










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
versão On-line ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.12 no.8 Dez. 2007
New dental simulator for microsurgical training preliminary overview
Jesús Usón Gargallo1, Elena Abellán Rubio1, José Luis Gutiérrez Pérez2, Daniel Torres Lagares3, Carmen Calles Vázquez1
(1) Microsurgery Unit. Minimally Invasive Surgery Centre. Cáceres
(2) Head of the Maxillofacial Surgery Department, Virgen del Rocío University Hospitals. Professor of Oral Surgery. Faculty of Dentistry. University of Seville. Seville
(3) Assistant Lecturer of Oral Surgery. University of Seville. Seville. Spain
ABSTRACT
Objective: To present a new simulator designed at the Minimally Invasive Surgery Centre (Cáceres) which offers an integral, effective and viable training system that can be used for learning microsurgical techniques.
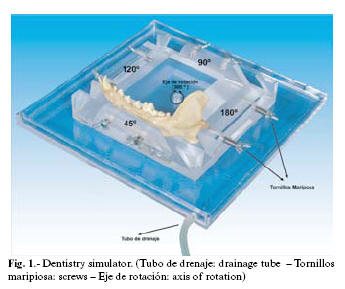
Study design: A square methacrylate block was used. Animal jaws were fixed to the sides by means of butterfly screws. This block also has a drainage tube to facilitate the escape of fluids.
Results: Excellent results were obtained using this simulator in microsurgical suturing training in dental, Oral and Maxillofacial Surgery
Conclusions: We believe that this simulator is an essential component in microsurgical training. It is an ethically and morally valid training method with which various suturing techniques can be practised before using live animals and before applying these to daily clinical practice.
Key words: Microsurgery, training, suturing technique, learning, dental surgery, Oral Surgery, Maxillofacial Surgery.
Introduction
Microsurgery can be defined as "surgery which makes use of magnifying techniques in the operating field to see above the normal range of vision". The Real Academia Española de la Lengua (1989) which regulates the Spanish language defines "micro" as: a quantifier prefix which gives the meaning of "small" to a word. "Surgery" is defined as the section of medicine which aims to cure illnesses by means of surgical operations (1).
Specific surgical material is required to practice microsurgical techniques. This is usually finer and more delicate than that used in conventional surgery: smaller suture material, special needles, and most importantly visual magnifying aids (2-5). The combination of these factors makes it important that the techniques are corrected acquired in an individual manner carrying out continuous practice of the new skills obtained (6-7). In the Minimally Invasive Surgery Centre (MISC), we have designed a simulator (Fig. 1) which reproduces real situations on organic and methacrylate material, using various positions and levels of difficulty in order to learn microsurgical suturing techniques in Dental, Oral and Maxillofacial Surgery. Other training in more advanced techniques can also be acquired in periapical surgery and endodontics in general, avoiding the use of live subjects and in particular, preventing practice on human patients. A more precise simulation is obtained with this simulator since it more closely resembles actual microsurgical techniques in these fields and also requires a more demanding, refined technique.
Material and methods
Description of simulator and instructions for use.
The dental simulator that has been designed in the Minimally Invasive Surgery Centre (Fig. 1) is made up of a 44 mm thick methacrylate square block with four openings to position the jaws of various animals (extracted post-mortem) at varying degrees of inclination: 90º, 105º, 115º and 130º. The jaws are fixed to the sides of the openings of the methacrylate block using butterfly screws (Fig. 1). The simulator also turns 360º on a central axis (rotation axis Fig. 1), in both a clockwise and counter-clockwise direction. This feature, together with the varying degrees of inclination in which the jaws can be positioned, offers numerous positions for practice. Different levels of difficulty and subsequently various real situations in daily clinical practice on human patients can be reproduced.
The methacrylate block is joined to a methacrylate box by a nut which permits the simulator to rotate. It also has a drainage tube to facilitate the escape of fluids (Fig. 1).
Jaws from organic subjects are fixed in various positions to the simulator in order to practice microsurgical suturing techniques and other more advanced techniques in periapical surgery and endodontics in general. This avoids the use of live subjects and especially, practice on human subjects.
Results
The excellent results obtained for this microsurgical suturing training method have proven the success of the simulator. 50 dental, oral and maxillofacial surgeons learned suturing techniques by using this method. All of these were specialists who have attended microsurgical beginners and advanced courses in our Microsurgery Unit, where they practised suturing techniques by carrying out various types of grafts in the simulator.
