










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkPharmacy Practice (Granada)
versión On-line ISSN 1886-3655versión impresa ISSN 1885-642X
Pharmacy Pract (Granada) vol.4 no.2 Redondela abr./jun. 2006
|
Original research |
Diabetes in a primary care center among Spaniards and immigrants
Diabetes en un centro de salud entre españoles e inmigrantes
Diabetis en un centre de salut entre espanyols i immigrants
Montserrat ROCA VILALTA, Águeda CASTAÑO PÉREZ, Charo LÓPEZ MOYA, Mercedes LÓPEZ OLIVARES.
|
ABSTRACT Diabetes is a disease with different prevalence in different populations. Key words: Diabetes. Emigration and Immigration. Spain. |
RESUMEN Objetivo: averiguar la práctica clínica real del tratamiento
en las unidades de cuidados intensivos sobre las infecciones relacionadas
con catéteres con teicoplanina o vancomicina desde la perspectiva
de un hospital. Como los ensayos clínicos han demostrado que la
eficacia de estos glucopéptidos es simular, también se realizó
un análisis de minimización de costes. Palabras clave: Diabetes. Emigración e inmigración. España. |
Montserrat ROCA VILALTA. Nurse. South Tarrasa Primary Care Center. Tarrasa,
Barcelona (Spain).
Águeda CASTAÑO PÉREZ. Nurse. South Tarrasa Primary Care
Center. Tarrasa, Barcelona (Spain).
Charo LÓPEZ MOYA. Nurse. South Tarrasa Primary Care Center. Tarrasa,
Barcelona (Spain).
Mercedes LÓPEZ OLIVARES. Nurse. South Tarrasa Primary Care Center. Tarrasa,
Barcelona (Spain).
INTRODUCTION
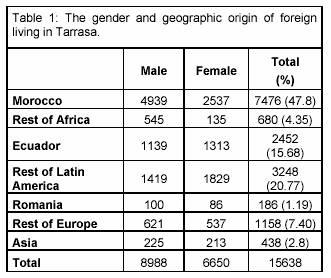
In recent years, Europe has received the most important wave of immigrants in the last few centuries. Spain, which was a country of emigrants a few years ago, has become a receiving country. The immigrants who come to find an opportunity to improve their life status chose mainly Catalonia (23%), Madrid (22%), and Andalusia (13%).1,2 The present study was carried out in Tarrasa, close to Barcelona (20 km), a city with a population of almost 200,000 inhabitants that includes 8.26% of foreign inhabitants. Morocco was the main geographical origin (47.8%), followed by Latin America (36.45%; 43% of these were from Ecuador). The Moroccans were mainly males, in contrast to the Latin Americans, who were mainly females (table 1). Moroccan immigrants were young, with only 1.3% older than 65 years, and 78.3% between 16 years and 64 years old.
Many patients find it difficult to understand the concept of a chronic disease that cannot be cured and that requires them to adapt to a new situation, including follow-up and continuous medication, because they associate the disease with some symptoms that prevent them from acting normally. As a consequence, it is difficult to gain compliance with dietetic requirements. This difficulty can be made worse by cultural differences, and may interfere with the treatment of diseases such as diabetes. These differences range from food habits to the perception of the disease, and make it difficult to persuade patients to comply with dietetic and pharmacologic prescriptions, and thus influence their disease control. For example, Moroccans use to consider diabetes to be an occidental disease that would disappear as soon as they returned to Morocco.3,4 This, combined with the fact that the prevalence of diabetes in Morocco is just 1.52%, makes it even more difficult to gain compliance.5,6
The aim of the present study is to determine if the prevalence of diabetes mellitus was similar among patients visiting our primary care center, regardless of their geographic origin, and to determine if the control of diabetes was different among groups of different geographic origin.
METHODS
The present study was carried out during 2004 in the primary care center at South Tarrasa, which is an appointed center owned by Mutua de Tarrasa. This health care center assists 21,472 inhabitants, with a high proportion of immigrants.
