










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.22 no.71 Murcia jul. 2023 Epub 13-Nov-2023
https://dx.doi.org/10.6018/eglobal.554501
Originals
Face-to-face classes during COVID-19: implementation of school health protocols
1Graduate in Nursing. Assisstant Professor. Basic Nursing Department. Universitas Pendidikan Indonesia
2Graduate in Nursing. Assisstant Professor. Medical Surgical Nursing Department. Universitas Pendidikan Indonesia
3Graduate in Nursing. Assisstant Professor. Disaster Nursing Department. Universitas Pendidikan Indonesia
4Graduate in Nursing. Assisstant Professor. Pediatric Nursing Department. Universitas Pendidikan Indonesia
Introduction:
The opening of schools increases the likelihood of an increase in COVID-19 cases, and to prepare for this, schools must begin to create various checklists, as indicated in the Joint Decree of Four Ministers on Guidelines for Implementing Learning During the COVID-19 Pandemic. Safe school openings are possible provided sufficient planning and mitigation are implemented, such as through the use of accepTable school opening guidelines.
Objective:
The purpose of this study is to examine the compliance of school health protocols during COVID-19 in West Java, Indonesia, as well as the differences between participants.
Methods:
A quantitative cross-sectional study was conducted in an elementary school in West Jawa, Indonesia. Using a structured instrument, modified from Panduan Penyelenggaraan Pembelajaran di Masa Pandemi Covid-19 (Guidelines for Implementing Learning During the Covid-19 Pandemic) by the researchers, containing school characteristics, availability of sanitation infrastructure, hygiene and health facilities, canteen availability, and Behavior of maintaining health protocols in schools with 27 questions: 11 availability of sanitation, hygiene, and health facilities, canteen availability, and Behavior of maintaining health protocols in schools The study involved 347 individuals from 29 primary schools. SPSS software and the Kruskal-Wallis non-parametric test were used to examine the study hypotheses.
Result:
The mean score on sub-variable availability of sanitation infrastructure, cleanliness, and health facilities was high (27.49/5.391). The three sub-variables that were tested were different based on the participant's assessment, only the canteen availability sub-variable had no difference in the mean score between the participants, the value of Sig =.255, which is more than 0.05.
Conclusion:
The study's findings revealed that the introduction of health protocols in primary schools during face-to-face learning was effective, with a high average total score.
Keywords: face-to-face classes; elementary school; health protocol; COVID-19; Return to school
INTRODUCTION
After nearly 18 months of school closures to lower the prevalence of COVID-19 transmission, WHO and UNICEF advise schools in Indonesia to resume face-to-face learning as soon as possible (1). The reopening of schools must be done as soon as possible, given that COVID-19 cases in Indonesia are beginning to drop and the extended duration of distance learning creates several physical and emotional challenges (2),(3). Distance learning can also raise the risk of long-term interpersonal stress and social isolation throughout adolescence (4). Based on these factors, the Republic of Indonesia's government has decreed that restricted face-to-face learning would begin in January 2022, with numerous restrictions that must be followed by all educational institutions (5).
The opening of schools increases the likelihood of an increase in COVID-19 cases, and to prepare for this, schools must begin to create various checklists, as indicated in the Joint Decree of Four Ministers on Guidelines for Implementing Learning During the COVID-19 Pandemic. Safe school openings are possible provided sufficient planning and mitigation are implemented, such as through the use of accepTable school opening guidelines (6). Back-to-school initiatives must review and ensure the education system's preparation for school reopening, including infrastructure, teaching staff, pedagogy, students and their families; learning continuity; and system resilience to foresee and cope with future crises (7). One of the things that the school must prepare is the Health Protocol. The health protocols that must be implemented are as follows: a) use a mask under the provisions, namely covering the nose, mouth, and chin; b) maintain a distance of at least 1 (one) meter between people and/or between chairs/Tables; c) avoid physical contact; d) do not borrow each other's equipment or learning supplies; e) do not share food and drink, and do not eat and drink together face to face and close together; f) apply coughing and sneezing etiquette; and g) regular hand sanitizing (8).