A further 100 specialists answered a survey, giving their opinions regarding the use of the simulator for initial training of the microsurgical suturing techniques.
All of the abovementioned specialists who have been trained in microsurgical techniques using the practice card1 and subsequently the simulator answered a survey giving their opinions about the advantages or disadvantages of the use of the simulator and whether or not it should be included in the microsurgical training programme within their specialty.
When asked about the importance of time spent using the simulator on a 1-10 score, 90% of the 100 specialists taking the survey answered 10, 6% answered 9, 2% answered 8, and 2% answered 7.
98% of the 100 respondents preferred to begin a one day training course using the dental simulator instead of directly carrying out the techniques on live rats.
Discussion
The simulator used by the Microsurgical Unit of the MISC provides an ethically sound training system which allows trainees to acquire microsuturing techniques without having to learn from mistakes made on live animals. A progressive training system is required, initially using inert material (practice card) (1) and subsequently the dental simulator, since this method also gives better results in the same time frame.
Based on our many years of experience in microsurgical training and on the surveys and statistical studies conducted by the Microsurgical Unit, we conclude that this simulator is a crucial element for learning microsurgical suturing techniques in Dental, Oral and Maxillofacial Surgery. The simulator allows trainees to acquire the skills required and at the same time reduces the number of animals used and the cost. It can therefore be considered an ethical training method (8,9).
Although innate talent plays an important role in acquiring microsurgical suturing skills for their application in these specialties, when the simulator is used, the trainee manages to perform better-quality stitches with greater ease in three or four hours of practice. This may seem difficult at the beginning; but is subsequently beneficial since in our experience, microsurgical techniques can only be mastered after many years of microsurgical training. Furthermore, we should bear in mind that skill in the suturing technique is an essential, decisive factor in microsurgical training (10,11).
References
1. Uson J, Calles MC. Design of a new suture practice card for microsurgical training. Microsurgery. 2002;22(8):324-8. [ Links ]
2. Adrales GL, Chu UB, Witzke DB, Donnelly MB, Hoskins D, Mastrangelo MJ Jr, et al. Evaluating minimally invasive surgery training using low-cost mechanical simulations. Surg Endosc. 2003 Apr;17(4):580-5. [ Links ]
3. Cuschieri, A. No authors listed Training and simulation. Minim Invasive Ther Allied Technol. 2001 Mar;10(2):67-74. [ Links ]
4. DesCoteaux JG, Leclere H. Learning surgical technical skills. Can J Surg. 1995 Feb;38(1):33-8. [ Links ]
5. Haluck RS, Krummel TM. Computers and virtual reality for surgical education in the 21st century. Arch Surg. 2000 Jul;135(7):786-92. [ Links ]
6. Rogers DA, Elstein AS, Bordage G. Improving continuing medical education for surgical techniques: applying the lessons learned in the first decade of minimal access surgery. Ann Surg. 2001 Feb;233(2):159-66. [ Links ]
7. Bro-Nielsen M. Finite element modeling in surgery simulation Proceedings of the IEEE. 1998; 86: 490-503. [ Links ]
8. Wanzel KR, Ward M, Reznick RK. Teaching the surgical craft: From selection to certification. Curr Probl Surg. 2002 Jun;39(6):573-659. [ Links ]
9. Dubrowski A, Carnahan H. Principles of motor learning: Can they be applied to surgical education? FOCUS Surg Ed. 2003; 20: 22-32. [ Links ]
10. Kneebone RL, Scott W, Darzi A, Horrocks M. Simulation and clinical practice: strengthening the relationship. Med Educ. 2004 Oct;38(10):1095-102. [ Links ]
11. Anastakis DJ, Wanzel KR, Brown MH, McIlroy JH, Hamstra SJ, Ali J, et al. Evaluating the effectiveness of a 2-year curriculum in a surgical skills center. Am J Surg. 2003 Apr;185(4):378-85. [ Links ]
![]() Correspondence:
Correspondence:
Dra. Elena Abellán Rubio
Centro de Cirugía de Mínima Invasión "Jesús Usón"
Crta. Nacional 521; Km 41,8 km
10071 Cáceres, SPAIN.
E-mail: eabellan@ccmijesususon.com
Received: 11-1-2007
Accepted: 23-10-2007

