










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
versión On-line ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.11 no.1 ene./feb. 2006
ORAL SURGERY
Colon adenocarcinoma with metastasis to the gingiva
Carlos Álvarez Álvarez 1, Begoña Iglesias Rodríguez 1, Susana Pazo Irazu 2, Carlos Delgado Sánchez-Gracián 3
(1) Médico adjunto. Servicio de Anatomía Patológica
(2) Médico adjunto. Servicio de Otorrinolaringología
(3) Médico adjunto. Servicio de Radiología. Hospital POVISA. Vigo (Pontevedra)
ABSTRACT
Metastatic tumors involve the oral cavity, and the most common primary sites are the breast and lung. Most cases affect the mandible and maxilla in that order, although some of them can be located in the soft perioral tissues. We report the case of a 62-year-old male who had been diagnosed with sigmoid adenocarcinoma with nodal and liver metastasis, who presented 6 months later with a gingival polypoid tumor, at first considered as a primary neoplasm of gingiva, that was diagnosed in a biopsy as metastatic intestinal adenocarcinoma. The histological evaluation is essential to separate adenocarcinoma from the commoner in this site squamous cell carcinoma, and the immunohistochemical techniques are useful to distinguish metastatic tumor versus primary adenocarcinoma from the minor salivary glands of the area. The intraoral spread of a disseminated neoplasm is generally a sign of bad prognosis, although a longer survival can be expected if a radical surgical treatment of a solitary metastasis is carried out.
Key words: Gingiva, adenocarcinoma, metastasis, colon.
RESUMEN
La cavidad oral es lugar de asiento de tumores metastásicos, sobre todo con origen en mama y pulmón. La mayoría de los casos afectan por este orden a los huesos mandibular y maxilar, aunque en ocasiones se desarrollan sobre las partes blandas intraorales. Presentamos el caso de un paciente de 62 años diagnosticado de adenocarcinoma de colon sigmoide con metástasis ganglionares y hepáticas, que 6 meses después presenta una lesión vegetante en la encía, interpretada inicialmente como neoplasia primaria de encía, que tras ser biopsiada fue diagnosticada como adenocarcinoma intestinal metastásico. El estudio histológico es obligatorio para diferenciar un adenocarcinoma de los carcinomas de células escamosas, habituales en la zona, y las técnicas inmunohistoquímicas permiten diferenciar entre un tumor metastásico, sea intestinal o de otro origen, y un adenocarcinoma primario originado en glándulas salivares menores de la zona. La presencia de un tumor diseminado con extensión intraoral acarrea un pronóstico ominoso, aunque si se trata de una metástasis única es posible un tratamiento quirúrgico radical con una supervivencia mayor.
Palabras clave: Encía, adenocarcinoma, metástasis, colon.
Introduction
Metastatic tumors to the oral cavity are uncommon, accounting for 1% of all neoplasms in the area, and their primary origin can be anywhere (1). Most patients were previously diagnosed with primary neoplasm and treated, although in one third of them metastasis is the first clinical sign (1,2). The most common primary tumors were lung in men and breast in women (1,2). Colonic carcinoma is the most frequent malignant gastrointestinal neoplasm, and one of the commonest tumors in the general population. We report a patient with sigmoid colon carcinoma who developed metastasis to the oral soft tissues and mandibular bone, emphasizing the differential diagnosis and the value of immunohistochemical techniques in the final diagnosis.
Case Report
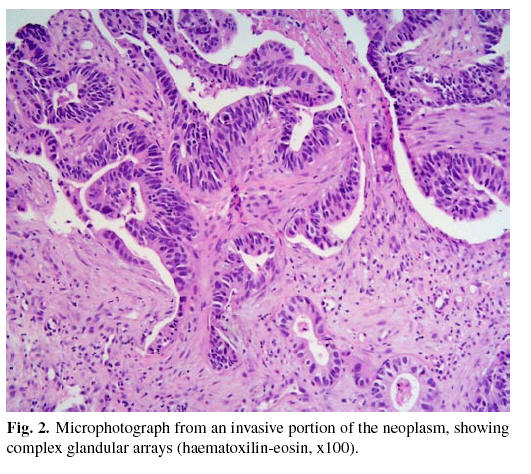
A 62-year-old male was diagnosed in September 2003 under radiographic examination with a sigmoid stenosing tumor with metastasis to regional lymph nodes and liver (stage IV). Endoscopical biopsies from the neoplasm were taken, and the diagnosis was intestinal adenocarcinoma. Tumor was considered irresectable, and was treated with a palliative colostomy and chemotherapy with FOLFOX regimen (oxaliplatin-5-fluorouracil-leucovorin). The patient was reevaluated after 6 cycles, showing no tumoral progression, but after 12 cycles metastasis to the lymph nodes and adrenals were noted. In March 2004 the patient presented with pain and swellings in the mandibular region of 3 weeks duration, and an exophytic tumor in the right anterior mandibular gingiva was observed. CT scan of the head and neck showed a solid mass involving the right mandible with bony erosion, 4 cms in diameter, suggesting a primary neoplasm of gingiva (figure 1), without lymphadenopathy. A biopsy was performed, showing a neoplasm not connected to the mucosal surface, made up by irregular, atypical glands, lined by columnar cells with numerous mitotic figures (figure 2). The tumor cells showed positive immunostaining for cytokeratin (CK) 20 and CEA (carcinoembryonic antigen), and negativity for CK7, and the final diagnosis was intestinal metastatic adenocarcinoma. The patient was planned for 4 cycles of chemotherapy with the FOLFORI regimen (CPT11-5 fluorouracil-leucovorin), and palliative radiotherapy to metastatic sites, but the condition started deteriorating and he succumbed to disease within 9 months of diagnosis of gingival metastasis. Necropsy was not conceded.

