










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.22 no.71 Murcia jul. 2023 Epub 13-Nov-2023
https://dx.doi.org/10.6018/eglobal.555161
Originals
Neonatal mortality trends by region in Brazil, 2015-2019: an ecological study
1Nurse. Master in Public Health. Technical Responsible for the State Coordination of Women's Health of the State Department of Health of Amazonas (SES-AM), Amazonas, Brazil
2Nurse. PhD. student in Tropical Diseases at the Center for Tropical Medicine at the Federal University of Pará (UFPA). Assistant Professor I of the Bachelor's Degree in Nursing at the State University of Pará (UEPA), Altamira Campus, Pará, Brazil
3Nurse. PhD. in Sciences from the School of Nursing at the University of São Paulo/EEUSP. Adjunct Professor and Coordinator of the Professional Master's Program in Nursing in the Amazonian Context at the Federal University of Amazonas, Amazonas, Brazil
4Nurse. Master in Health, Society and Endemic Diseases in Amazon by the Federal University of Amazonas (UFAM/). Assistant Professor of the Bachelor's Degree in Nursing at the Federal University of Amazonas, Amazonas, Brazil
5Nurse. PhD. in Gynecology, Obstetrics, and Mastology by the Paulista State University (UNESP). Associate Professor of the Bachelor's Degree in Nursing at the Federal University of Paraíba (UFPB), Paraíba, Brazil
6Nurse. PhD. student in Tropical Diseases at the Tropical Medicine Center at the Federal University of Pará (UFPA). Assistant Professor I of the Medicine Course at the Federal University of Pará (UFPA), Altamira Campus, Pará, Brazil
Aim:
To analyze the trend of neonatal mortality in Brazil from 2015 to 2019 and its preventable causes.
Methods:
Ecological time-series study with data extracted from the Mortality Information System and Live Births Information System. Neonatal mortality rates were calculated overall and according to preventable causes. Trend analysis was performed by Prais-Winsten regression.
Results:
The overall neonatal mortality rate reduced from 8.78 in 2015 to 8.60 in 2019. Disparities in neonatal mortality rates were observed among regions, with higher rates in the northern (10.3/1,000) and northeastern (9.9/1,000) regions. The causes preventable by adequate care for pregnancy, delivery and neonatal care prevailed, together totaling 97.8% of neonatal deaths in the period. There was a decreasing trend in preventable causes due to adequate care of the newborn (p < 0.001).
Keywords: Neonatal Mortality; Mortality Registries; Ecological Studies; Time Series Studies
INTRODUCTION
Neonatal mortality is understood as deaths that occur between 0 and 27 days, subdivided into two categories: early neonatal deaths (0 to 6 days of life) and late neonatal deaths(1) (2) (3). The Neonatal Mortality Rate (NMR) is considered one of the most appropriate indicators to measure the quality of life, socioeconomic development, the level of social well-being of a population, as well as its access to health services in a given territory, therefore linked to the intersection of a set of biological, socioeconomic, and healthcare factors that may be directly involved with this phenomenon(4,5).
According to the World Health Organization (WHO), the NMR is an indicator that sensitively assesses the availability, use, and effectiveness of health care, especially the ones provided during the pregnancy-puerperal cycle, to the newborn and the child up to the first year of life, being a powerful instrument in the context of health situation analyzes to direct public policies in the maternal and child context(6).
In this context, Kropiwiec, Franco, and Amaral(7) claim that NMR is considerably lower in nations with a high Human Development Index (HDI). While countries with low HDI tend to have higher NMRs, showing that these mortality rates are linked to whether to factors related to human development and the conformation of health services that most often have a reduced standard of effectiveness due to the development conditions of a given territory.
Global estimates indicate there was a drastic reduction in the mortality of children under five years of age worldwide, with four million fewer deaths in 2015 compared to the year 2000(8). Therefore, it was possible to note that the NMR also suffered a considerable decrease in recent decades, jumping from 37 to 18 deaths per thousand live births (LB) in the interstice of 1990-2018 (9).