Teachers have not adequately executed health procedures during restricted face-to-face learning in primary schools, which focused on wearing masks appropriately and correctly, washing hands, and keeping distance (9), despite the fact that schools are an excellent location to teach students the discipline of wearing masks (10). There is still a lack of awareness of the key tasks of the COVID-19 task force in schools; there has been no official covid-19 task force coaching; coaching is only available through social media and self-taught; Human resources are still scarce when it comes to adopting health regulations in face-to-face learning in schools (11). This is most likely the reason of the threefold spike in COVID-19 cases, or roughly 6000 cases, in August 2022 (12).
Face-to-face learning should begin with five critical considerations: reopening schools in phases, keeping physical and social distance, managing infections using testing and tracking accessible in schools, protecting children and instructors, and doing research and assessment (13). Starting with the pre-condition stage, timing, priorities, central-regional cooperation, and monitoring and evaluation, the process of opening schools in Indonesia is carried out in stages (12). Based on a survey conducted by Fitriah et al.(2020) that The majority of principals, teachers, parents, and education offices are ready to implement face-to-face learning in all aspects, including implementing health protocols during face-to-face learning, but the condition of supporting facilities and infrastructure is still inadequate, including poor health data collection. Although, clinically, children (1-18 years old) exhibit moderate symptoms or no symptoms due to COVID-19, the number of hospitalized children is likewise minimal and no more infectious than adults (15)-(18), Because students, teachers, and other school residents contact in schools, the transmission of this disease must be monitored. This condition produces concern in both students' parents and instructors. Furthermore, parents of students are concerned that their children may spread the disease to their family at home (19). The reopening of schools during the pandemic has also created concern among parents and teachers because to the possibility of COVID-19 transmission in schools, where students often contact with a large number of individuals (20).
During an era of ongoing communicable disease outbreaks, nurses serve as a valuable resource in preventing and responding to threats to the health of school populations by teaching prevention and basic but important precautions, with a focus on respiratory and hand hygiene, as well as other important precautions, due to the vital roles they play in communication between students, school personnel, and public health officials (21). Therefore, nurses have an obligation to participate in overcoming the spread of COVID-19 in school clusters (22).
Based on this description, it is required to evaluate the application of health protocols during face-to-face learning, which has been underway for roughly 2 months, to serve as a foundation for anticipating the expansion of COVID-19 in school clusters.
OBJECTIVE
To ascertain the adoption of school health protocols during COVID-19 in West Java, Indonesia, as well as the variations in implementation of school health protocols during COVID-1 across participants.
METHODS
Ethical aspect
The study was carried out in compliance with national and international ethical rules and was authorized by the Research Ethics Committee of Universitas Pendidikan Indonesia's Centre of Research and Community Services, whose opinion is attached to this submission. All participants engaged in the study provided written free and informed consent. All study data were kept confidential and coded, with only the research team having access to it. The participants were not named in the published findings.
Design, period and place of study
This is a cross-sectional design research based on data from 29 primary school principals, teachers, and students. STROBE-Strengthening the Reporting of Observational Studies in Epidemiology was used to report the methodological processes. Participants were sought in August 2022 from 29 primary schools in West Java, Indonesia.
Population or sample
The cross-sectional survey was carried out between August 6 and 10, 2022. The school principals, teachers assigned as the person in charge of the health-promoting school, and students who met the inclusion criteria of (1) being male or female, (2) being in 5th or 6th grade, and (3) being able to self-report by completing an anonymous survey questionnaire were the study's target population. The attendees included all of the school administrators and instructors, for a total of 58 people. The minimal sample size for students was 290, which was gathered from a total student population of 792 pupils in grades 5 and 6 who were deemed capable of filling out questionnaires provided by researchers and calculated based on the slovin formula.
Study protocol
First, a structured instrument was used, which was adopted by the researchers from Panduan Penyelenggaraan Pembelajaran di Masa Pandemi Covid-19 (Guidelines for Implementing Learning During the Covid-19 Pandemic) and included school characteristics, sanitation infrastructure availability, cleanliness and health facilities, cafeteria availability, and behaviour of maintaining health protocols in schools. To represent the degree of implementation on a Likert-type scale ranging from one to two, one to three, and one to four.
