










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
On-line version ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.12 n.8 Dec. 2007
Plasmacytoid myoepithelioma of the palate. Report of one case and review of the literature
Florence Cuadra Zelaya1, Daniel Quezada Rivera1, José Luis Tapia Vazquez1, Carlos Paez Valencia2, Luis Alberto Gaitán Cepeda1
(1) Oral Pathology Laboratory, Postgraduate and Research Division, Dental School, National Autonomous University of Mexico
(2) Pathology Service, Hospital General "20 de Noviembre", ISSSTE, México city, México
ABSTRACT
Introduction: Myoepithelioma is a benign neoplasm of salivary glands, represents 1.5 % of all salivary glands neoplasm. The plasmacytoid myoepithelioma from palate salivary glands is considered as a rare entity, at date it has been reported 14 cases. It is present one case of plasmacytoid myoepithelioma of palate. Case report: A Hispanic female of 28 years old presented a not-ulcerate, painless ovoid swelling at left side of hard palate with a one year and a half of evolution. An excisional biopsy was done. The sample was fixed at 10% buffer formalin, embedded in paraffin, cuts at 5 µ and stained with H-E. Microscopically, the lesion was composed by myoepithelial neoplastic cells characterized by a round ovoid silhouette, an eccentric nuclei of dense chromatin and eosinophilic cytoplasm. In some myoepithelial neoplastic cells were identifies intranuclear cytoplasmatic inclusions. The lesion was analysed with immunohistochemical technique using the follow antibodies: vimentin, citokeratin AE1/AE3, S100 protein and actin muscle specific. We observe positive immunoreactivity against vimentin, citokeratin, S100 protein and actin muscle specific. A diagnosis of plasmacytoid myoephitelioma of palate salivary glands was done. Our findings supports the suggestion about plasmacytoid myoepithelioma is an independent entity. The histological diagnostic parameters of plasmacytoid myoepithelioma versus pleomorphic adenoma are discussed.
Key words: Myoepithelioma, plasmacytoid, minor salivary glands, palate, pleomorphic adenoma.
Introduction
Myoepithelioma is a benign neoplasm of salivary glands that represents the 1.5% of all salivary glands neoplasm (1). Their most frequent location is parotid glands. It has not been reported any gender predilection, and their highest frequency is observed at the third decade of life (1). The myoepithelioma is characterized by the proliferation of myoepithelial cells arranged in cords, nests or mantles. On a histological point of view the myoepithelioma is classified in the follow cells types: spindle, plasmacytoid, reticular, epitheliod, and clear, additionally mixed histological form were described (1,2). The most frequent histological variety is the spindle ones (2). The plasmacytoid myoepithelioma from palate salivary glands is considered as a rare entity. To date there have been reported at scientific literature 14 cases of plasmacytoid myoepithelioma of minor salivary glands of palate (3-11). With the objective of contribute to better understanding of this neoplasm we present one case of plasmacytoid myoepithelioma of palate, and additionally we discusses the characteristics of the present case in regard to previously reported cases.
Case report
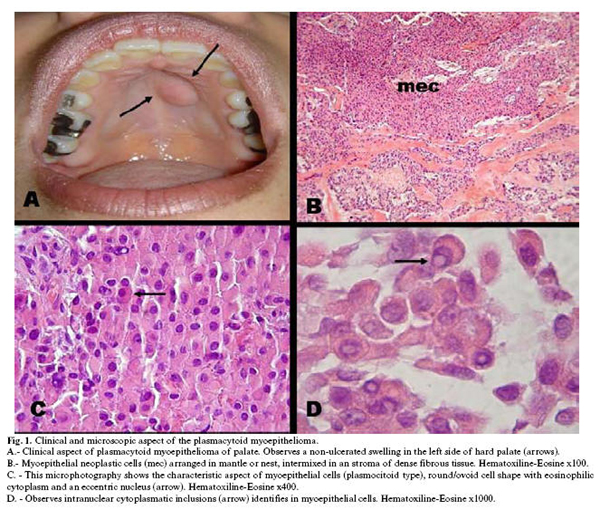
A female of 28 years old, hispanic, was admitted at Oral Medicine Clinic, Postgraduate Division, Dental School, National Autonomous University of Mexico at January of 2005, by the presence of a swelling of hard palate. At oral examination was observed an increase of volume (1 x 1 cm) located at left side of hard palate (Figure 1-A). The lesion was ovoid in shaped, not ulcerate, with a well delimited border. To palpation the tumour was firm and not painful.