Regarding neonatal mortality, data from the World Health Organization (WHO) point to discrepancies in the NMR taking into account the distribution between developed, developing, and underdeveloped countries in the period from 1990 to 2019. The data reveal that in this period NMR of Canada, the US, the UK, and Japan were 3.4/1000 LB, 3.6/1000 LB, 2.6/1000 LB, and 0.9/1000 LB, respectively. While in Brazil, Bolivia, Guatemala, and Panama, the NMR was 8.5/1,000 LB, 14.9/1,000 LB; 12.7/1,000 NV, and 8.8/1,000 NV, respectively. On the other hand, countries like Pakistan and the Central African Republic presented NMR of 43.0/1,000 LB and NV; of 41.8/1,000 NV, respectively(10).
Specifically in Brazil, data reveal a reduction in NMR from 25.33/1,000 LB in 1990 to 8.5/1,000 LB in 2019. This reduction scenario is the result of intense institutional work by the Department of Health (DH) in recent decades with the implementation of major programs and agreements such as the Prenatal and Birth Humanization Program (PHPN), the Baby-Friendly Hospital Initiative (IHAC), the National Pact for the Reduction of Maternal and Neonatal Mortality and, more recently, in 2011 the Rede Cegonha Program, designed for the country to reach the 4th goal of the then Millennium Development Goals (MDGs), which was to reduce the infant mortality rate to two-thirds of the rate observed in 1990, a fact that achieved in the same year (10),(11)).
Despite notable advances in the reduction of neonatal mortality in Brazil over the years, it is salutary to highlight the existing discrepancies in NMR between the regions of the country, where the North and Northeast regions historically concentrate the highest rates concerning the other regions as a result of the social inequalities and iniquity in health that were historically constructed in the country, with the social determinants of health as the background of this context(12) (13) (14) (15). In addition, neonatal deaths, and especially preventable ones, are responsible for a portion of the deaths of children under five years, a fact that brings up the need to seek to analyze the health situation of each region, so that actions can be taken in a targeted manner to extinguish these preventable deaths.
In this way, knowing the NMR trend is necessary since Brazil is a signatory of the Sustainable Development Goals (SDGs) of the United Nations (UN), which foresees the eradication of neonatal mortality from preventable causes and reaching an NMR of 12 deaths per 1,000 LB by 2030 and understanding the phenomena involved with NMR over time can contribute to the analysis and direction of public policies related to the theme based on scientific evidence(16),(17). In addition, time series studies(15) can show atypical patterns in the evolution of morbidity and mortality rates of diseases and or conditions and the formation of their causes, a factor that allows assessing the impacts produced by targeted actions in a given context, in the present case on the possible modifiable determinants of neonatal mortality.
Thus, this study aims to analyze the trend of neonatal mortality in Brazil from 2015 to 2019 and its preventable causes.
MATERIAL AND METHOD
It's an ecological time-series study to assess the trend in the neonatal mortality rate in Brazil from 2015 to 2019. Ecological studies are relevant for analyzing the health situation of a community, having as a unit of study a particular geographic area. For Antunes and Cardoso(18), time series studies can be defined as a series of quantitative data related to specific moments which are studied according to their temporal distribution. These studies serve to monitor the health of populations, assess the risk of exposure of subjects to a certain injury, predict the occurrence of situations/events in health, provide elements for possible explanations of cause and effect, guide the analysis of the health situation to the development of actions, as well as evaluating the impacts generated by these interventions.
The data refer to neonatal deaths that occurred in Brazil from 2015 to 2019 and were extracted from the Mortality Information System (SIM) and the Live Births Information System (SINASC) through the Department of Informatics of the Unified Health System (DATASUS), public domain online platform of the Department of Health.
