










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
versión On-line ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.12 no.5 sep. 2007
Florid cemento-osseous dysplasia: A case report
Saadettin Dagistan1, Ümmühan Tozoglu2, Mustafa Göregen2, Binali Çakur1
(1) DDS phD
(2) DDS. Department of Oral Diagnosis and Oral Radiology, Faculty of Dentistry, Atatürk University, Erzurum, Turkey
ABSTRACT
Cemento-osseous dysplasias are a group of disorders known to originate from periodontal ligament tissues and involve, essentially, the same pathological process. They are usually classified, depending on their extent and radiographic appearances, into three main groups: periapical (surrounds the periapical region of teeth and are bilateral), florid (sclerotic symmetrical masses) and focal (single lesion) cemental dysplasias. Florid cemento-osseous dysplasia clearly appears to be a form of bone and cemental dysplasia that is limited to jaws. Patients do not have laboratory or radiologic evidence of bone disease in other parts of the skeleton.
For the asymptomatic patient, the best management consists of regular recall examinations with prophylaxis and reinforcement of good home hygiene care to control periodontal disease and prevent tooth lose. Management of the symptomatic patient is more difficult. At this stage, there is an inflammatory component to the disease and the process is basically a chronic osteomyelitis involving dysplastic bone and cementum. Antibiotics may be indicated but may not be effective.
A case of florid cemento-osseous dysplasia occurring in a 47-year-old Caucasian female is reported which was rare in regard to race and sex.
Key words: Florid cemento-osseous dysplasia, gigantiform cementoma, familial multiple cementomas.
Introduction
Florid cemento-osseous dysplasia is more commonly seen in middle-aged black women (in some series, more than 90 percent of patients), although it also may occur in Caucasians and Asians (1). The reason for this racial and gender predilection is unknown (2). In some cases, a familial tendency has been reported, but most examples appear to represent isolated instances (3). The lesions show a marked tendency for bilateral and often quite symmetric involvement, and it is not unusual to encounter extensive involvement of all four posterior quadrants. The process may be totally asymptomatic and, in such cases, the lesion is detected when radiographs are taken for some other purposes. Symptoms such as dull pain or drainage are almost always associated with exposure of sclerotic calcified masses in the oral cavity. This may occur as the result of progressive alveolar atrophy under a denture or after extraction of teeth in the affected area (4). Radiographically, the lesions appear as multiple sclerotic masses, located in two or more quadrants, usually in the tooth-bearing regions. They are often confined within the alveolar bone (5). Histologically, these lesions are composed of anastomosing bone trabeculae and layers of cementum-like calcifications embedded in a fibroblastic background. Management of florid cemento-osseous dysplasia may be difficult and not very satisfactory. The disease may persist for indefinite periods of time without causing any symptoms. For the asymptomatic patient, the best management consists of regular recall examinations with prophylaxis and reinforcement of good home hygiene care to control periodontal disease and prevent tooth loss. Because the onset of symptoms is usually associated with exposure of the sclerotic masses to the oral cavity, biopsy or elective extraction of teeth should be avoided. Indeed biopsy increases the risk of infection or fracture of the jaw and it is not normally justified to surgically remove these lesions, as this often requires extensive surgery(6).
Case Report
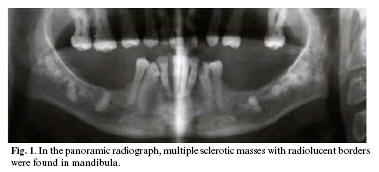
A 47-year-old Caucasian female presented for dental care. She was systemically healthy and extra-oral examination was within normal limits. Intraoral examination revealed a partially edentulous area and the overlying gingiva and mucosa were normal without any clinical signs of inflammation. Panoramic and periapical radiographs were obtained. A biopsy is not required to confirm the diagnosis as this is usually established radiographically. Indeed biopsy increases the risk of infection or fracture of the jaw and it is not normally justified to surgically remove these lesions, as this often requires extensive surgery. In the panoramic radiograph, multiple sclerotic masses with radiolucent borders were found in mandibula (Fig 1). Periapical radiographs, periapical regions of lower right first molar and premolar and lower left first molar and premolar teeth, confined within the alveolus at a level corresponding to the roots of the teeth, above the inferior alveolar canal (Fig 2).

Discussion
Florid cemento-osseous dysplasia was first described by Melrose et al. in 1976 (1).This condition has been interpreted as a dysplastic lesion or developmental anomaly arising in tooth-bearing areas. These lesions exhibit a sclerotic appearance similar to that of other lesions on conventional radiographs. Histopathologically, it is a benign fibro-osseous lesion that must be differentiated from other benign fibro-osseous lesions such as fibrous dysplasia, ossifying fibroma, Pagets disease, and sclerosing osteomyelitison on the basis of combined clinical, radiographic, and histological features. However, this lesion do not appear to be developmental in nature such as fibrous dysplasia (7), nor do it show the characteristics of neoplasia such as ossifying fibroma (8,9). Pagets disease of the bone may have a cotton-wool appearance. However, this condition affects the bone of the entire mandible and shows loss of lamina dura, whereas florid cemento-osseous dysplasia is centered above the inferior alveolar canal and its cervical two thirds are normal (10). Pagets disease is often polyostotic, involving other bones such as spine, femur, skull, pelvis and sternum (11) and produces biochemical serum changes, such as elevated alkaline phosphate levels (12). No biochemical alterations and others bone involvement were found in the case reported.
