










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
versión On-line ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.11 no.2 mar./abr. 2006
Interceptive orthodontics: The need for early diagnosis and treatment of posterior crossbites
Ortodoncia interceptiva: Necesidad de diagnóstico y tratamiento temprano en las mordidas cruzadas transversales
Amparo Castañer Peiro
Lecturer in Orthodontics. Health Care, Public Health and
Veterinary Health Department.
Cardenal Herrera-CEU University. Alfara del
Patriarca. Valencia
ABSTRACT
Crossbites are the result of a malocclusion on the transverse
plane of the maxilla and are defined as alterations of the correct alignment of
the palatal cusps of the upper molars and premolars with the pits of the lower
molars and premolars.
Transverse alterations are frequently seen in general dental
practices and it is necessary to establish a good differential diagnosis in
order to adopt the treatment that will achieve the greatest efficiency and the
most stable Results possible. Skeletal constriction, dentoalveolar constriction
and dental constriction must therefore be differentiated, as each requires
different treatment with different orthodontic appliances.
This article aims to provide a simple guide to the correct
diagnosis of transverse anomalies and to choosing the most suitable orthodontic
appliance for each case.
Key words: Transverse anomalies, unilateral crossbite, bilateral crossbite, Quad-Helix, Haas expander.
RESUMEN
Las mordidas cruzadas corresponden a una
maloclusión en el plano transversal del maxilar definiéndose como la alteración
en la correcta articulación de las cúspides palatinas de molares y premolares
superiores con las fosas de molares y premolares inferiores.
Dada la frecuencia de alteraciones transversales que se presentan en la consulta
de odontología general, vemos la necesidad de realizar un buen diagnostico
diferencial de las mismas para poder adecuar nuestros tratamientos de la forma más
eficaz y con los Resultados más estables posibles. Para ello se ha de
diferenciar entre compresión esquelética, compresión dentoalveolar y compresión
dental ya que estos tres supuestos requerirán tratamientos diferentes con
aparatología ortodóncica diferente.
El propósito de este artículo es disponer de una guía sencilla en la que
apoyarnos para realizar un diagnostico correcto de las alteraciones
transversales y una guía para elegir la aparatología ortodóncica más
adecuada en cada caso.
Palabras clave: Anomalías transversales, mordida cruzada unilateral, mordida cruzada bilateral, Quad-Helix, Disyuntor.
Introduction
Crossbites are defined as the occlusion between the buccal cusps of the upper molars and premolars and the pits of the lower molars and premolars.
The frequency of crossbites seen in dental clinics varies between 1% and 23%, according to different studies. The most frequent is single-tooth crossbite, at around 6-7%, followed by unilateral crossbites, around 4-5%, and lastly, bilateral crossbites, which make up 1.5% - 3.5% (1). The frequency of crossbites is not influenced by either age or sex.
In 1899 Angle proposed the first classification of malocclusions, but although this is the classification that has gained the greatest acceptance world-wide, it only takes the anterior-posterior plane into account (2). As a result, in 1921 Hellman stated that it is as important for the mesio-buccal cusp to be in Angles class I as it is for the mesio-palatal cusp to be positioned in the central pit of the lower molar (3). However, it was Paul W. Simon, in 1926, who provided a classification on the three spatial planes: anterior-posterior, transverse and vertical (3). The classification proposed by Schwarz contained sixteen groups and their respective sub-groups. Thenceforward a more global vision of malocclusions could be obtained. Many classifications have subsequently been proposed, but it was not until 2002 that Lorente (3) presented the first classification of transverse alterations that takes dentoalveolar compensations into account and relates them to mandible size.
After classifying the posterior crossbite, the most suitable expansion treatment must be chosen. Maxillary expansion to treat bone/tooth discrepancy has been a perpetual concern since the early days of orthodontics. In 1881 W.H. Coffin designed an appliance with a central spring made of piano wire that expanded the maxilla, but it was E. H. Angell, in 1860, who designed the first appliance that opened the mid-palatal suture. However, early 20th century studies asserted that expansions only caused changes at a dentoalveolar level rather than at a skeletal level.