Analyzes of overall neonatal mortality rates and preventable deaths were performed. For the classification analysis of the avoidability of neonatal deaths, the Brazilian list of causes of death preventable by actions of the Unified Health System (UHS) was adopted. According to the list, avoidable causes are distributed in the following groups: 1) Reducible by immunoprevention actions; 2) Reducible by adequate care for women during pregnancy; 3) Reducible by adequate care during childbirth; 4) Reducible by adequate care for the newborn; 5) Reducible by appropriate diagnostic and treatment actions; 6) Reduced by adequate health promotion actions. Deaths from ill-defined causes and those from causes that were not preventable were excluded from the analysis(19),(20).
Data were extracted and organized in Excel spreadsheets. To calculate the NMR, the quotient between the number of deaths from 0 to 27 complete days, by place of residence, and the number of live births of resident mothers, multiplied by 1,000, was calculated. Neonatal mortality rates were calculated in the period and each year in Brazil and the geographic regions of the Brazilian Institute of Geography and Statistics (BIGS), as well as according to preventable causes in Brazil in the total of 5 years and every year.
To carry out the analysis of trends the Prais-Winsten linear regression method was used, which corrects the serial autocorrelation that usually occurs with population data, such as time series in epidemiology. To perform the screen regression method, the NMR was transformed into a logarithmic scale, to reduce the heterogeneity of the variance of the residues from the analysis of the time series(18). P = 0.05 was adopted as a critical value in determining the significance of the trend.
The regression results were interpreted and classified as follows: increasing linear trend when the p-value was less than 0.05 and the angular coefficient (beta) b1 was positive; decreasing linear trend when the value of p was less than 0.05 and the angular coefficient (beta) b1 was negative; stationary linear trend when the p-value was greater than 0.05. Data were processed using the R software version 4.0.0.
Because it is an ecological study and, therefore, without subjects, but population aggregates for analysis, it was not necessary to be evaluated by an ethics committee for research with human beings. Furthermore, the data is in the public domain and does not contain information about the identity of the participants or other sensitive information that could violate the secrecy of the data. Therefore, the precepts of Resolution No. 510 of 12/04/2016 of the National Health Council/Ministry of Health of Brazil were complied with.
RESULTS
During the period from 2015 to 2019, 181,231 infant deaths were recorded in Brazil, of which 70% (126,882) were neonatal. Almost 75.0% of neonatal deaths occurred from preventable causes. From 2015 to 2019, there was a reduction in preventable neonatal deaths by 1.2% (Table 1).
Table 1. Distribution of infant and neonatal deaths by year of death. Brasil, 2015 a 2019.
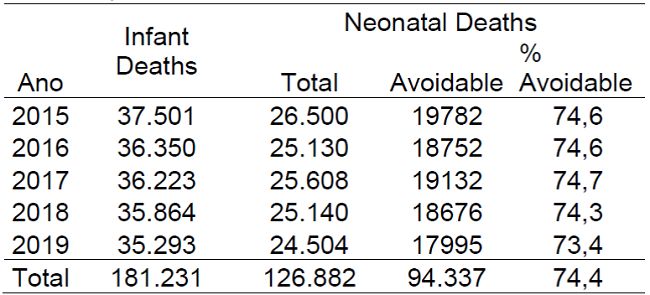
Source: Elaborated by the authors based on data from the Mortality Information System (MIS), 2022.
The average death rate in the period was 8.69 deaths per thousand live births. In general, there was a decrease in the neonatal mortality rate in Brazil, from 8.7/1,000 in 2015 to 8.6/1,000 live births in 2019, corresponding to a decrease of 0.18% (Table 2).
There was a decline in neonatal mortality rates in the Northeast region, from 10.1 deaths per thousand live births in 2015 to 9.6 in 2019, and in the Center-West region where the mortality rate reduced from 8.72 deaths to 8. 25 for every thousand live births in the same period. On the other hand, the North, Southeast, and South regions maintained stationary mortality rates between the years 2015 to 2019 (Table 2).
Table 2. Distribution of neonatal mortality rate and trend per 1,000 live births between regions, Brazil, 2015 to 2019.
