










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Although patient satisfaction has been evaluated and studied for some time, it was not linked to quality measures until the 2000s. In 2001, patient-centered care was considered when assessing the quality of the patient's experience with health care services.1According to the Agency for Healthcare Research and Quality, “patient experience includes several aspects of health care delivery that patients value highly when they seek and receive care, such as getting timely appointments, easy access to information, and good communication with health care providers”.2 Patient satisfaction and patient experience differ in that satisfaction measures a patient's expectations, whereas experience measures whether or not care processes that were supposed to happen occurred.2,3 Considering these definitions, this means that patient experience is more objective (i.e., did something happen or not) than patient satisfaction which can be subjective and vary according to patient expectations for a particular service.2,3 In prior pharmacy literature, most patient satisfaction studies examined elements of patient experience, although this was not differentiated from satisfaction.4 5 6 7 8-9 This is not surprising since the terms satisfaction and experience are commonly interchanged.2,3 For descriptive studies, satisfaction with pharmacist care tends to be high with ratings near the high end of a scale across care settings, including inpatient and community pharmacist services as well as pharmacist services delivered via the telephone.5,6,10,11 A systematic review of pharmacist services included 41 studies that measured patient satisfaction and found that satisfaction with care was higher when pharmacists were involved compared to when they were not in half of the studies.4
Clinical pharmacists in ambulatory care settings specialize in chronic disease management and when collaborative practice agreements are in place, clinical pharmacists' roles typically allow for initiating new prescriptions, changing or discontinuing medications, and providing comprehensive medication reviews. Studies have shown positive clinical outcomes for chronic diseases when ambulatory care pharmacist-led management is involved.4,6,11 Less has been reported about patient experience with clinical pharmacist services in an ambulatory care setting. However, there have been reports of satisfaction with pharmacist management of specific conditions such as hepatitis C virus (HCV) treatment and rheumatoid conditions.7,9 In a US urban academic medical center hepatology outpatient clinic, 24 participants indicated the highest possible level of overall satisfaction (i.e., great) and similar ratings occurred for questions related to pharmacist education about the HCV infection, medication administration and storage, and medication adherence.7 In an outpatient rheumatology clinic in Canada, overall scores across six care dimensions were significantly higher with a pharmacist-physician team vs. physician alone (4.6, SD=0.4 vs. 4.3, SD=0.4 on a 5-point scale).9
Despite the fact that pharmacists have a track record of being a member of care teams at federally-qualified health centers (FQHCs), little is known about patients' perceptions of clinical pharmacist care in this setting.12 13 14-15 Patients served by a FQHC tend to be complex, often have multiple uncontrolled chronic conditions and are uninsured or underinsured, which means that tailoring care experiences is important for achieving optimal outcomes. At CommUnityCare Health Centers, which are FQHCs in Central Texas, clinical pharmacist appointment-based visits are focused on ensuring medication regimens are individualized to meet the patient's needs. In addition to medication reviews, patients receive medication and adherence counseling, as well as disease state education. Collaborative practice agreements guide medication management for the following conditions: diabetes, hypertension, hyperlipidemia, anticoagulation, heart failure, chronic obstructive asthma, pulmonary disease, primary hypothyroidism, gout, obesity, smoking cessation, depression, osteoporosis, and rheumatoid arthritis. CommUnityCare administrators were interested in assessing patient experience with clinical pharmacists to assess quality of care and identify opportunities to improve clinical pharmacist services as part of ongoing quality improvement monitoring. This study adds to the literature by assessing 4 components of patient experience (pharmacist-patient interactions, information provision, support for self-care, and involvement in decisions) with clinical pharmacist care in an ambulatory care setting in a diverse patient group. The study's objectives were to describe patient experience with clinical pharmacist services in a FQHC setting and to determine if demographic or health-related factors were related to patient experience.
METHODS
Study design and sample
A cross-sectional design was used to address the study objectives. The study sites included ten FQHCs in Travis County, Texas. FQHCs are funded by the United States Health Resources and Services Administration Health Center Program and provide health care for medically underserved areas using a sliding scale fee based on income levels.16 Patients were included if they were >18 years old, completed a clinical pharmacist appointment in March or April 2018, and were English or Spanish speaking. To avoid confounding of the results, patients were excluded if they were seen during a co-visit, which included both the clinical pharmacist and physician.