In 1987, Haas studied both the dental and skeletal effects of rapid maxillary expansion and observed opening of the mid-palatal suture, downward and forward displacement of the maxilla (8, 9) and mandibular postero-rotation.
Subsequently, studies have been conducted to forestall the undesirable effects of rapid expansion and mandibular postero-rotation is avoided by using a high chin support.
In 1975, Rickets described the Quad-Helix appliance (10) as an ideal treatment to achieve dental constriction through prolonged gentle pressure. In 1982, Greenbaun and Zachrisson studied the effects of expansion on the periodontal tissues for the first time (10). A study by Giron de Velasco in 2005 showed that the effect of Quad-Helix expansion was above all dental and produced extrusion of the upper molars, but that if expansion was carried out by rapid maxillary expansion after having corrected the dental compensations, the expansion was skeletal and intrusion of the upper molar took place.
Based on the classification of transverse malocclusions proposed by Lorente in 2002 (3, 4, 5, 6), these can be divided into unilateral crossbites and bilateral crossbites (Table 1) Based on this classification, the therapeutic alternatives for each are presented here below.

Diagnosis and treatment of posterior crossbites
Unilateral crossbite (UCB):
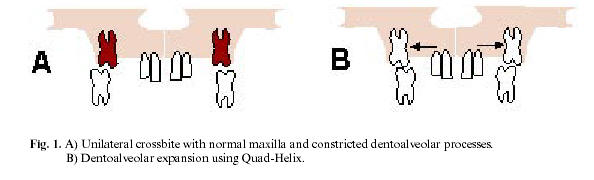
UCB with normal maxilla and constricted dentoalveolar process
There is no maxillary alteration, as the maxilla is not constricted, but constriction is found at dentoalveolar process level in the posterior sector. If the patient is observed occlusally it will be found that although his or her dentoalveolar processes are constricted, the crossbite is confined to one side, as a result of lateral displacement of the mandible on occlusion (5), and the dental midlines are off-centre.
Clinically, the dentoalveolar processes are symmetrically constricted, although intra-orally the patient presents unilateral crossbite.
The treatment is designed to expand the dentoalveolar processes symmetrically during the first stage of mixed dentition in order to reposition the mandible, as its functional deviation can be perpetuated unless corrected at an early stage. The appliances of choice are:
A) Removable appliance: Hawley appliance with midline expansion screw (7, 8). Activate a ¼ turn twice a week.
B) Fixed appliance: Quad-Helix fixed appliance attached to the upper molars by two bands (9). It is activated in the clinic with a three-prong plier. These two appliances only perform dentoalveolar expansions (10, 12).
As the expansion is performed symmetrically, the mandible is repositioned to centric occlusion (Figure 1).
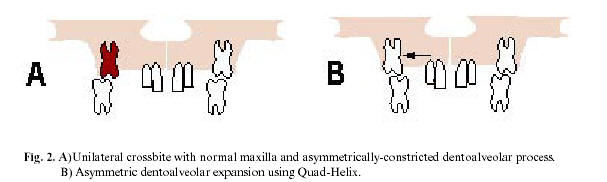
UCB with normal maxilla and asymmetrically-constricted dentoalveolar process
In this case there is no skeletal alteration of the maxilla but one of the posterior dentoalveolar processes is constricted, leading to unilateral crossbite on the constricted side (5). The diagnostic difference between this and the former case is that the unilateral crossbite persists when the mandible is corrected to a centric relation.
The treatment is designed to produce asymmetric expansion of the constricted dentoalveolar process. The appliances of choice are:
A) Removable appliance: Hawley appliance with a lingual shield on the side that is not to be expanded, providing the necessary anchorage to expand the opposite side.
