










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
versión On-line ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.12 no.1 ene. 2007
Primary leiomyosarcoma of the mandible. A case report
João de Jesus Viana Pinheiro 1, Sérgio de Melo Alves 2, Edson Okuda 3,
Waldir Antonio Jorge 4, Ruy Gastaldoni Jaeger 5, Ney Soares de Araújo 6
(1) DDS, PhD, Universitary Hospital João de Barros Barreto, Department of Oral Pathology, School of Dentistry, Federal University of Pará
(2) DDS., MS. Department of Estomatology, School of Dentistry, University Center of Pará
(3) DDS, Oral and Maxillofacial Surgery Clinic, São Paulo Tatuapé Hospital
(4) DDS, PhD, Department of Stomatology, School of Dentistry, São Paulo University
(5) DDS, PhD, Department of Histology and Embryology, Institute of Biomedical Sciences, São Paulo University
(6) DDS, PhDe Department of Oral Pathology, School of Dentistry, São Paulo University
ABSTRACT
The aim of this article is to describe a case of leiomyosarcoma of the mandible with immunohistochemical analysis that was useful in making the final diagnosis.
A 40-year-old woman was referred to the Stomatology Clinic of São Paulo Tatuapé Hospital, , for evaluation of a lesion on the left side of the mandible. This lesion presented a fast growth in the last 6 months. Intraoral examination showed a firm, fixed, red colored mass measuring, approximately 60-mm in diameter. No lymph nodes involvement was found. The radiographic examination showed a lytic lesion showed ill-demarcated radiolucent with facial and lingual cortical bone destruction. Microscopic examination of the mandibular lesion showed a neoplasm composed by interlacing fascicles of spindle-shaped cells. Most of the cells presented a blut-ended elongated shape. A marked cellular pleomorphism was observed, represented by cells with irregular shape and abundant eosinophilic cytoplasm. Nuclei were large, hyperchromatic, either vacuoled or cigar-shape. The cytoplasm of the cells stained red with Massons trichrome stain. Neoplastic cells expressed vimentin, smooth-muscle actin, HHF-35 and desmin. These findings were consistent with the diagnosis of leiomyosarcoma.
Key words: Imunohistochemical, leiomyiosarcoma, mandible.
Introduction
Leiomyosarcoma makes up 6 to 7% of all soft tissue sarcomas. This neoplasm of smooth muscle is more common in older adult population and most often arises in the uterus, gastrointestinal tract, and the retroperitonial region(1). Women are more affected than men because of the uterine association. The prognosis is poor, with a hight percentage of recurrence or metastasis. The most common sites of metastasis include the lungs, bone, brain and the lymph node. This neoplasm, is a extremely rare mesenchymal lesion in the oral cavity, with unusual bone location because of paucity of smooth muscle in that site(2). However, the definitive histologic diagnosis of leiomyosarcoma is difficult because of the similarity with other spindle-cell sarcomas(1). The immunohistochemical analysis for cytoesqueletal proteins such as actin, vimentin, desmin, HHF-35 and ultrastructural examination has been widely used for the diagnosis of leiomyosarcoma(3).
The aim of this article is to describe a case of leiomyosarcoma of the mandible with immunohistochemical analysis that was useful in making the final diagnosis.
Case report
A 40-year-old woman was first seen with a lesion on the left mandible. This lesion had demonstrated rapid growth during the last 6 months. Intra oral examination showed a firm, fixed, red colored mass measuring 60-mm in diameter. No lymph nodes involvement was found.
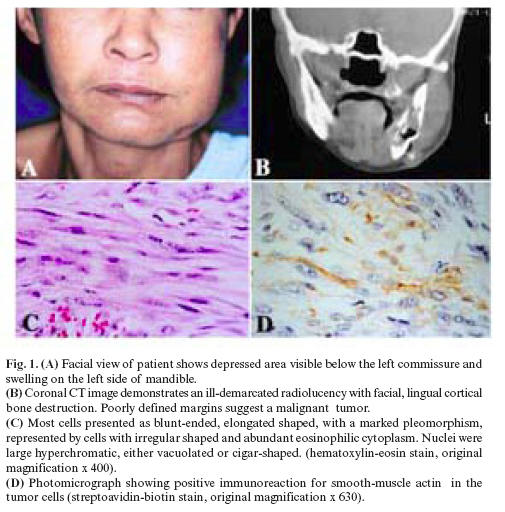
A biopsy was performed under local anesthesia. The specimen was fixed in formalin, parafin embedded and stained by hematoxylin-eosin. A diagnosis of an inflammatory chronical process with desmoplasia of the connective tissue was made. Due to the clinical appearance of the lesion, it was suggested that the biopsy should be repeated, in order to obtain a more representative sample. Unfortunately, the patient returned one month later, with a pronounced enlargement of the left side of the mandible with depressed area, (Fig. 1A). No fistula or discharge were observed and all the teeth in the region were vital. At this point the patient reported pain. In addition, the computed tomographic imaging showed a lytic, ill-demarcated radiolucency lesion with facial and lingual cortical bone perfuration. The medular bone was destroyed, there was calcification into tumor masss and expansion of soft tissue. The Poorly defined margins suggest a malignant tumor. (Fig. 1 B).