The guidelines questions took about 15 minutes to complete separately. The tool displays self-reported implementation. It consisted of 11 questions on the availability of sanitary infrastructure, cleanliness, and health facilities, 8 questions about the availability of canteens, and the last 8 about the behaviour of keeping health protocols in schools.
The correlation value between the item score and the overall score of the scale is used in the validity test utilizing item-total correlation, also known as correlations Pearson product moment. The value of the item-total correlation for item number 28 is the correlation of the subject's score in item number 28 with the subject's overall score on the scale. The validity test concludes that the entire variable item is valid because its significance value is less than 0.05 (0.05). Alpha-beta reliability tests Cronbach's alpha coefficient was.873, indicating that the instrument used to acquire the data is extremely reliable. The overall score ranged from 27 to 104 (the availability of sanitary infrastructure ranged from 11 to 43, hygiene and health facilities ranged from 8 to 30, and canteen availability was from 8 to 32).
Analysis of results and statistics
The data was tabulated and verified in pairs to correct any typing errors before being analyzed with the IBM SPSS Statistics Subscription Trial. First, descriptive statistics were computed for numerical variables using measures of central tendency (mean, standard deviation minimum, maximum) and proportions for categorical variables.
Furthermore, SPSS software and the Kruskal-Wallis nonparametric test were used to examine the study hypotheses.
RESULTS
Demographic data
This research looked at descriptive information regarding the features of the schools studied. As shown in Table 1, the highest percentage is associated with schools that implemented face-to-face learning during the pandemic (99.7%), while the lowest percentage is related to schools that implemented blended learning and online learning (0%). Learning occurs practically every day (97.8%), and almost all learning time (85%) is spent in line with the school curriculum (Table 1)

Descriptive analysis
The mean score on sub-variable availability of sanitation infrastructure, cleanliness, and health facilities was high (27.49/5.391), with the evaluation of teacher participants yielding the highest mean score (30.52/4.808). Canteen availability has a mean score of 18.84 (4.094), with teacher participants receiving the highest score (19.45/4.298). The last sub-variable, behaviour of adhering to health guidelines, had a mean score of 20.89 (4.641), with the principal's participants having the highest mean score (22.93/4,363) Table 2.
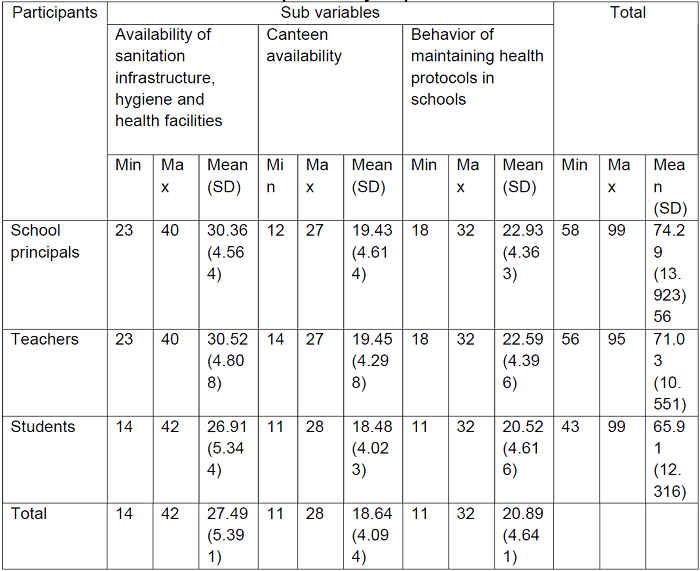
Overall, from highest to lowest, the evaluation of the implementation of health protocols in face-to-face learning is an assessment of principal participants 74.29 (13.923), an assessment of teacher participants 71.03 (10.551), and an assessment of student participants 65.91. (12.316).