B) Fixed appliance: Quad-Helix (13, 14); for asymmetric expansion the design needs to be modified by leaving the inner wire bordering the palatal faces of the upper premolars and canine on the side that is not to be expanded, to serve as anchorage, and removing the inner wire on the side to be expanded (figure 2).
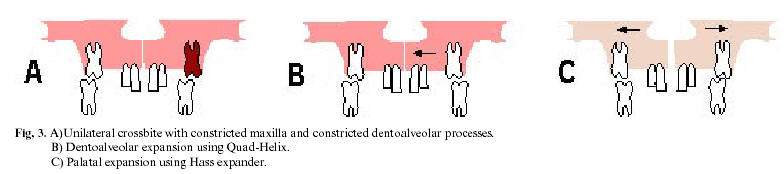
UCB with constricted maxilla and one buccally-displaced dentoalveolar process
In this case the patient presents skeletal alteration of the upper jaw expressed as maxillary constriction and the dentoalveolar processes are in an unequal relation to the basal bone: one presents a harmonious relationship, so a crossbite is found on this side, while the other is buccally displaced, thus presenting normal occlusion on the other side (5).
The treatment is designed to produce:
Unilateral palatal displacement of the buccally displaced dentoalveolar process, using a Quad-Helix to apply asymmetric constriction. This converts the unilateral crossbite into bilateral crossbite with maxillary constriction and harmonises the dentoalveolar processes with their basal bones (15, 16)
Subsequently, symmetrical expansion of the bony bases of the maxilla should be performed as early as possible, when the first upper molars erupt, as orthopaedic treatment is indicated. The appliance of choice is the Haas expander (17), a four-band fixed appliance with a central expansion screw that opens the mid-palatal suture when activated. Intraorally, the presence of an inter-incisor diastema will be observed (figure 3). In this case, a different appliance is preferred because the aetiology is different.
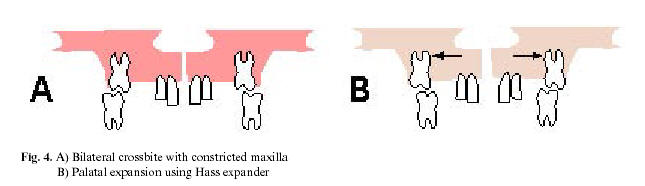
Bilateral crossbite (BCB)
BCB with constricted maxilla
The maxilla presents skeletal constriction and if the relationship between the alveolar processes and the basal bones is harmonious, bilateral posterior crossbite of skeletal origin (4) will be found intra-orally.
The orthodontic treatment is designed to achieve symmetrical maxillary skeletal expansion (18, 19). The preferred appliance is the Haas expander, to open the mid-palatal suture, carrying out early orthopaedic treatment to correct the maxillary bone constriction (20). Later, if the patient presents bone/tooth discrepancy, a 2nd stage of treatment will be conducted with a fixed orthodontic appliance (figure 4).
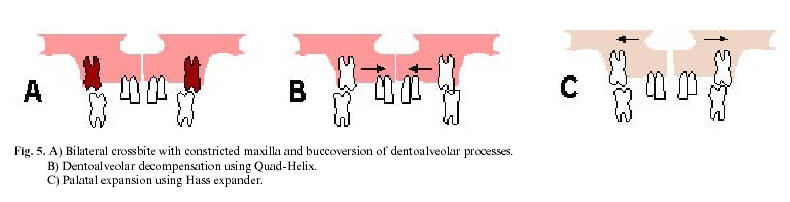
BCB with constricted maxilla and buccally-displaced dentoalveolar processes
Skeletal constriction of the maxilla is present but the maxillary dentoalveolar processes present buccoversion, attempting to compensate for the bone deficit. Intra-orally the patient will not present bilateral crossbite, but observation of the maxilla will show a development deficiency, presenting a triangular shape which, it is sensed, should be expanded (4).
