










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
versión On-line ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.11 no.1 ene./feb. 2006
Gastroesophageal reflux diagnosed by occlusal splint tintion
José Luis Cebrián Carretero 1,José María López-Arcas Calleja 2
(1) Médico Adjunto. Servicio de Cirugía Maxilofacial
(2) Médico Residente. Servicio de Cirugía Maxilofacial. Hospital Universitario La Paz
ABSTRACT
The gastroesophageal reflux (GER) disease is a very frequent digestive disorder, mainly characterised by the reflux of the gastric acidic content to the esophage in abnormal quantities. There are different situations that favour this situation but almost in all of them rely an incompetence of the esophagic sphincter. The clinical consequences are many, including oral manifestations. Among all of them the most frequent is the esophagitis followed by symptoms at the pharynx or larynx and finally, the oral cavity. At this level fundamentally we will find enamel and oral mucosa erosions. We report the case of a patient who was indirectly diagnosed of her esophague disease by the observation of the alterations in the occlusal splint induced by the gastric reflux. We review the literature concerning the above topic and its possible association with the miofascial syndrome.
Key words: Gastroesophageal Reflux, Miofascial Síndrome.
RESUMEN
El reflujo gastro-esofágico (RGE) es un trastorno digestivo muy frecuente que se caracteriza por el paso de cantidades patológicas de ácido del estómago hacia el esófago. Esto es debido a una incompetencia de los mecanismos que regulan la retención del contenido gástrico en el estómago por causas primarias o secundarias. Las consecuencias clínicas de este reflujo afectan al tracto aerodigestivo superior, incluyendo la boca. Lo más frecuente es la esofagitis, seguido por la afectación de faringe y laringe y finalmente por alteraciones patológicas en la boca. A éste nivel lo más frecuente es la erosión del esmalte y las lesiones erosivas de la mucosa oral. Presentamos el caso de un paciente en el que el RGE fue diagnosticado de forma indirecta por la impregnación y coloración de una férula oclusal utilizada para el tratamiento de un síndrome miofascial. Partiendo de este caso se discuten las consecuencias del RGE en la cavidad oral y su asociación con el dolor muscular masticatorio.
Palabras clave: Reflujo Gastro-Esofágico, Síndrome Miofascial.
Introduction
The gastroesophageal reflux (GER) is one of the most frequent digestive disorders. Approximately 25% of the US population will suffer at least one symptom of GER during their lives.
It occurs when the amount of gastric juice that refluxes into the esophagus exceeds the normal limit, causing symptoms with or without associated esophageal mucosal injury (esophagitis).
The ethiology can be cryptic or associated to a Hiatal Hernia, sclerodermya, smoking, alcohol, poor dietary habits, food allergies, anticolinergic or smooth muscle relaxing medications, or even surgical destruction, etc.)(1).
Moreover, an increment of the gastric volume or pressure (obesity, pregnancy) favours the gastric reflux.
Approximately 50% of patients with reflux develop esophagitis, which is classified into 4 grades based on severity. Grade I is erythema, grade II is linear nonconfluent erosions, grade III is circular confluent erosions. When it scars by intestinal metaplasia we achieve the grade IV or Barrett esophagus, which represents a great risk of developing a esophageal cancer. It is considered the main complication of the GERD and begins when the protective mechanisms are overcome by the amount of gastric acid reflux.
Besides the typical symptoms (heartburn, regurgitation, dysphagia), abnormal reflux can cause atypical symptoms such as coughing, chest pain, and wheezing and also damage to the lungs (pneumonia, asthma, idiopathic pulmonary fibrosis), vocal cords (laryngitis, cancer), and teeth (enamel decay).
Clinical case
We present the case of a 40-year old caucasian female assisted at first by her Primary Care Doctor for headache, daily somnolence and frequent nightly awakenings. Besides the patient presented pain localised at the occipital and temporal regions. She was sent to the pneumologyst with the suspicion of SAOS, which was ruled out after going through a polysomnography. The referred pain continued getting worse day by day, the reason why se was suggested to come to our Unit of Oral and Facial Pain. The clinical exploration showed a dissoclusion type 2 of Angle, slight occlusal erosion, as well as signs and symptons of malfunction of the masticatory system, including trigger points in both maseteric and ECM. The patient also referred backache, and diffuse gastric symptons.
A treatment with NEAIS and muscle relaxers was implemented, in addition to a plain occlusal splint, Michigan type.
Three months later, the pain had relieved though she still had some difficulties to sleep.