To carry out the study, we reviewed the clinical records of diabetic patients, recording age, gender, geographic origin, type of diabetes, the most recent Hb1AC value, and treatment. The level of diabetes control was categorized following the criteria given by the Servei Català de la Salut (Catalonian Health Service), being: normal a Hb1AC between 4% and 6%; good control, fewer than 7.5%; and poor control, over 7.5%. For immigrant patients, we recorded the year they arrived in Spain.
To analyze gestational diabetes, we surveyed all pregnant women cared for in our center during 2004.
Data were analyzed with computer program SPSS version 11.5.
RESULTS
The total population of diabetic patients in the primary care center was 1215 people, with an average age of 65 years (SD 14). Ages ranged from 7 years to 99 years.
The distribution by gender was quite normal, 598 males (49%) and 617 females (51%). The average ages were 68 years for women and 64 years for men.
Glycosylated hemoglobin Hb1AC concentrations ranged from 4% to 12.4%, with an average of 6.9%. We found normal figures in 32% (n = 389), good control in 34.1% (n = 414) and poor control in 28.7% (n = 349). Regarding the type of diabetes, we found that type 1 diabetic patients had poorer control, with Hb1AC = 8%, than type 2 diabetic patients with Hb1AC = 6.9%.
All type 1 diabetic patients were treated with insulin. For type 2 diabetic patients, 46.6% (n = 532) were treated with OHA, 36.5% (n = 416) with dietetic restriction only, 7.9% (n = 90) with OHA + insulin, and 9% (n = 103) with insulin.
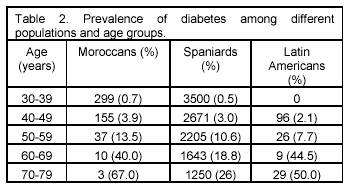
Non-Spanish patients were between 32 years and 76 years old. The prevalence of diabetes for each age group is given in table 2.
Diabetes by geographic origin
The Moroccan patients were the youngest diabetic patients (average age 50 years old), followed by Latin Americans (56 years), Spaniards (66 years), and finally the rest of Europe (68 years).
Among Spaniards and other Europeans there is no difference between genders (51% females in Spaniards and 50% in other Europeans). On the other hand, 70% of Latin Americans and 46% of Moroccans are women. This is why most of the Morrocan immigrants were males, while Latin American patients were mainly females.
The best metabolic control is in the Latin American population, with Hb1AC of 6.3%, followed by Spaniards with Hb1AC of 6.9%, other Europeans with Hb1AC of 7.6%, and finally Moroccans with Hb1AC of 8.1% (table 3).
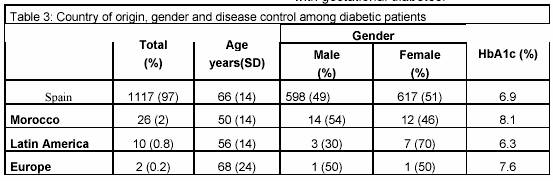
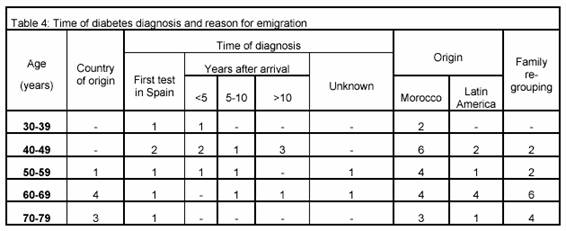
Table 4 presents the distribution of diabetic patients with regard to the time of their diagnosis, and the percentage who came to Spain for family re-grouping.
Diabetes in Moroccans
The average age in type 1 diabetic Moroccan patients was 33 years, while the average age of the rest of the type 1 diabetic patients was 37 years. Among the type 2 diabetics, on average, Moroccans were 55 years old while the rest were 67 years old.