Great care should be taken with the differential diagnosis in this case, as the molars are very close to the cortical bone and alveolar resorption could take place if the maxilla is expanded without having previously decompensated the dentoalveolar processes. The treatment criteria will be as follows:
Palatal displacement of the buccoversion dentoalveolar processes to coordinate these with their basal bones and create bilateral crossbite, using a Quad-Helix to apply constriction.
Early orthopaedic treatment, expanding the bony base of the maxilla with the Haas expander and opening the mid-palatal suture (21,22) when the first upper molars erupt. (figure 5).
BCB with constricted maxilla and mandibular excess
In this case the bilateral crossbite is caused more by the excessive development of the mandible, which is very difficult to treat, than by maxillary bone deficiency. Although a high percentage of these cases require surgical intervention, orthopaedic treatment of the maxilla is possible at an early age (4). The treatment criteria are as follows:
Dentoalveolar decompensation in the posterior maxillary area if necessary, using a Quad-Helix to apply constriction.
Orthopaedic treatment to expand the maxilla, using the Haas expander to open the mid-palatal suture at as early an age as possible, during the first stage of mixed dentition, in order to achieve as stable a result as possible (23, 24).
Dental alignment with a fixed appliance if necessary.
Reassessment of the case for guidance as to future surgery.
Conclusions
Correct diagnosis of crossbites is important, as if dentoalveolar compensations are present when expansion is performed the result will be scissors bite (25, 26). Equally, if there is buccoversion of the dentoalveolar processes and dentoalveolar expansion is performed, considerable gingival resorption can take place in the posterior sectors, in the premolars but more frequently in the canines, as these teeth are very close to the cortical bone. Good diagnosis is therefore very important in order to choose the most suitable appliances.
It should also be emphasised that it is very important to correct crossbites at an early age, during the first stage of mixed dentition, when these appliances (rapid maxillary expanders) can be used to open the mid-palatal suture and correct transverse skeletal problems (27). This suture can be opened when palatal expansion is performed in patients who are still growing, whereas in adult patients the only possible expansion is dentoalveolar rather than skeletal, which limits the correction of malocclusions.
Consequently, the following should be highlighted:
All transverse alterations should be treated as soon as possible, ideally during mixed dentition
If the transverse alteration is skeletal, the treatment should be even earlier, as soon as the first upper permanent molars erupt. Early treatment is essential for a stable result
If the transverse problem is dentoalveolar then treatment can be delayed until permanent dentition, but only while patients are still growing.
Dentoalveolar transverse problems are corrected with a Hawley appliance with an expansion screw or with a Quad-Helix.
For skeletal transverse problems the appliance of choice is a rapid maxillary expander
If the transverse alteration is accompanied by a vertical or anterior-posterior malocclusion, the transverse alteration must be treated first.
After correcting the transverse malocclusion at an early age, the Results must be stabilised with retainers until all the permanent teeth have replaced the deciduous teeth.
Prof. Amparo Castañer Peiro
Facultad de Ciencias Experimentales y de la Salud.
