










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
versión On-line ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.12 no.8 dic. 2007
Drill failure during ORIF of the mandible. Complication management
Lipa Bodner1, Yizthak Woldenberg1, Max Puterman2
(1) Department of Oral and Maxillofacial Surgery
(2) Department of Otolaryngology Head and Neack Surgery. Soroka University Medical Center and Ben Gurion University of the Negev, Beer-Sheva, Israel
ABSTRACT
A case of a drill breakage during open reduction and internal fixation (ORIF) of a mandibular fracture is reported. The clinical decision, diagnosis and surgical management of the complication are described.
Key words: Mandible, fracture, fracture fixation, internal, operative complication.
Introduction
The use of ORIF with or without intermaxillary fixation is considered the standard of care for mandibular fractures (1,2) The reported complications of this technology include: malunion, infection, disturbed wound healing, hypoesthesia or paresthesia, impalement of tooth or the inferior alveolar canal and fracture of miniplate (3).
Breakage of surgical instruments, as an intraoperative complication hase been reported sporadically in the orthopedic literature (4,5), where surgical drills account for the most common instrument to be broken (6). We are unaware of reports on drill breakage as an intraoperative complication in oral and maxillofacial surgery, though it is a quite common mishap.
The aim of the present report is to describe an unusual case of a drill breakage during ORIF of a mandibular fracture its diagnosis, operative and postoperative management.
Report of Case
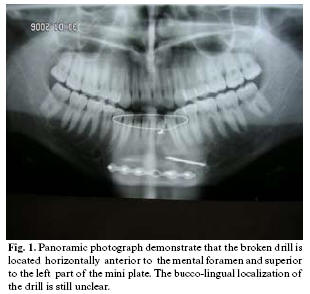
A 20-year-old male patient with a comminuted fracture of the left mandible was scheduled for ORIF under general anesthesia, using a 2.0 mm Craniomaxillofacial Fixation system ( W. Lorenenz Surgical, Jacksonville, Florida, USA). A 1.5 twist drill ( 1.5x115 mm, 37mm Stop, 01-9203) was used to place a 2.0 mm, 6-hole, straight, regular, monocortical mini plate. While drilling at the far left side of the mandible , the drill brok. Attemps to retrieve the drill bit were unsuccessful. This included, creation of a 5 mm hole in the buccal cortex , allowing to insert into the medulla a spoon- shaped excavator , periodontal curette and a magnet. Intraoperative fluoroscope revealed that the broken drill was in situ, but did not enable a precise localization. A clinical decision was made to go ahead with the ORIF procedure and to pospone the retrieval of the drill. Postoperative panoramic radiograph (Fig 1) demonstrated that the drill was located adjacent to the left mental foramen. Axial CT of the mandible (Fig 2) showed that the drill was located partially in the medulla of the mandible but most of its length outside the mandible, extending through the lingual cortex toward the floor of the mouth. Under local anesthesia via a lingual approach the drill was retrieved (Fig 3). The follow up was uneventfull.


Discussion
The application of internal fixation in maxillofacial trauma is among the great advances that have been made in the field. The use of this technique has resulted in many advantages for the patients, however complications can arise (3). The most common complications are malunion, infection / osteitis, paresthesia and iatrogenic piercing of tooth roots or the mandibular canal.
Instrument breakage as an operative complication during ORIF, have been reported in orthopedic surgery, and drill breakage is the most common one (6). The fact that in many trauma centers the drills used for ORIF are re-used, may be in part, the reason for the high breakage rate. It is likely that re-used drills are at increased risk of failure. It was proposed that surgeons should ensure the single use by bending them at the end of each case to prevent re-use (7).
Equipment failure, such as fracture of bicortical screws or fracture of intermaxillary fixation screws have been reported in oral and maxillofacial surgery (8,9). Drill bit breakage was mentioned among the disadvantages of the standart self-tapping screws and the rational for development of the drill free screws (10).