Comparison analysis
Hypothesis 1: There is a considerable difference in participants' availability of sanitary infrastructure, hygiene, and health facilities. The Kruskal-Wallis test was performed to test the above hypothesis, and the results are shown in the Table below: As shown in Table 3, the value of Sig = <.001, which is less than 0.05, is less than 0.05.
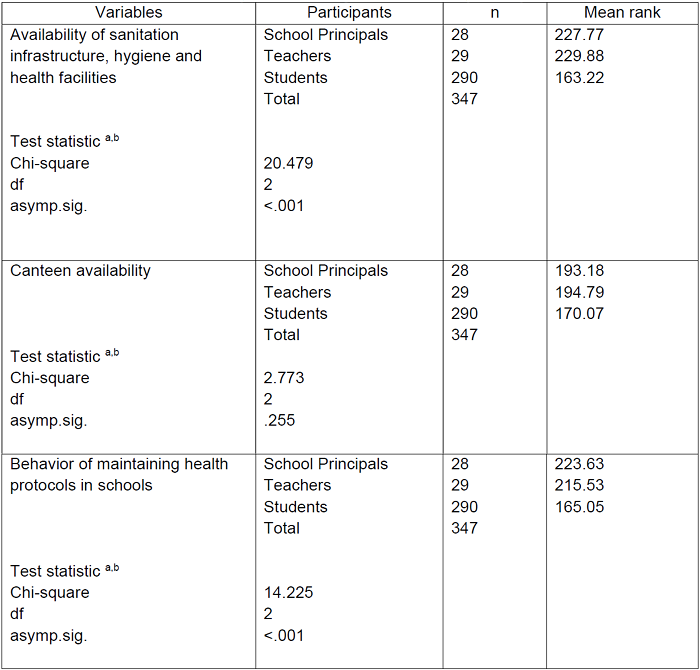
Hypothesis 2: There is no statistically significant variation in Canteen availability among participants. The Kruskal-Wallis test was performed to test the above hypothesis, and the results are shown in the Table below: As shown in Table 3, taking into account the value of Sig =.255, which is more than 0.05.
Hypothesis 3: There is a considerable difference in the behavior of participants in sustaining health protocols in schools. The Kruskal-Wallis test was performed to test the above hypothesis, and the results are shown in the Table below: As can be seen in Table 3, the value of Sig =.255 is more than 0.05.
DISCUSSION
In general, learning in elementary schools has been almost entirely conducted face-to-face in the classroom, under the Joint Decree of the Four Ministers, which states that beginning with the 2022-2023 school year, odd semesters of learning have been allowed face-to-face by paying attention to the state of the school area at levels 1 and 2 of the PPKM (Implementation of Community Activity Restrictions) and paying attention to strict health protocols(23). Learning is carried out every day (6 days per week) with a learning duration that is under the curriculum. Only a tiny fraction of schools plan to learn in an alternate method (3 days per week) with a maximum learning time of 6 hours per day or not in compliance with the curriculum. This is because face-to-face learning is tailored to the capability of classrooms and teachers, hence some schools cannot conduct 100% face-to-face learning (24).
The application of health protocols in face-to-face learning is separated into three sub-variables: sanitation infrastructure availability, cleanliness and health facilities, cafeteria availability, and behaviour of maintaining health protocols in schools. The average value per sub-variable is relatively high in general. This is because the school has begun to prepare health protocol infrastructure long before the implementation of face-to-face learning is fully implemented to ensure that the school remains a safe place for everyone to learn and that thorough planning and preparation are undertaken by the principal, teachers, students, parents, and other school personnel (25). Schools must also carefully plan for the reopening of schools and alter existing buildings and infrastructure to meet the defined requirements that are required for schools to reopen(26).
The assessment of the teacher in charge of health protocols in the school or the teacher of a health-promoting school delivers the highest average score of the first sub-variable, while the assessment of students generates the lowest average score. The lowest score on this sub-variable is on question item number 10, which concerns the availability of the Peduli Lindungi QRCode at the school's entrance and departure. Almost many schools lack the Peduli Lindungi QRCode as a way of tracing people who enter a public location, including schools, although obtaining the QRCode is simple; every school registers to receive the QRCode online (27). QRCode Peduli Lindungi is also a government initiative to restrict the spread of COVID-19, thus public facility managers should be aware of this (28).