The patient was awake of a slow growth of the lesion from the last one year and a half. The medical record shows fibrocystic disease of breast under treatment without complication. The patient was an active smoker of ten cigarettes at day by the last 8 years. With this clinical characteristic, a presumptive clinical diagnosis of benign neoplasm of minor salivary glands compatible with pleomorphic adenoma was done.
The patient was refereed to Oral and Maxillofacial Surgery clinic, at the same institution, for an excisional biopsy. The total of the entity was removed and fixed in 10% buffer formalin and sends to Oral Pathology Laboratory, Postgraduate and Research Division, Dental School, National Autonomous University of Mexico by histopathological diagnosis.
Macroscopically, the specimen was formed by multifragmented soft tissue (1.5 x 1.2 x 0.4 cm), of ovoid shape and irregular surface, whitish to brownish colour. At cut the sample had a solid pattern. After their fixation time (24 hours) all of the fragments of the lesion was processed in a routinely way. The whole sample was cuts at 5 µ. All of the slides were stained with H-E, except 8 slides that were signed to immunohistochemistry technique.
Microscopically, it was observed a lesion compose by myoepithelial neoplastic cells intermixed with a stroma of dense fibrous connective tissue (Figure 1B). The neoplastic cells, as it can observe in figure 1C, showed a round/ovoid silhouette with dense chromatin nucleus located eccentrically and an eosinophilic cytoplasm. In some myoepithelial neoplastic cells we were available to identify intranuclear cytoplasmatic inclusions (Figure 1D). The stroma was formed by collagen fibbers arranged in septum of hyalinised or mixoid aspect. Ductal structures constitute less of 5% of all of the microscopic fields analyzed coming from of all of the sample. With the previous histological characteristics a diagnosis of plasmacytoid myoepithelioma of palate salivary glands was done.
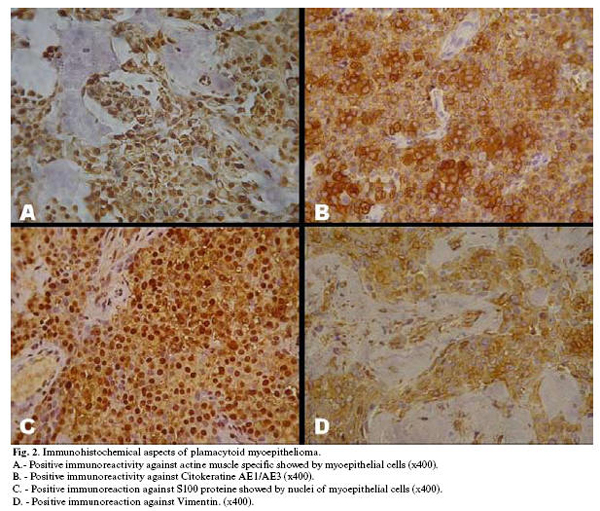
To corroborate the myoepithelial nature of the neoplastic cells and with the objective of a better understanding of this neoplasm, the sample was analysed with immunohistochemical technique. The antibodies used were: anti-actin muscle specific, anti-cytokeratin AE1/AE3, anti-S100 protein and anti-vimentin. As the figure 2 shows, we observe positive immunoreactivity of myoepithelial cells against actine muscle specific (Figure 2A) and against Cytokeratine AE1/AE3 (Figure 2B). The nuclei of plasmacytoid myoepithelial neoplastic cells show positive immunoreaction against S100 protein (Figure 2C). A strong inmunoreactivity in the cytoplasm of neoplastic cells against vimentin was observes (Figures 2D).