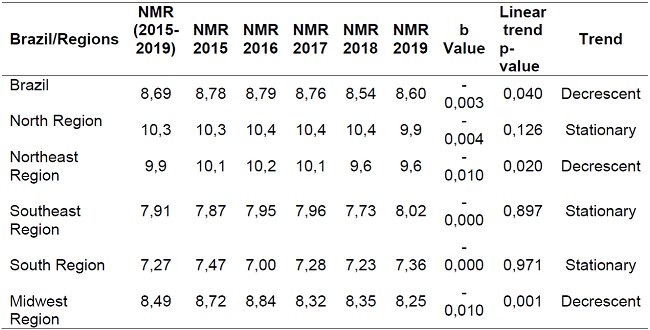
Source: Elaborated by the authors based on data extracted from the Information System on Mortality and the Information System on Live Births (ISM, ISLB/DH), 2022.
As for deaths due to preventable causes, there was a predominance of those that can be reduced by actions in the context of care for women during pregnancy (49.0%), followed by deaths that can be avoided by appropriate actions in care for newborns (30, 7%). All preventable causes decreased between 2015 and 2019, with emphasis on those reducible through diagnostic actions and adequate treatment, which decreased by 26.7% (Table 3).
Table 3. Distribution of neonatal deaths according to preventable causes in Brazil. Brazil, 2015-2019.
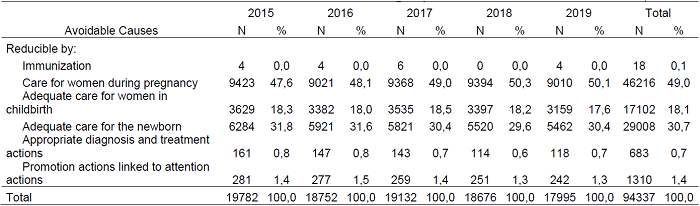
Source: Elaborated by the authors based on data extracted from the Information System on Mortality and the Information System on Live Births (ISM, ISLB/DH), 2022.
Deaths that could be prevented by actions related to newborn care, adequate diagnosis and treatment, and promotion actions linked to care actions showed a decreasing trend in the studied period (p<0.05) (Table 4).

DISCUSSION
Infant mortality (IM), which includes neonatal deaths, is considered one of the best indicators to measure the quality of life, health, and state of social well-being of a population, and presents an undesirable phenomenon in public health, since they are premature deaths and which in most countries happens due to preventable causes (21).
The present study reveals that there was a decrease in the neonatal mortality rate from preventable causes in Brazil during the period studied. Specifically, the Northeast and Midwest regions were responsible for a reduction of approximately 1.2% in preventable neonatal mortality in the country. On the other hand, the North, Southeast, and South regions maintained stable rates, a fact that needs to be thoroughly analyzed, since what was expected was an NMR with a decreasing trend in all regions. However, this scenery reveals that Brazil has been reaching values well below expectations, as recommended by the goal established by the Sustainable Development Goals (SDGs), which hopes to reduce, by the year 2030, the neonatal mortality rate to less than 12 deaths per thousand live births all over the world ((16),(17).
Several public policies have been implemented in recent years to reduce neonatal mortality in Brazil, such as the expansion of the Family Health Strategies (FHS), the Stork Network Program, the Bolsa Familia Program, which were fundamental to impact the health of mothers and children through access to income, education, and health services. The actions provided within the scope of these policies have contributed to women and society as a whole achieving a greater level of knowledge about their sexual and reproductive rights, in addition to a restructuring of maternal and child healthcare services. (22) (23) (24).
The downward trend in NMR in the country is supported by other studies that have been analyzing this historical series over the last few years, although high neonatal mortality rates are still evident when compared to other countries(15) (25) (26). In addition, the present study shows that neonatal deaths represent about 70% of all infant deaths in the period, and of these, almost 75% occurred due to preventable causes, that is, which could have been avoided by qualified maternal-infant care, especially those focused on prenatal care, care in the delivery room and care for newborns in neonatal units(27).