In the second sub-variable on the administration of school cafeterias during the COVID-19 pandemic, teachers in charge of health procedures in schools have the highest average assessment and school students have the lowest. The question item with the fewest scores is number 12, which is about the capacity of the canteen that has been opened 100%, implying that practically all school canteens have been opened properly and the school cafeteria is rarely cleaned regularly. The school cafeteria has been closed for a long time, and the school finally feels ready to reopen the canteen; however, some schools are not ready to open the canteen, so the practicality of the canteen is questionable (29).
The last sub-variable in this study, school health protocol conduct, received the highest average score from the principal's assessment. Question item number 25 has the lowest score of all the question items in this sub-component. This item inquires about the practice of eating together and facing each other without keeping their distance, implying that many students still do not retain their distance and face each other when eating and drinking. This is possible since the school cafeteria has begun to open completely, resulting in crowds when purchasing and enjoying meals from the canteen, as the canteen is also a source of crowds that must be considered when the school opens (25).
In this study, researchers also investigated the differences in each sub-variable based on participants to reach the results: there were differences in sub-variables of availability of sanitation infrastructure, cleanliness, and health facilities based on participants, which suggests that the evaluation between participants in this variable differs from one another. There is no variation in the Canteen availability sub-factors per participant, implying that participants' assessments of these sub-variables are the same. Furthermore, there are variances in the evaluation of sub-variables of the behaviour of maintaining health protocols in schools based on participation, implying that the assessment of these sub-variables varies between one set of participants and another. The equation of the assessment of canteen capacity by each set of participants demonstrates that the research instruments utilized are fairly reliable.
Limitation of the study
The limitation of this study is that data gathering is not directly observed by the researcher, thus the correctness of the data collected from the outcomes of participants filling out the questionnaire cannot be cross-tested.
Contributions to nursing and health
The findings of this study help to broaden nurses' understanding of health promotion as part of nursing intervention, particularly in health-promoting schools.
CONCLUSION
In this study, administrators, instructors, and students evaluated the adoption of health protocols during face-to-face learning in primary schools. The study's findings revealed that the introduction of health protocols in primary schools during face-to-face learning was effective, with a high average total score. Participants' judgments of the availability of sanitation infrastructure, cleanliness, and health facilities varied, as do their assessments of the third sub-variable, the behaviour of upholding health protocols in schools. Meanwhile, there is no variation in evaluation for the second sub-variable, canteen availability.
REFERENCES
1. UNICEF. [Indonesia: 18 months after schools close, it's time for children to return to school safely as soon as possible] [Internet]. Unicef Indonesia. 2021 [cited 2022 Aug 7]. Available from: https://www.unicef.org/indonesia/id/press-releases/indonesia-18-bulan-setelah-sekolah-ditutup-kini-waktunya-anak-anak-kembali-ke [ Links ]