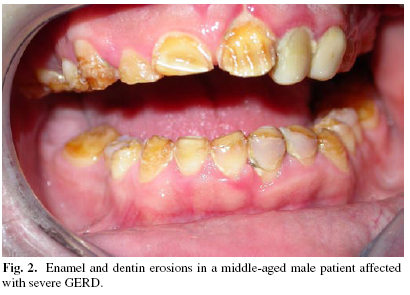
By the examination of the discharging splint we noticed a dark-green colouring of it which greatly reminded us the appearance of the gastric juices (Fig 1)//(Fig2)
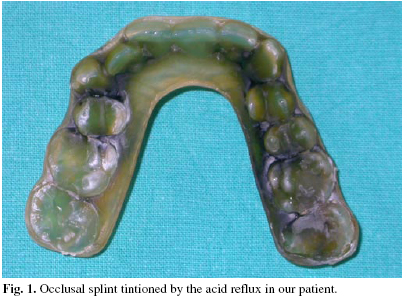
Taking to account the clinical symptoms of the patient which included gastric manifestations and the remarkable colouring of the splint we suspected a GER. The gastroenterologyst, confirmed the diagnose after performing the pertinent tests (pHmetry and endoscopy) .
The patient was treated with dietary measures and proton pump inhibitors.
6 months later in the next revision, we were glad to see that most of her symptoms had disappeared. The patient continues in our Facial Pain Management program with good results and without gastric symptoms. (Fig.1 and 2).
Discussion
The presence of acid juices in the oral cavity may produce different effects. We often notice symptoms at the smooth tissues which are usually expressed in terms of hyperstesia and oral burn without any pathological lesion at this level (2).
The teeth erosion (3,4,5,6), however, is considered the main manifestation GRE at the oral cavity. This relationship between GRE and dental erosion was first described by Bargen and Austin in 1.937(3). It is so important because in some cases it can be the only clinical sign of GERD. The dental pathology usually begins with subtle changes at the enamel which in some occasions can progress till the complete loss of the dental tissue. As there are many possible causes of enamel erosion the diagnose can be very difficult.
Although the main mechanism of teeth lesion in the patients with GERD is the progressive degeneration of the enamel and the dentine under the acid exposure there are many other factors involved in one sense or another in the clinical evolution. Among all of them the most important is the salivary system as a buffer of the refluxed gastric juices.
Nevertheless in most patients with GERD it is impossible to find any stigma at the oral cavity although they can manifest any other symptomatology. In this case, the clinical signs were subtle, but evident if we consider the natural association between the GERD and the masticatory muscular pain. It is based in the fact that this kind of the patients, classically described as type A personalities, are predisposed to suffer both diseases. Se trata de los clásicamente descritos como personalidades de tipo A(7).
The colouring or tintions of the prostheses and splints may be considered a stigma for itself of the GERD and should warn about the possible diagnose of GERD.
The diagnose of GER may be made by endoscopy or esophague endoscopy. The first one quantifies the amount of acid that reflux while the second one evaluates the consequences of the reflux at the esophague (8).
The treatment aims, reducing the reflux, neutralizing the refluxed material, accelerating the esophague dumping and protecting the esophage mucosa (8).
The less complicated cases usually ameliorate with dietary and behavioural measures (weight loss, stop smoking, elevate the bedhead, avoid the copious meals, etc.)
In the cases grade mild to severe it is necessary to suplement the measures above enumerated. Proton Pump inhibitors like the Omeprazol at doses of 20 to 40 mg per day have been proved as a extremely effective treatment option for this pathology. The esophaguitis due to reflux usually requires a 3-6 months treatment or even more if it rapidly recidives.
For those cases where the medical treatment is not enough to control the symptoms a surgical procedure may be indicated.
In our case the way to diagnose showed us a way to treat the dental erosion as a side effect of the gastric reflux in the oral cavity. In this sense the use of dental splints during the sleep may protect the teeth.
![]() Correspondence
Correspondence
Dr. José Luis Cebrián Carretero
Servicio de Cirugía Maxilofacial.
Hospital Universitario La Paz.
Paseo de la Castellana 246. 28046 Madrid.
Telef: 917277336.
E-mail: drlopezarcas@tiscali.es.
Received: 27-02-2005
Accepted: 10-07-2005
References
1. Harrison. Harrison eds. Principios de Medicina Interna ed. 14. Madrid:McGraw-Hill-Interamericana de España, S.A.U; 2002. p. 1807-11. [ Links ]
2. Orr WC. Sleep and gastroesophageal reflux disease: a wake-up call.Rev Gastroenterol Disord. 2004;4:25-32. [ Links ]
3. Lazarchik DA. Effects of gastroesophageal reflux on the oral cavity. Am J Med 1997;103:107-13. [ Links ]
4. Valena V. Dental erosion patterns from intrinsic acid regurgitation and vomiting. Aus Dent J 2002;47:106-15. [ Links ]
5. Taylor G. Dental erosion associated with asymptomatic gastroesophage reflux 1992;59:182-5. [ Links ]
6. Linnet V. Dental erosion in children: a literature review. Pediatr Dent 2001;23:37-43. [ Links ]
7. Keltikangas-Jarvinen L. The prevalence and construct validity of type A behaviour in patients with duodenal ulcers. Br J Med Psychol 1987;60:163-7. [ Links ]
8. Modlin I. GERD 2004: Issues from the past and a consensus for the future. Best Pract Res Clin Gastroenterol. 2004;18:55-66. [ Links ]