In this context, it is crucial to highlight the fundamental role of the infant and fetal mortality investigation committees in reducing this specific component of IM, which are preventable neonatal deaths, since this phenomenon is the main object of work of these committees, which act directly in the investigation of these deaths, to clarify the failures that culminated in the same, and to propose interventions from the perspective of preventability(28).
As for the analysis of the TMN in the period between the regions of the country, the study shows a higher rate in the north (10.3/1,000) and northeast (9.9/1,000), even surpassing the national TMN in the period (8.69 /1,000), a finding confirmed by other studies that evaluated the time series of neonatal deaths in the country(15)(25)(26). These findings confirm the existing discrepancies between the regions of Brazil, as a result of socioeconomic inequalities and difficulties in accessing health services, which are still very pronounced in the north and north regions, despite the incentives for mitigating this problem in recent years(27),(29).
Despite the other regions showing lower rates, including concerning the national TMN, the analysis showed that the south and southeast regions have a stationary trend when they should have shown decreasing trends since the implementation of public policies for the reduction of these rates is being fully operated in these regions(25),(27).
Regarding neonatal deaths according to preventable causes, although all causes have shown a reduction in the analyzed period, causes preventable by adequate care during pregnancy prevail (49.0%) over the other elements and showed a stationary trend. These findings are corroborated by other studies on the subject, though, in a study analyzing the historical series until 2017, taking into account a period of 10 years, an increasing trend was found according to the preventable cause in question(15) (25) (26).
The auspicious start and provision of adequate prenatal care are the main factors for reducing maternal and perinatal morbidity and mortality rates since during pregnancy it is possible to identify risk factors that can lead to unfavorable obstetric outcomes, thus carry out adequate prevention and or treatment to mitigate such outcomes(13) (27) (30).
A nationwide study(31) that evaluated the quality of prenatal care in the Family Health Strategies (FHS) showed low adequacy of infrastructure, care, and management for the operation of prenatal care in the country, with the percentages of adequacy below 50% in all regions, with the north region presenting the lowest percentage of adequacy, with only. In addition, another study(32) carried out in 2014 identified that the inadequacy of primary care for providing prenatal care was related to 40% of preventable infant and neonatal deaths in Brazil.
Neonatal deaths preventable by adequate care for the newborn corresponded to 30.7% of the total, with a decreasing trend, and deaths preventable by appropriate care during childbirth represented 18.1% of deaths in the period, with a steady trend. Studies that analyzed the historical series of the subject in question, according to regions of the country, also found results similar to those shown in this study (15),(25).
A systematic review study with meta-analysis of observational studies to identify the main risk factors associated with neonatal deaths identified that factors related to childbirth, structure, and management of obstetric care, and newborn care are planned and executed in an incipient and may determine an increase in unwanted neonatal outcomes, such as morbidity and mortality among this population(27).
Although they still represent a high percentage of preventable neonatal deaths, actions related to delivery and birth care have been the target of institutional actions in recent years, especially from 2011 with the implementation of the Stork Network Program, which aimed fundamentally at agreeing on actions for structuring places for obstetric care, training professionals for care, to reduce maternal and neonatal mortality. These actions contributed to the reduction of mortality from these causes over time, as demonstrated in this study(1) (6) (24).
In addition, the decreasing NMR, the second death that can be avoided by adequate care for the newborn, can be considered a result of the expansion of beds in the Neonatal Intensive Care Unit (NICU) in the country, especially in regions with the greatest deficit, incorporation of new technologies for NICU care, training of professionals in the light of scientific evidence. These actions allowed for the improvement of neonatal care and the avoidability of neonatal death, especially in the first hours after birth(1) (2) (4) (27).
Neonatal mortality rates from other preventable causes were less frequent in the present study and all showed a downward trend, quite possibly thanks to programs related to child health, expansion of the FHS, and immunization, which are consolidated in the country and which contributed to the observed reduction on screen(23),(27).