2. Kartika M, Muhammad H. [Active cases of Covid-19 in Indonesia decreased by 65.81 Percent] [Internet]. Republika. 2021 [cited 2022 Aug 7]. Available from: https://sindikasi.republika.co.id/berita/qyqzs7380/kasus-aktif-covid19-di-indonesia-turun-6581-persen [ Links ]
3. Chaabane S, Doraiswamy S, Chaabna K, Mamtani R, Cheema S. The impact of COVID-19 school closure on child and adolescent health: A rapid systematic review. Children [Internet]. 2021;8(5):1-17. Available from: https://doi.org/10.3390/children8050415 [ Links ]
4. Magson NR, Freeman JYA, Rapee RM, Richardson CE, Oar EL, Fardouly J. Risk and protective factors for prospective changes in adolescent mental health during the COVID-19 pandemic. J Youth Adolesc. 2021;50(1):44-57. https://doi.org/10.1007/s10964-020-01332-9 [ Links ]
5. Kemdikbud RI. [Joint decree of 4 ministers guiding the implementation of learning during the Covid-19 pandemic] [Internet]. Pengelola Web Kemdikbud, 05/KB/2021 Indonesia; 2021 p. 1-70. Available from: https://www.kemdikbud.go.id/main/blog/2021/12/keputusan-bersama-4-menteri-tentang-panduan-penyelenggaraan-pembelajaran-di-masa-pandemi-covid19 [ Links ]
6. Irfan O, Li J, Tang K, Wang Z, Bhutta Z. Risk of infection and transmission of SARS-CoV-2 among children and adolescents in households, communities and educational settings; A systematic review and meta-anaysis. J Glob Health. 2020;311(05013):539-47. https://doi.org/10.7189/jogh.11.05013 [ Links ]
7. UNESCO. COVID-19 education response webinar back to school: Preparing and planning for the reopening of schools [Internet]. 2020. Available from: https://en.unesco.org/covid19/educationresponse [ Links ]
8. Kemdikbud. [Guidelines for implementing learning during the COVID-19 pandemic] [Internet]. 1st ed. Vol. 2019, Kemendikbud. Jakarta, Indonesia: Kemdikbud RI; 2020. 1-58 p. Available from: https://www.kemdikbud.go.id/main/blog/2020/06/buku-saku-panduan-pembelajaran-di-masa-pandemi-covid19 [ Links ]
9. Ardillah Y, Septiawati D, Windusari Y. [Readiness of water sanitation hygiene (Wash) facilities and implementation of health protocols for teaching staff during the Covid-19 pandemic at Palembang State Elementary Schools]. J Ekol Kesehat. 2021;20(1):1-11. https://doi.org/10.22435/jek.v20il.4525 [ Links ]
10. Esposito S, Principi N. To mask or not to mask children to overcome COVID-19. Eur J Pediatr. 2020;27:9-12. https://doi.org/10.1007/s00431-020-03674-9 [ Links ]
11. Sukaesih NS, Hudaya AP, Pramajati H, Sopiah P, Lindayani E. [Strengthening COVID-19 health protocols ahead of face-to-face learning in elementary schools (SD) for teachers in Cimalaka District]. J Pengabdi Pada Masy. 2022;7(2):469-82. https://doi.org/10.30653/002.202272.96 [ Links ]
12. Satgas Penanganan COVID-19. [School opening must go through 5 stages - handling Covid-19] [Internet]. Covid19.go.id. 2021 [cited 2022 Aug 8]. Available from: https://covid19.go.id/p/penanganan-covid-19/pembukaan-sekolah-harus-melalui-5-tahapan [ Links ]
13. Viner RM, Mytton OT, Bonell C, Melendez-Torres GJ, Ward J, Hudson L, et al. Susceptibility to SARS-CoV-2 infection among children and adolescents compared with adults: A systematic review and meta-analysis. JAMA Pediatr [Internet]. 2021 Feb 1 [cited 2021 Mar 28];175(2):143-56. Available from: https://pubmed.ncbi.nlm.nih.gov/32975552/ https://doi.org/10.1001/jamapediatrics.2020.4573 [ Links ]
14. Fitriah A, Solihin L, Purnama J, Hijriani I, Widjaya I. School reopening readiness during COVID-19 pandemic : a perspective of education stakeholders. J Anal Kebijak. 2020;4(2):40-53. https://doi.org/10.37145/jak.v4i2.467 [ Links ]
15. Cevik M, Bamford A, Ho A. COVID-19 pandemic- a focused review for clinicians. Eur Soc Clin Microbiol Infect Dis. 2020;2020(26):842-7. https://doi.org/10.1016/s2213-2600(20)30152-1 [ Links ]