Discussion
At date, and in our knowledge, it has been reported 15 cases, including the present one, of plasmacytoid myoepithelioma from palate (3-11). In spite of not gender preference has been reported, the analysis of cases reported at scientific literature, shows a male:female ratio of 1:2 (5 male: 9 female). It has been reported that the highest prevalence of plasmacytoid myoepithelioma is observes at third decade of life (1). However, the average of age of all the reported cases is 36.3 years, and their highest prevalence is ubiquities at second decade of life. The demographic data of the previously reported cases of plasmacytoid myoepithelioma from palate are shown in Table 1.
The plasmacytoid type of 1myoepithelioma is characterized by groups of myoepithelial cells closely packed or arranged in cordons, nests or mantles. The cytoarchitecture of myoepithelial plasmacytoid neoplastic cells includes round, ovoid, poliedric cells with eccentric nucleus and eosinophilic cytoplasm (1-2). All of this cellular characteristics were identifies in the present case. It has been described that some myoepithelial cells shows a nuclear crevice and some times the cells shows intranuclear cytoplasmic inclusions (12); again this characteristics were observed in our case, (Figure 1D.)
Although it has been proposed specific diagnostic criteria to differentiate the myoepithelioma from pleomorphic adenoma, controversy is arising in this issue. Sciubba and Brannon (13) consider to myoepithelioma as a subtype or final spectrum of pleomorphic adenoma, because their biological behaviour and distribution. On the other hand, World Health Organization classifies to myoepithelioma as an independent entity (1). In such a way, it has been proposed that if the neoplasm contains less of 5% of ductal and acinar components must be named myoepithelioma (1,14).
To establish specific percentages like 5% or 10% of determinate histological component could be subjective for each observer. However this quantitative parameter constitutes the diagnostic parameter accepted to establish a differential diagnosis between pleomorphic adenoma rich in myoepithelial cells and plasmacytoid myoepithelioma. On the other hand a diagnostic parameter based in cellular predominance could be an alternative to be considered. We suggest if there is myoepithelial predominance should be named myoepithelioma and if there is ductal predominance a pleomorphic adenoma diagnosis should be establish. However until this suggestion will be confirm or reject by other research groups the percentage of the ductal structures should be considered the principal diagnostic parameter of plasmacytoid myoepithelioma of salivary glands versus pleomorphic adenoma rich in myoepithelial cells.
Immunohistochemical studies have been revealed that myoepithelial neoplastic cells show variable immunoreactivity related to cell phenotype. It has been reported positive immunoreactivity against S100 protein, cytokeratin, cytokeratin 14, actin muscle specific, vimentin and fibrilar glycoprotein (7,8,14-16). On the other hand it has been reported negative immunoreactivity against actine muscle specific (15). In our case we observe positive immunoreactivity to actin muscle specific, vimentin, cytokeratin AE1/AE3 and S100 protein.
The first choice treatment for plasmacytoid myoepithelioma is surgical excision with margin of healthy borders. The potential of recurrence of myoepithelioma is low (13). At date of the present report (18 months) our patient has not show any signs of recurrence.
In base of our findings we suggest that plasmacytoid myoepithelioma of palate is an independent entity that should be included in the differential diagnosis of neoplasm of palatine glandular salivary.