In the past these calcifications have been interpreted as chronic diffuse sclerosing osteomyelitis; Schneider and Mesa(13) reported two cases of each condition as they tried to demonstrate any differences between them. Chronic diffuse sclerosing osteomyelitis is a primary inflammatory condition of the mandible presenting with cyclic episodes of unilateral pain and swelling and shows a single area of diffuse sclerosis containing small, ill-defined osteolytic areas. whereas florid cemento-osseous dysplasia is seen as multiple round or lobulated opaque masses. Chronic diffuse sclerosing osteomyelitis involves the body of the mandible from the alveolus to the inferior border and may extend into the ramus. Florid cemento-osseous dysplasia has been interpreted as a dysplastic lesion or developmental anomaly arising in tooth-bearing areas. In addition, florid cemento-osseous dysplasia is frequently associated to black women, while chronic diffuse sclerosing osteomyelitis is seen predominantly in adult Caucasian men (6,14).
Florid cemento-osseous dysplasia may have similarities with jaw bone changes in familial adenomatosis coli (Gardners syndrome)(15), but florid cemento-osseous dysplasia has no other skeletal changes or skin tumours or even the dental anomalies that are seen in this syndrome.
Florid cemento-osseous dysplasia may be familial with an autosomal dominant inheritance pattern, but there are only a few examples in the literature in which the familial pattern has been confirmed (1,3). In the present case no familial aspects of the disease could be established.
Conclusion
Normally, a diagnosis of florid cemento-osseous dysplasia in the jaws is made by clinical findings, radiographic features and histology. However, florid cemento-osseous dysplasia is a condition in which the diagnosis relies on radiology and clinical findings alone. As reassuring as a biopsy might be, in this situation it may precipitate infection that is difficult to control without extensive surgical intervention.
References
1. Gonçalves M, Pispico R, Abreu Alves F, Lugão CB, Gonçalves A. Clinical, radiographic, biochemical and histological findings of florid cemento-osseous dysplasia and report of a case. Braz Dent J 2005;16:247–50. [ Links ]
2. Neville BW, Damm DD, Allen CM, Bouquot JE, eds. Oral and Maxillofacial Pathology. W.B. Saunders Company Philadelphia; Pennsylvania:1995. p. 531–3. [ Links ]
3. Toffanin A, Benetti R, Manconi R. Familial florid cemento-osseous dysplasia: a case report. J Oral Maxillofac Surg 2000;58:1440–6. [ Links ]
4. Said-al-Naief NA, Surwillo E. Florid osseous dysplasia of the mandible: report of a case. Compend Contin Educ Dent 1999;20:1017–9. [ Links ]
5. Damm DD, Fantasia JE. Multifocal mixed radiolucencies. Florid cemento-osseous dysplasia. Gen Dent 2001;49:461,538. [ Links ]
6. Smith S, Patel K, Hoskinson AE. Periapical cemental dysplasia: a case of misdiagnosis. Br Dent J 1998;185:122–3. [ Links ]
7. Farzaneh AH, Pardis PM. Central giant cell granuloma and fibrous dysplasia occuring in the same jaw. Med Oral Patol Oral Cir Bucal 2005;10 Suppl 2:El 30–2. [ Links ]
8. Perez-Garcia S, Berini-Aytes L, Gay-Escoda C. Ossifying fibroma of the upper jaw: report of a case and review of the literature. Med Oral 2004;9:333–9. [ Links ]
9. Galdeano Arenas M, Crespo Pinilla JI, Alvarez Otero R, Espeso Ferrero A, Verrier Hernandez A. Cemento-ossifying fibroma of mandibular gingiva: single case report. Med Oral 2004;9:176–9. [ Links ]
10. Langlais RP, Langland OE, Nortjé CJ,eds. Diagnostic Imaging of the Jaws. Malvern: Williams & Wilkins; 1995. [ Links ]
11. White SC, Pharoah MJ,eds. Oral Radiology - Principles and Interpretation. Saint Louis: Mosby; 2000. [ Links ]
12. Loh FC, Yeo JF. Florid osseous dysplasia in Orientals. Oral Surg Oral Med Oral Pathol 1989;68:748–53. [ Links ]
13. Schneider LC, Mesa ML. Differences between florid osseous dysplasia and chronic diffuse sclerosing osteomyelitis. Oral Surg Oral Med Oral Pathol 1990;70:308–12. [ Links ]
14. Groot RH, van Merkesteyn JP, Bras J. Diffuse sclerosing osteomyelitis and florid osseous dysplasia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996;81:333–42. [ Links ]
15. Wolf J, Hietanen J, Sane J. Florid cemento-osseous dysplasia (gigantiform cementoma) in a Caucasian woman. Br J Oral Maxillofac Surg 1989;27:46–52. [ Links ]
![]() Correspondence:
Correspondence:
Dr. Binali Çakur
E-mail: bcakur@atauni.edu.tr
Received: 30-10-2006
Accepted: 25-03-2007