One of the main limitations of this study was the fact that it was not possible to extract, due to the unavailability in the DH system, maternal and neonatal data such as maternal age, mother's education, gestational age, type of delivery, birth weight, which are considered major factors for the assessment of neonatal mortality rates(27).
NMR is multidetermined and the factors associated with it go beyond the health sector, permeating socioeconomic issues, population education, empowerment of the female population, and cultural issues. In this way, the actions to face it must also happen from intersectoral and coordinated actions(24),(27).
CONCLUSIONS
The results of this study revealed that there was a decrease in the neonatal mortality rate in Brazil, from 2015 to 2019, although the country still has rates considered high, given the numerous public policies and programs aimed at the qualification of maternal and child care, and which have been implanted and implemented in the country in the last decades.
Regarding the temporal trend analysis, the country presented a decreasing NMR in the analyzed period. On the other hand, in the geographic macro-regions, there was a decrease only in the Northeast and Midwest regions, with a stationary trend in the other regions, which allows us to discuss the need to qualify policies related to the health of mothers and children in the affected regions.
Concerning the analysis of deaths according to preventable causes, those that can reduce by adequate care during pregnancy, childbirth, and the newborn were the ones with the highest proportion, respectively. In the trend analysis, neonatal deaths that could reduce by appropriate care during pregnancy showed a steady state. Deaths that can avoid by proper care during childbirth and the newborn were decreasing. However, these findings reflect the low quality of prenatal care in Brazil already measured in large-scale studies, and reveal the urgent need to qualify managers and workers for adequate care for pregnant women in Primary Health Care.
Finally, the data analyzed in this research, originating from MIS and ISLB, both belonging to the Department of Health, can provide subsidies for the analysis of the health situation regarding neonatal mortality in Brazil and by regions, according to preventable causes, and thus, to qualify the analysis process of policies implemented in the field of maternal and child health, enabling the redefinition of actions when necessary.
REFERENCIAS
1. Pinheiro LC, Machado TB, Silva SAS, Melo AL, Sena RPS, Felix RO, et al. Produção científica acerca da mortalidade neonatal na primeira semana de vida. REAS. 2020;12(12): e4900. Doi: 10.12957/reuerj.2015.5794. [ Links ]
2. Paulista MC, Azevedo LS, Melo EC, Oliveira RR. Prevalência e causas da mortalidade neonatal no Brasil. R Pesq Cuid Fundam. 2022;14:e11615. Doi: 10.9789/2175-5361. [ Links ]
3. Mulu GB, Gebremichael B, Desta KW, Kebede MA, Aynalem YA, Getahun MB. Determinants of Low Birth Weight Among Newborns Delivered in Public Hospitals in Addis Ababa, Ethiopia: Case-Control Study. Pediatr Heal Med Ther. 2020; 11:119-26. Doi: 10.2147/phmt.s246008. [ Links ]
4. Oliveira EAR, Lima CSO, Cirino IP, Vera PVS, Lima LHO, Conde WL. Mortalidade neonatal: causas e fatores associados. Saúde em Redes. 2020;(6)3: 113-117. Doi: 10.1016/j.bpobgyn.2016.06.002. [ Links ]