The rapid onset of a painful left mandibular swelling, lacking signs of infection or inflamation, along with radiographic features of facial and lingual bone destruction suggested malignancy. For a patient at this age and sex, primary and metastatic malignancies in mandibular bone should be considered. The differential diagnosis could include soft tissue sarcomas, osteosarcoma and condrosarcoma.
The patient was admitted at São Paulo Tatuapé Hospital for an emergency surgery. Another incisional biopsy was performed.
Microscopic examination of the mandibular lesion showed a neoplasm composed of interlacing fascicles of spindle-shaped cells . Most of the cells were blunt-ended and elongated shaped. A marked cellular pleomorphism was observed, represented by cells with irregular shape and abundant eosinophilic cytoplasm. Nuclei were large, hyperchromatic, either vacuolated or cigar-shaped (Fig. 1C). Mitotic figures could occasionally be identified (less than of 2 per 10 high power fields). The tumor exhibited hemangioperycitoma-like areas. Few giant cells were present. Necrotic areas were noted. Immunohistochemistry was carried out through the streptoavidin biotin method (LSAB, Dako Corporation Carpinteria CA USA ). The antibodies used were anti-vimentin (1:200 Tris-HCl), anti-smooth-muscle actin (1:50 Tris-HCl), anti-HHF35 (1:50 Tris-HCl), anti-desmin (1:100 Tris-HCl), anti-S100 protein (1:400 Tris-HCl), anti-CD-34 (1:50 Tris-HCl), h-caldesmon (1:100 Tris-HCl). All antibodies were from Dako (Dako NS, Glostrup, Denmark), except the anti-CD34, purchased from Novocastra (Novocastra, Newcastle, UK). Neoplastic cells expressed vimentin, HHF-35, desmin, h-caldesmon and smooth-muscle actin (Fig. 1D). These findings were consistent with the diagnosis of leiomyosarcoma.
The hemimandibullectomy was the chosen treatment for the present case. The patient has been followed for 11 months and no local recurrence has been observed. The cervical and submandibular regions remain free of palpable lymph nodes. Systemic examinations revealed no other site affected by this malignant neoplasm. The neoplasm in question was a primary leyomiosarcoma of the mandible.
Discussion
The leiomyosarcoma has been divided into three main groups based on geographic occurrence: 1) retroperitoneal and intra-abdominal; 2) cutaneous and subcutaneous; and 3) vascular. Each group has certain clinical and biological differences, althought, they are histologically similar. The site of the leiomyosarcoma is more important for prognosis than its histological features. Those arising in a superficial cutaneous localization have the best prognosis (1).
Intraoral leiomyosarcoma occurs predominantly in males with a ratio of 2:1 and may present at any age, (2) ranging from 1 to 88 years (3-5). The mean age of the 10 previously described patients with leiomyosarcoma arising from jaw bone was 43.8 years (6). The patient of the present case is a woman of 40 years with a primary lesion at the mandible.
Farman (7) found only 5 oral cases among 7,748 benign smooth-muscle tumors of the whole body. In a review of the literature, in 1977, by Farman and Key (8), 11 cases of primary leiomyosacomas in the jaws or in the oral cavity were located. A total of 30 cases of primary leiomyosarcoma in the oral cavity have been described during the last 75 years (6, 9-13). The intraoral locations of these tumors were as follows: cheek (5), mandible (8), gingiva (4), maxilla (4), floor of the mouth (3), tongue (3), soft palate (2), hard palate mucosa (1) (7, 13).
In the oral cavity, the jaw bones have been the most prevalent location for this tumor, accounting for 45% of all reported cases. Including the current case, only 9 cases have been reported in the mandible (7, 13). There is no distinct clinical feature that may suggest the presence of oral leiomyosarcoma. These tumors can appear as a painless, well-circunscribed mass, firmly adherent to the surrounding tissues (3).
Histopathologically, this neoplasm is characterized by sheets of sweeping, alternating bundles and fascicles of densely packed spindle cells with abundant fibrillar eosinophilic cytoplasm and indisctinct cytoplasmic borders. The nucleus is usualy centrally located and blunt-ended, squared-off or cigar-shaped. Occasional cells have perinuclear vacuoles (1,9,14,15). In some cases, nuclear hyperchromasia, and pleomorphism are pronounced. Both typical and atypical mitosis, as few as one or as many as 20 per high-power field populate the tumor (9,11). The diagnosis of soft tissue tumors of mesenchymal origin can be very difficult and necessitates differentiation from a number of other tumors (16,17). Massons trichrome staining and immunohistochemial evaluation for muscle antigens are helpful in diagnosis separating leiomyosarcoma from other sarcomas (18). Positive reactions for desmin, vimentin, smooth-muscle actin and h-caldesmon have been demonstrated in this neoplasm (3, 19-21).
The case presented fulfilled these criteria and confirmed the diagnosis of leiomyosarcoma.