16. Goldstein E, Lipsitch M, Cevik M. On the effect of age on the transmission of SARS-CoV-2 in households, school, and the community. J Infect Dis. 2021;2021(223):362-9. https://doi.org/10.1093/infdis/jiaa691 [ Links ]
17. Whittaker E, Bamford A, Kenny J, Kaforou M, Jones C., Shah P, et al. Clinical characteristics of 58 children with a paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2. African J Thorac Crit Care Med. 2020;26(3):259-69. https://doi.org/10.7196/ajtccm.2020.v26i3.113 [ Links ]
18. Dufort EM, Koumans EH, Chow EJ, Rosenthal EM, Muse A, Rowlands J, et al. Multisystem inflammatory syndrome in children in New York State. N Engl J Med. 2020;383(4):347-58. https://doi.org/10.1056/nejmoa2021756 [ Links ]
19. Wijaya AS, Riyadi A. [Increased family knowledge in reducing parental anxiety in preparing for children's schools in the new normal period of COVID-19]. J Pengabdi Kpd Masy PUSTINGKIA. 2022;1(1):1-8. https://doi.org/10.33088/jpustingkia.v1iI.107 [ Links ]
20. Wakui N, Abe S, Shirozu S, Yamamoto Y, Yamamura M, Abe Y, et al. Causes of anxiety among teachers giving face-to-face lessons after the reopening of schools during the COVID-19 pandemic: a cross-sectional study. BMC Public Health. 2021;21(1):1-10. https://doi.org/10.1186/s12889-021-11130-y [ Links ]
21. Fritsch K, Heckert KA. Working together: Health promoting schools and school nurses. Asian Nurs Res (Korean Soc Nurs Sci) [Internet]. 2007;1(3):147-52. Available from: http://dx.doi.org/10.1016/S1976-1317(08)60017-1 [ Links ]
22. Alexandropoulou M. The health promoting school and the school nurse: A content analysis of school staff's views. Br J Sch Nurs. 2013;8(3):134-41. https://doi.org/10.12968/bjsn.2013.8.3.134 [ Links ]
23. Kemdikbud. [Joint Decree of 4 latest ministers regulates one hundred percent face-to-face learning] [Internet]. 2022. 2022 [cited 2022 Aug 16]. Available from: https://www.kemdikbud.go.id/main/blog/2022/05/skb-4-menteri-terbaru-atur-pembelajaran-tatap-muka-seratus-persen [ Links ]
24. Malihah E. New challenges of face-to-face Learning [Internet]. 2022. 2021 [cited 2022 Aug 16]. Available from: https://mediaindonesia.com/opini/452733/tantangan-baru-pembelajaran-tatap-muka [ Links ]
25. CDC. Operational strategy for K-12 schools through phased prevention [Internet]. 2021 [cited 2021 Mar 28]. Available from: https://www.cdc.gov/coronavirus/2019-ncov/community/schools-childcare/operation-strategy.html [ Links ]
26. Kusumawardani A, Nina Alfa Rizkana. Parental perception and anxiety facing reopening school in Indonesia during the pandemic Covid-19. Eur J Humanit Educ Adv [Internet]. 2021;2(12 SE-):1-10. Available from: https://www.scholarzest.com/index.php/ejhea/article/view/1531/1282 [ Links ]
27. Kemenkes RI. Here's how to get a PeduliLindungi QR code! [Internet]. 2021. 2021 [cited 2022 Aug 16]. p. 1-2. Available from: https://covid19.go.id/edukasi/materi-edukasi/ini-cara-dapat-qr-code-pedulilindungi [ Links ]
28. Rahman MZR. How appropriate is a Pedulilindungi in the era of a pandemic. Pustaka IlmuId [Internet]. 2022;2(4):1-8. Available from: http://pustakailmu.id/index.php/pustakailmu/article/view/124 [ Links ]
29. Hadi H, Triastanti RK, Anggraeni D, Nurwanti E, Lewis EC, Colon-Ramos U, et al. The role of the school food environment in improving the healthiness of school canteens and readiness to reopen post COVID-19 pandemic: A study conducted in Indonesia. J Public health Res. 2022;11(1):1-8. https://doi.org/10.4081/jphr.2021.2287 [ Links ]
Acknowledgement
All of the authors are grateful to the Sumedang Department of Education for assisting and granting permission to gather data for this study
Received: January 19, 2023; Accepted: April 18, 2023
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