5. Silva EMP, Sanchez METL, Ferreira ALC, Lucena KNC, Oliveira KRV, Santos AAP. Impacto da implantação da Rede Cegonha nos óbitos neonatais. Rev Enferm UFPE On Line 2019; 13(5):1317-1326. Doi: 10.5205/1981-8963-v13i5. [ Links ]
6. França EB, Lansky S, Rego MAS, Malta DC, França JS, Teixeira R, et al. Principais causas da mortalidade na infância no Brasil, em 1990 e 2015: estimativas do estudo de Carga Global de Doença. Rev. bras. epidemiol. 2017;20(Supl.1):46-60. Doi: 10.1590/1980-5497201700050005. [ Links ]
7. Kropiwiec MV, Franco SC, Amaral AR. Fatores associados à Mortalidade Infantil em município com índice de desenvolvimento humano elevado. Rev Paul Pediatr. 2017; 35 (4):391-8. Doi: 10.1590/1984-0462. [ Links ]
8. Liu L, Oza S, Hogan D, Chu Y, Perin J, Zhu J, et al. Global, regional, and national causes of under-5 mortality in 2000-15: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet. 2016; 388:3027-35. Doi: 10.1016/s0140-6736(16)31593-8 [ Links ]
9. Fundo de Emergência Internacional das Nações Unidas para a Infância (UNICEF). Levels and Trends in the level of child mortality [Internet]. UNICEF; 2019 [acessado em 15 fev. 2022]. Disponível em: https://www.unicef.org/reports/levels-and-trends-child-mortality-report-2019. [ Links ]
10. World Health Organization (WHO). Neonatal Mortality Rate. 2019. [acessado 2022 Fev 15]. Disponível em: https://childmortality.org/?r=site/graph&ID=BRA_Brazil,2019. [ Links ]
11. Roma JC. Os objetivos de desenvolvimento do milênio e sua transição para os objetivos de desenvolvimento sustentável. Cienc. Cult. 2019; 71(1): 33-39. Doi: 10.21800/2317-66602019000100011. [ Links ]
12. Paim J, Travassos C, Almeida C, Bahia L, Macinko J. The Brazilian health system: history, advances, and challenges. Lancet 2011; 377(9779):1778-97. Doi: 10.1016/s0140-6736(11)60054-8. [ Links ]
13. Migoto MT, Oliveira RP, Silva AMR, Freire MHS. Mortalidade neonatal precoce e fatores de risco: estudo caso-controle no Paraná. Rev Bras Enferm. 2018;71(5):2675-83. Doi: 10.1590/0034-7167-2016-0586. [ Links ]
14. Medeiros VAB, Bezerra INS, Mota LM, Monteiro FS. Perfil da mortalidade neonatal em Alagoas no período de 2008 a 2017. Rev Cienc Plural. 2019; 5(2):16-31. Doi: 10.21680/2446-7286.2019v5n2ID16212. [ Links ]
15. Bernardino FBS, Gonc¸alves TM, Pereira TID, Xavier JS, Freitas BHBM, Gaíva MAM. Tendência da mortalidade neonatal no Brasil de 2007 a 2017. Ciência & Saúde Coletiva. 2022; 27(2):567-578. Doi: 10.1590/1413-81232022272.41192020. [ Links ]
16. Brasil. Ministério da Saúde. O Brasil e os Objetivos do Desenvolvimento do Milênio [Internet]. 2018. [acesso 15 fevereiro 2022]; 1-4. Disponível em: http://www.odmbrasil.gov.br/o-brasil-eosodm. [ Links ]
17. Hug L, Alexander M, You D, Alkema L. National, regional, and global levels and trends in neonatal mortality between 1990 and 2017, with scenario-based projections to 2030: a systematic analysis. Lancet Glob Health. 2019;7(6):e710-20. Doi: 10.1016/s2214-109x(19)30163-9. [ Links ]
18. Antunes JLF, Cardoso MRA. Uso da análise de séries temporais em estudos epidemiológicos. Epidemiol Serv Saude. 2015;24(3):565-76. Doi: 10.5123/S1679-49742015000300024. [ Links ]
19. Malta DC, Sardinha LMV, Moura L, Lansky S, Leal MC, Szwarcwald CL et al. Atualização da lista de causas de mortes evitáveis por intervenções do Sistema Único de Saúde do Brasil. Epidemiol Serv Saúde. 2010; 19(2):173-6. Doi: 10.5123/S1679-49742010000200010. [ Links ]
