed.gob.mx/gobmx/boletin/pdf/boletin18/cultura_seguridad.pdf [ Links ]
Received: July 09, 2022; Accepted: November 10, 2022
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