References
1. Cardesa A, Alos L. Myoepithelioma. In: Barnes L, Everson JW, Reichert P, Sidransky D, eds. Pathology and Genetics of Head and Neck Tumours. Tumours of the Salivary Glands. World Health Organization. Lyon, France: IARC Press; 2005. p. 259-60. [ Links ]
2. Dardick I, Thomas MJ, Van Nostrand AW. Myoepithelioma--new concepts of histology and classification: a light and electron microscopic study. Ultrastruct Pathol. 1989 Mar-Jun;13(2-3):187-224. [ Links ]
3. Barnes L, Appel BN, Perez H, El-Attar AM. Myoepithelioma of the head and neck: case report and review. J Surg Oncol. 1985 Jan;28(1):21-8. [ Links ]
4. Lins JE, Gnepp DR. Myoepithelioma of the palate in a child. Int J Pediatr Otorhinolaryngol. 1986 Feb;11(1):5-13. [ Links ]
5. Nesland JM, Olafsson J, Sobrinho-Simoes M. Plasmacytoid myoepithelioma of the palate. J Oral Pathol. 1981 Feb;10(1):14-21. [ Links ]
6. Kanazawa H, Furuya T, Watanabe T, Kato J. Plasmacytoid myoepithelioma of the palate. J Oral Maxillofac Surg. 1999 Jul;57(7):857-60. [ Links ]
7. Lopez JI, Ugalde A, Arostegui J, Bilbao FJ. Plasmacytoid myoepithelioma of the soft palate. Report of a case with cytologic, immunohistochemical and electron microscopic studies. Acta Cytol. 2000 Jul-Aug;44(4):647-52. [ Links ]
8. Acikalin MF, Pasaoglu O, Cakli H, Ciftci E. Plasmacytoid myoepithelioma of the soft palate: a review of the literature and report of a case with immunohistochemical findings. Kulak Burun Bogaz Ihtis Derg. 2005 May-Jun;14(5-6):127-30. [ Links ]
9. Taylor J, Tighe JV. A minor salivary gland tumour presenting with dysphagia. J Laryngol Otol. 1999 Jun;113(6):569-72. [ Links ]
10. Katsuyama E, Kaneoka A, Higuchi K, Takasu K. Myoepithelioma of the soft palate. Acta Cytol. 1997 Nov-Dec;41(6):1856-8. [ Links ]
11. Nwoku AL, Al-Shlash S, Al-Atel A. Pediatric myoepithelioma of the palate. Saudi Med J. 2005 Jun;26(6):999-1002. [ Links ]
12. Das DK, Haji BE, Ahmed MS, Hossain MN. Myoepithelioma of the parotid gland initially diagnosed by fine needle aspiration cytology and immunocytochemistry: a case report. Acta Cytol. 2005 Jan-Feb;49(1):65-70. [ Links ]
13. Sciubba JJ, Brannon RB. Myoepithelioma of salivary glands: report of 23 cases. Cancer. 1982 Feb 1;49(3):562-72. [ Links ]
14. Dardick I, Cavell S, Boivin M, Hoppe D, Parks WR, Stinson J, et al. Salivary gland myoepithelioma variants. Histological, ultrastructural, and immunocytological features. Virchows Arch A Pathol Anat Histopathol. 1989;416(1):25-42. [ Links ]
15. Takai Y, Dardick I, Mackay A, Burford-Mason A, Mori M. Diagnostic criteria for neoplastic myoepithelial cells in pleomorphic adenomas and myoepitheliomas. Immunocytochemical detection of muscle-specific actin, cytokeratin 14, vimentin, and glial fibrillary acidic protein. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995 Mar;79(3):330-41. [ Links ]
16. Ponce Bravo S, Ledesma Montes C, López Becerril U, Morales Sánchez I. Myoepithelial cells are the main component in pleomorphic adenomas. Med Oral Patol Oral Cir Bucal. 2007 Mar 1;12(2):E110-5. [ Links ]
![]() Correspondence:
Correspondence:
Dr. Luis Alberto Gaitán Cepeda
Laboratorio de Patología Clínica y Experimental.
División de Estudios de Postgrado e Investigación,
Facultad de Odontología, Universidad Nacional Autónoma de México.
Circuito Institutos s/n, Ciudad Universitaria, Coyoacán 04510,
México, D.F.
México
E-mail: lgaitan@servidor.unam.mx
Received: 5-1-2007
Accepted: 1-08-2007