Discussion
Less than 1% of all oral malignant tumors are metastatic. In a review, Van der Waal et al (1) found 24 in 1537 patients with oral cavity neoplasms, 1 of them from the colon. The most common primary sources were in decreasing order, breast, lung, kidney and prostate (1-4), although lung is the most common primary site if only the metastasis in soft tissues of the mouth are considered (2).
There are no significant differences regarding sex in the reported cases (1-3). Oral metastasis involving the gingiva may present clinically as a firm polypoid tumor, and the pathological study of the lesion is necessary for the diagnosis. The predominant histological type was adenocarcinoma in 65% of cases (1), and immunohistochemical techniques are compulsory to confirm either the primary or metastatic origin of the neoplasm. Colorectal adenocarcinomas usually express CK20, but not CK7 (5), and in addition to positivity for CEA other origins can be ruled out with confidence. From a pathological point of view, the differential diagnosis includes the adenoid squamous cell carcinoma, with a pseudoglandular pattern, and above all the polymorphous low-grade adenocarcinoma, that affects the minor salivary glands of the mouth, which is located preferentially to the palate (6). This is a low grade malignancy, with features resembling mixed tumor and adenoid cystic carcinoma and occasional recurrences, although with a favorable prognosis, with negative immunostaining for CEA (7).
Most intraoral metastatic tumors present in patients who had also developed metastasis at other sites, but in up to 30% of patients they are the first clinical sign of primitive tumor spreading or of a recurrence after a period free of disease.
Most of the oral metastasis involve the bone, the mandible being the most common, while only one third are in the soft tissue of the oral cavity (1-4), mostly located in the gingiva and tongue (2). In this case report, the tumor involved both the gingiva and the mandible, and the computed tomography, showing a well defined area in the mandible and an expansive pattern in the gingiva, help evaluate the extent of the process and highly suggest a progression from bone to the oral cavity.
The mechanism of metastatic dissemination is unclear, but a hematogenous spread from a distant focus is suggested. In the gastrointestinal tract, colonic carcinomas usually display metastasis to regional lymph nodes, liver, peritoneum, lung or ovaries, rarely at the supraclavicular organs (8).
The treatment of the metastatic tumors depends on the degree of dissemination of the neoplasm and the location. Metastasis in the soft oral tissues should be approached surgically, whatever the spread of the tumor may be. Surgical resection is recommended when oral metastasis is the only one present and the bone is involved, but if the tumor is widely disseminated a palliative radiotherapic treatment is recommended (1). Mean survival time for advanced cases after the diagnosis is 6 months (1).
In summary, although rare, metastatic tumors should be included in the differential diagnosis of an intraoral malignant neoplasm, above all if there is a primary known tumor and the histologic features are similar, because in some patients this could be the first indication of the presence of a primary tumor.
![]() Correspondence
Correspondence
Dr. Carlos Álvarez Álvarez
Servicio de Anatomía Patológica
Hospital POVISA
C/Salamanca 5. 36211 Vigo (Pontevedra). España
Tfno: 986413144 ext 1530 - Fax: 986421439
Email: capialvarez@yahoo.com
Received: 12-03-2005
Accepted: 25-05-2005
References
1. van der Waal RIF, Buter J, van der Waal I. Oral metastases: report of 24 cases. Brit J Oral Maxilofacial Surg 2003;41:3-6. [ Links ]
2. Hirshberg A, Buchner A. Metastatic tumours to the oral region. An overview. Eur J Cancer B Oral Oncol 1995;31B: 355-60. [ Links ]
3. Valdivieso M, Ostroa J, Lobos N. Oral and maxillofacial metastases of neoplasms from other sites of the body. Med Oral 1999;4:583-7. [ Links ]
4. Bhutani MS, Pacheco J. Metastatic colon carcinoma to oral soft tissues. Spec Care Dentist 1992;12:172-3. [ Links ]
5. Kende AI, Carr NJ, Sobin LH. Expression of cytokeratins 7 and 20 in carcinomas of the gastrointestinal tract. Histopathology 2003;42:137-40. [ Links ]
6. Kumar M, Stivaros N, Barrett AW, Thomas GJ, Bounds G, Newman L. Polymorphous low-grade adenocarcinoma-a rare and aggressive entity in adolescence. Brit J Oral Maxillofacial Surg 2004;42:195-9. [ Links ]
7. Hannen EJM, Bulten J, Festen J, Wienk SM, de Wilde PCM. Polymorphous low grade adenocarcinoma with distant metastases and deletions on chromosome 6q23-qter and 11q23-qter: a case report. J Clin Pathol 2000;53:942-5. [ Links ]
8. Cama E, Agostino S, Ricci R, Scarano E. A rare case of metastases to the maxillary sinus from sigmoid colon adenocarcinoma. ORL 2002;64:364-7. [ Links ]