Edificio Odontología
C/ del Pozo s/n
Alfara del Patriarca 46115. Valencia
E-mail: amparo_peiro@uch.ceu.es
Received: 4-12-2005
Accepted: 31-01-2006
References
1. Bravo LA. ed. Manual de Ortodoncia. Madrid: Síntesis; 2003. p. 617-48. [ Links ]
2. Angle EH. Classification of malocclusion. Dent Cosmos 1899; 41:248-64. [ Links ]
3. Lorente P. Clasificación y tratamiento de las maloclusiones transversales. Rev Esp Ortod 2002;42:179-81. [ Links ]
4. Lorente P. Clasificación y tratamiento de las maloclusiones transversales. 1. Mordidas cruzadas bilaterales (MCB). Rev Esp Ortod 2002;42:182-95. [ Links ]
5. Lorente P. Clasificación y tratamiento de las maloclusiones transversales. 2. Mordidas cruzadas unilaterales (MCU). Rev Esp Ortod 2002;42:196-210. [ Links ]
6. Lorente P. Clasificación y tratamiento de las maloclusiones transversales. 3. Mordidas cruzadas completas (MCC). Rev Esp Ortod 2002;42:211-23. [ Links ]
7. Quiros OJ. ed. Ortodoncia nueva generación. Caracas: Amolca; 2003. p. 3-23. [ Links ]
8. Haas JA. Palatal expantion: Just the beginning of dentofacial orthopedics. Am J Ortod 1967;26:219-55. [ Links ]
9. Huertas D, Ghafari J. New posteroanterior cephalometric norms: A comparison with craneofacial measures of children treated with palatal expansion. Angle Orthod 2001;71:285-92. [ Links ]
10. Greenbaun KR, Zachrisson BU. The effect of palatal expansion therapy on the periodontal supporting tissues. Am J Orthod 1982;81:12-21. [ Links ]
11. Giron de Velasco J. Cambios óseos y dentarios con disyunción y quad-hélix: estudio comparativo de una muestra de 41 pacientes. Rev Esp Ortod 2005; 45:64-73. [ Links ]
12. Cervera-Sabater A, Simon-Pardell M. Quad-Helix. Biomecánica básica. Rev Esp Ortod 2002;32:253-62. [ Links ]
13. Haas JA. Palatal expansion: Just the beginning of dentofacial orthopedics. Am J Orthod 1970;57:219-55. [ Links ]
14. Asher C. The removable Quadhelix appliance. Br J Orthod 1985;12:40-5. [ Links ]
15. Jones SP, Waters NE. The quadhelix maxillary expansion appliance: Part mechanics. Europ J Orthod 1989;11:169-78. [ Links ]
16. Ingerval B, Gölner P, Gebauer U, Frölich K. A clinical investigation of the correction of unilateral first molar crossbite with a transpalatal arch. Am J Orthod Dentofac Orthop 1995;107:418-25. [ Links ]
17. Hass AJ. Rapid expansion of the maxillary dental arch and nasal cavity by opening the midpalatal suture. Angle Orthod 1961;31:73-90. [ Links ]
18. Wertz R. Skeletal and dental changes accompanying rapid midpalatal suture opening. Am J Orthod 1970;58:41-65. [ Links ]
19. Wertz R, Dreskin M. Midpalatal suture opening: a normative study. Am J Orthod 1977;71:367-81. [ Links ]
20. Zimring JF, Isaacson RJ. Forces produced by rapid maxillary expansion. Angle Orthod 1965;35:178-86. [ Links ]
21. Chang JY, McNamara JA, Herberger TA. A longitudinal study of skeletal side effects induced by rapid maxillary expansion. Am J Orthod Dentofac Orthop 1997; 112:330-37. [ Links ]
22. Linder-Aronson S, Lindgren J. The skeletal and dental effects of rapid maxillary expansion. Br. J Orthod 1979;6:25-9. [ Links ]
23. Ladner PT, Muhl ZF. Changes concurrent with orthodontic treatment when maxillary expansion is a primary goal. Am J Orthod Dentofac Orthop 1995;108:184-9. [ Links ]
24. Majourau A, ,Nanda R. Biomechanical basis of vertical dimension control during rapid palatal expansion therapy. Am J Orthod and Dentofac Orthop 1994;106:322-28. [ Links ]
25. Bell RA, LeCompte EJ. The effects or maxillary expansion using quad-helix appliance during the deciduous and mixed dentitions Am J Orthod 1981;79:152-61. [ Links ]
26. Mossaz-Joelsön K, Mossaz CF. Show maxillary expansion: a comparison between banded and bonded appliances. Eur J Orthod 1989;11:67-76. [ Links ]
27. Thailander B, Wahlund S, Lennartsson B. The effect of early interceptive treatment in children with posterior cross-bite. Eur J Orthod 1984;6:25-34. [ Links ]