In the present case, the intraoperative attemps to retrieve the broken drill bit were unsuccessful. This was apparently due to lack of adequate imaging that could tell the precise location of the drill. A clinical decision was made that no additional trauma could be justified under these circumstances and the drill was left in situ. The next day and follwing the analysis of the panoramic radiograh and axial CT of the mandible, the precise location of the drill was detemined and consequently the lingual surgical approach, under local anesthesia, was selected and performed succesfully.
How mandatory is it to remove a broken drill ? According to guidelines offered in orthopedic surgery, a broken drill bit that is not in contact with an implant or a screw can be left in situ without any risk of delayed healing. However a drill fragment that is situated near a joint or one that can be easily removed without further trauma to the bone, should be removed. Once the fracture has healed the broken drill bit should be removed along with the implant (11).
It seems that these guidelines, with some adjustments, may be adopted to oral and maxillofacial surgery.
The following guidelines are reccomended:
Ideally, a broken drill should be removed intraoperatively.
The amount of effort to remove the drill intraoperatively, without having optimal imaging, should be restricted to "minor surgery".
The patient should be informed about the complication and the future steps to be taken.
As soon as possible, appropriate imaging modalities (pa-noramic radiograph, occlusal radiograph, axial CT scan) should be performed to determine the precise location of the drill.
A clinical decision should be made, whether or not to remove the drill, based on the following parameters : the length and the exact location, possible future damage if left in situ, proximity to nerves or tooth buds, extent of surgery required for removal, possible iatrogenic damage during the removal and the patients personality and understanding of the situation.
References
1. Dimitroulis G. Management of fractured mandibles without the use of intermaxillary wire fixation. J Oral Maxillofac Surg. 2002 Dec;60(12):1435-8. [ Links ]
2. Mukerji R, Mukerji G, McGurk M. Mandibular fractures: Historical perspective. Br J Oral Maxillofac Surg. 2006 Jun;44(3):222-8. [ Links ]
3. Ellis E 3rd. Complications of rigid internal fixation for mandibular fractures. J Craniomaxillofac Trauma. 1996 Summer;2(2):32-9. [ Links ]
4. Fothi U, Perren SM, Auer JA. Drill bit failure with implant involvement--an intraoperative complication in orthopaedic surgery. Injury. 1992;23 Suppl 2:S17-29. [ Links ]
5. Williams RL, Kunzru KM. A new technique for the removal of a broken cannulated screw. Injury. 1995 Jan;26(1):59-60. [ Links ]
6. Price MV, Molloy S, Solan MC, Sutton A, Ricketts DM. The rate of instrument breakage during orthopaedic procedures. Int Orthop. 2002;26(3):185-7. [ Links ]
7. Ashford RU, Pande KC, Dey A. Current practice regarding re-use of trauma instrumentation: results of a postal questionnaire survey. Injury. 2001 Jan;32(1):37-40. [ Links ]
8. Ellis JA Jr, Laskin DM. Analysis of seating and fracturing torque of bicortical screws. J Oral Maxillofac Surg. 1994 May;52(5):483-6. [ Links ]
9. Coburn DG, Kennedy DW, Hodder SC. Complications with intermaxillary fixation screws in the management of fractured mandibles. Br J Oral Maxillofac Surg. 2002 Jun;40(3):241-3. [ Links ]
10. Heidemann W, Gerlach KL, Gröbel KH, Köllner HG. Drill Free Screws: a new form of osteosynthesis screw. J Craniomaxillofac Surg. 1998 Jun;26(3):163-8. [ Links ]
11. Hirt U, Auer JA, Perren SM. Drill bit failure without implant involvement--an intraoperative complication in orthopaedic surgery. Injury. 1992;23 Suppl 2:S5-16. [ Links ]
![]() Correspondence:
Correspondence:
Prof. Lipa Bodner,
Department of Oral and Maxillofacial Surgery,
Soroka Medical Center,
P.O. Box 151,
Beer-Sheva 84101, Israel.
E-mail: lbodner@bgu.ac.il
Received: 8-02-2007
Accepted: 1-06-2007