The Hb1AC average in type 1 diabetic Moroccan patients was 10.2%, while the rest of the type 1 diabetics had an Hb1AC average of 8%. In Moroccan type 2 diabetic patients, was 7.8%, while the Hb1AC average for the rest of the type 2 diabetic patients was 6.9%.
Of the type 2 diabetic Moroccan patients, 50% were being treated with OHA. Among the rest of the type 2 diabetic patients, half were treated only with dietetic restrictions and the other half were treated with insulin. Among the rest of the type 2 diabetic patients, 46.6% were treated with OHA, 36.5% with dietetic restrictions, 9% with insulin, and 7.9% with OHA + insulin.
A total of 372 pregnant women with an average age of 30 years were cared for in the primary care center during 2004 and of these, 24 (6.5%) presented with gestational diabetes: 11% of Moroccan pregnant women, 6% of Spanish and 4.2% of Latin American pregnant women presented with gestational diabetes.
DISCUSSION
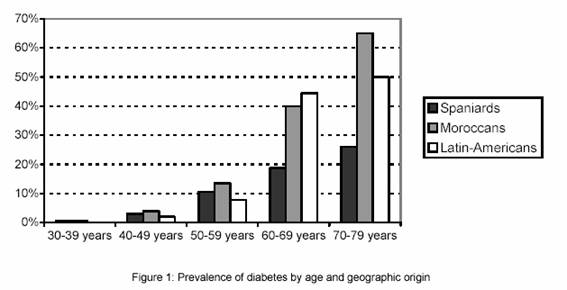
We have demonstrated that the initial hypothesis in this study, a greater prevalence of diabetes in Morrocan patients than in Spanish patients, was correct, as seen in figure 1. Previous studies7 found that prevalence of diabetes in the country of origin is much lower than that in the receiving country.
Probably, one of the reasons for this difference is a change in food habits. In Spain they consume more sweet drinks, more pastry, pre-cooked meals, etc. Among Morrocans, the first immigrant is usually a man, without his family. It is possible that many of them cannot prepare their own meals, and will have an unbalanced intake, including fast food. This could help to explain their poorer metabolic control.
Another reason for the greater prevalence in the receiving country may be that because on re-aggregating families, a sick family member may take precedence over healthy members. This could explain the enormous prevalence of diabetes in immigrants over 60 years old, who are the parents of those who came to Spain to work. This is confirmed because most of these patients came with a previous diagnosis of diabetes, as seen in table 4.
As there is a higher prevalence of diabetes in Moroccans, and their metabolic control is poorer, we consider them to be a group in need of specific education.
CONCLUSIONS
The prevalence of Moroccan diabetic patients in our primary care center is higher than that in Spaniards in all age groups and for all types of diabetes (type 1, type 2 and gestational). The prevalence among Latin-American patients is lower, except in those older than 60 years.
Most of our patients present good diabetes control, but that of our Moroccan patients is poor.
|
References |
1- Manual de Atención Sanitaria a Inmigrantes. Conserjería de Salud. Junta de Andalucía. 2º Edición. 2004. [ Links ]
2- Instituto Nacional de Estadística. España en cifras 2003-2004. Padrón. URL: http://www.ine.es/es [ Links ]
3- Estudio de los magrebíes con diabetes inmigrados a la ciudad de Barcelona. Díaz Casas M. URL: http://www.fsf.es/cast/recerca/investigación01 [ Links ]
4- Inmigración y diabetes. URL: http://www.diabetes.bayer.es [ Links ]
5- OMS. Diabetes Programme: Country and Regional data. URL: http://www.who.int/diabetes/facts/world_figures/en/ [ Links ]
6- Ruiz Ramos M, Roche F, Gálvez P, Fernández D, Viciana F, Hernández JA, Canto V. Diferencias por género en el estado de salud de una población de la Wilaya de Tetuán (Marruecos). Gaceta Sanit 2002;16(supl 1):72. [ Links ]
7- Diabetes tipo 2 e inmigración. Pertiñez Mena J, Franch Nadal J. Scientific Communication Management, SL. 2005 [ Links ]