Surgical resection, hemimandibullectomy or hemimaxillectomy, partial maxillectomy, are the prefered initial treatments for cases of leiomyosarcoma primary in the jawbones (13, 15). Regional lymph node investigation is recommended if there is clinical evidence of lymphadenopathy (21).
A hemimandibullectomy was the treatment of the choice in the present case. The patient has been following by 11 months and no local recurrence has been observed. The cervical and sumandibular regions remain free of palpable lymph nodes. Systemic examinations revealed no other site affected by this malignant neoplasm.
To summarize our report, we should emphasize the importance of an early diagnosis on the survival of the patient. This diagnosis can only be achieved if a representative fragment of the lesion is obtained. In addition, immunohistochemistry was very important to establish a final diagnosis of leiomyosarcoma.
References
1. Enzinger FM, Weis SW, eds. Soft Tissue Tumors: St. Louis, MO, Mosby Year Book Inc; 1995. p. 491-510. [ Links ]
2. Schenberg ME, Slootweg PJ, Koole R. Leiomyosarcoma of the oral cavity. Report of four cases and review of the literature. J Craniomaxillofac Surg 1993;21:342-7.
3. Izumi K, Maeda T, Cheng J, Saku T. Primary leiomyosarcoma of the maxila with regional lymph node metastasis: Report of a case and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995;80:310-9.
4. Freedman PD, Jones AC, Kerpel SM. Epithelioid leiomyosarcoma of the oral cavity: Report of two cases and review of the literature. J Oral Maxillofac Surg 1993;51:928-32.
5. Haedicke G, Kaban LB. Smooth-muscle tumors of the oral cavity. Plast Reconstr Surg 1988;81:264-9.
6. Carter LC, Aguirre A, Boyd B, DeLacure MD. Primary leiomyosarcoma of the mandible: Report of a case and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;87:477-84.
7. Farman AG. Benign smooth-muscle tumours. S Afr Med J 1975; 49:1333-408.
8. Farman AG, Key S. Oral leiomyosarcoma: Report of a case and review of the pertainnig to smooth-muscle tumors of the oral cavity. Oral Surg Oral Med Oral Pathol 1977;43:402-9.
9. Bass B, Archard H, Sussman R, Stern M. Saunders V. Clinicopathologic conferences, case 62: expansile radiolucent lesion of the mandible. J Oral Maxillofac Surg 1986;44:799-803.
10. Nishi M, Mimura T, Senba I. Leiomiosarcoma of the maxila. J Oral Maxillofac Surg 1987;45:64-8.
11. Poon CK, Kwan P-C, Yin N-T. Leiomyosarcoma of gingiva: Report of a case and review of the lierature. J Oral Maxillofac Surg 1987;45:888-92.
12. Mindel RS, Calcaterra TC, Ward PH. Leiomyosarcoma of the head and neck: A review of the literature and report of two cases. Laryngoscope 1975;85:902-10.
13. Karlis V, Zaslow M, Minkowitz G, Glickman RS. Leiomyosarcoma of the mandible: Report of a case and literature review. J Oral Maxillofac Surg 1996;54:1127-30.
14. Allen CM, Neville B, Damm DD, Marsh W. Leiomyosarcoma metastatic to oral region: Report of three cases. Oral Surg Oral Med Oral Pathol 1993;76:752-6.
15. Kratochvil FJ, MacGregor SD, Budnick SD, Hewan-Lowe K, Allsup H. Leiomyosarcoma of the maxila: Report of a case and review of the literature. Oral Surg Oral Med Oral Pathol 1982;54:647-55.
16. Lloria-Benet M, Bagan JV, Lloria de Miguel E, Borja-Morant A, Alonso S. Oral leiomyoma: a case report. Med Oral 2003;8:215-9.
17. Sanchez Jimenez J, Dean Ferrer A, Alamillos Granados F, Ruiz Masera JJ, Villar Pastor C, Garcia Lopez A, Penalba Manegold M. Adult rhabdomyoma in the masticatory area. New case presentation and review of the literature. Med Oral 2001;6:64-8.
18. Lack EE. Primary leiomyosarcoma of adrenal gland. Case report with immunohistochemical and ultrastructural study. Am J Surg Pathol 1991;15:899-905.
19. Lo Muzio L, Favia G, Mignogna MD, Piattelli A, Maiorano E. Primary intraoral leiomyosarcoma of the tongue: An immunohistochemical study and review of the literature. Oral Oncol 2000;36:519-24.
20. Mesquita RA, Migliari DA, De Souza SOM, Alves MR. Leiomyosarcoma of the buccal mucosa: A case report. J Oral Maxillofac Surg 1998;56:504-7.
21. Watanabe K, Kusakabe T, Hoshi N, Saito A, Suzuki T. h-Caldesmon in leiomyosarcoma and tumours with smooth muscle cell-like differentiation: its specific expression in the smooth muscle cell tumor. Hum Pathol 1999;30:392–6.
![]() Correspondence:
Correspondence:
Dr. João de Jesus Viana Pinheiro
Av. Almirante Wandenkolk, 1243, 1006
Umarizal. Belém-Pará-Brazil – ZIP Code: 66050-030
E-mail: radface@hotmail.com
Received: 1-10-2005
Accepted: 20-05-2006