20. Adamski K, Silva TG, Pereira PPS, Farias ES, Cantarelli KJ, Mendes VA. Mortalidade infantil por causas evitáveis em macrorregião de saúde: série temporal 2007 a 2020. REAS. 2022;(15)8:e10545. Doi: 10.25248/reas.e10545.2022. [ Links ]
21. Moura BLA, Alencar GP, Silva ZP, Almeida MF. Fatores associados à internação e à mortalidade neonatal em uma coorte de recém-nascidos do Sistema Único de Saúde, no município de São Paulo. Rev Bras Epidemiol. 2017; 23: e200088. Doi: 10.1590/1980-549720200088. [ Links ]
22. Dourado I, Medina MG, Aquino R. The effect of the Family Health Strategy on usual source of care in Brazil: Data from the 2013 National Health Survey (PNS 2013). Int J Equity Health. 2016 ; 15 (1): 151. Doi: 10.1186/s12939-016-0440-7. [ Links ]
23. Leal MDC, Szwarcwald CL, Almeida PVB, Aquino EML, Barreto ML, Barros F et al. Reproductive, maternal, neonatal and child health in the 30 years since the creation of the Unified Health System (SUS). Ciênc Saúde Coletiva. 2018; 23(6): 1915-28. Doi: 10.1590/1413-81232018236.03942018. [ Links ]
24. Silva ESA, Paes NA. Bolsa família programme and the reduction of child mortality in the municipalities of the Brazilian semiarid region. Ciênc Saúde Coletiva. 2019; 24 (2):623-30. Doi: 10.1590/1413-81232018242.04782017. [ Links ]
25. Prezotto KH, Oliveira RR, Pelloso SM, Fernandes CAM. Trend of preventable neonatal mortality in the States of Brazil. Rev. Bras. Saúde Mater. Infant. 2021; 21 (1): 301-309. Doi: 10.1590/1806-93042021000100015. [ Links ]
26. Kale PL, Fonseca SC, Oliveira PWM, Brito AS. Fetal and infant mortality trends according to the availability of causes of death and maternal education. Rev Bras Epidemiol 2021; 21(suppl 1): e180008. Doi: 10.1590/1980-549720210008. [ Links ]
27. Veloso FC, Kassar LM, Oliveira MJ, Lima TH, Bueno NB, Gurgel RQ, et al. Analysis of neonatal mortality risk factors in Brazil: a systematic review and meta-analysis of observational studies. J Pediatr (Rio J). 2019; 95:519-30. Doi: 10.1016/j.jped.2018.12.014. [ Links ]
28. Ruoff AB, Andrade SR, Schmitt MD. Atividades desenvolvidas pelos comitês de prevenção do óbito infantil e fetal: revisão integrativa. Rev Gaúcha Enferm. 2017; 38(1): e67342. Doi: 10.1590/1983-1447.2017.01.67342. [ Links ]
29. Albuquerque MV, Viana ALA, Lima LD, Ferreira MP, Fusaro ER, Iozzi FL. Desigualdades regionais na saúde: mudanças observadas no Brasil de 2000 a 2016. Cien Saude Colet 2017 ; 22(4):1055-1064. Doi: 10.1590/1413-81232017224.26862016. [ Links ]
30. Medeiros VAB, Bezerra INS, Mota LM, Monteiro FS. Perfil da mortalidade neonatal em Alagoas no período de 2008 a 2017. Rev Cienc Plural. 2019; 5(2):16-31. Doi: 10.21680/2446-7286.2019v5n2id16212. [ Links ]
31. Guimaraes WSG, Parente RCP, Guimaraes TLF, Garnelo L. Acesso e qualidade da atenção pré-natal na Estratégia Saúde da Família: infraestrutura, cuidado e gestão. Cad Saúde Pública. 2018; 34 (5): e00110417. Doi: 10.1590/0102-311x00110417. [ Links ]
32. Tomasi E, Fernandes PAA, Fischer T, Siqueira FCV, Silveira DS, Thumé E et al. Qualidade da atenção pré-natal na rede básica de saúde do Brasil: indicadores e desigualdades sociais. Cad Saúde Pública. 2017; 33 (3): e00195815. Doi: 10.1590/0102-311x00195815. [ Links ]
Received: January 25, 2023; Accepted: April 18, 2023
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