Survey instrument
The primary outcome was patient experience and survey questions were developed utilizing previously validated surveys and adapted to align with the clinical pharmacist services provided at CommUnityCare Health Centers.3,17 18-19 The Oxford Patient Involvement and Experience Scale was used as a guide for determining relevant patient experience domains, which included pharmacist-patient interactions (3 questions), information provision (5 questions), support for self-care (1 question) and involvement in decisions (1 question).18 These 10 items were measured using a 5-point Likert scale ranging from 1 =strongly disagree to 5 =strongly agree. Domain mean scores and an overall mean score comprised of all 10 items were calculated. One additional item, measured on a 5-point scale anchored by 1=very poor to 5=excellent, was used to rate the overall patient experience. In addition to patient experience, demographic (age, gender and race) and health-related variables were measured (number of clinical pharmacist visits in last six months, self-reported health status, and type of health conditions). Prior to survey administration, survey items were assessed for content validity by clinical pharmacists at each site. Pharmacist researchers with expertise in pharmacist services and survey design also assessed face and content validity of the survey. The survey was translated to Spanish by trained translators, back translated to English and re-reviewed for consistency. See Appendix A for the survey instrument.
Data collection and analysis
Upon completion of the clinical pharmacist visit, eligible patients were asked if they were interested in completing an anonymous patient experience survey. If they agreed, patients were handed a cover letter and survey in their preferred language (Spanish or English). Clinical pharmacists read out loud a script which described the survey purpose (i.e., to get feedback about and improve pharmacist services), directions, and privacy procedures. The patients then completed surveys in a designated area in the clinic, but away from their clinical pharmacist, and surveys were inserted into a sealed box. Data were collected from March to April 2018. Descriptive (means, standard deviations, frequencies, and percentages) and inferential statistics (analysis of variance (ANOVA)) were used to address the study objectives. Cronbach's alpha was utilized to measure scale reliability. The study was approved by the University of Texas at Austin Institutional Review Board.
RESULTS
From the convenience sample, a total of 99 patients completed the surveys. About half of the participants were women (53.1%), and the majority were Hispanic (63.3%). The mean age was 55.4 (SD=12.1) years. One-third of participants had 1 - 2 clinical pharmacist visits in the last 6 months, 42.3% had 3 - 5 clinical pharmacist visits, and 24.7% had 6 or more visits. Thirty-eight percent self-rated their health as fair and 34.0% rated their health as good. Diabetes, hypertension, and hypercholesterolemia were the most common chronic conditions with 77.6%, 57.1%, and 41.8% of participants reporting the presence of these conditions, respectively. Table 1 provides more detail regarding demographic and health-related information.
Table 1. Summary of Demographic and Health-Related Information (N=99a)
| Variables | Mean, SD N (%)b |
|---|---|
| Demographics | |
| Age in years (n =92) | 55.4, SD=12.1 |
| Gender | |
| Women | 52 (53.1) |
| Men | 46 (46.9) |
| Total | 98 (100.0) |
| Race/Ethnicity | |
| Asian | 1 (1.0) |
| Black | 13 (13.3) |
| Hispanic | 62 (63.3) |
| White | 22 (22.5) |
| Total | 98 (100.1) |
| Health-Related Information | |
| Number of clinical pharmacist visits | |
| 1-2 visits | 32 (33.0) |
| 3-5 visits | 41 (42.3) |
| 6 or more | 24 (24.7) |
| Total | 97 (100.0) |
| Self-rated health | |
| 1 =Poor | 2 (2.1) |
| 2 =Fair | 37 (38.1) |
| 3 =Good | 33 (34.0) |
| 4 =Very Good | 16 (16.5) |
| 5 =Excellent | 9 (9.3) |
| Total | 97 (100.0) |
| Presence of chronic diseasesb | |
| Diabetes mellitus | 76 (77.6) |
| Depression | 11 (11.2) |
| Hypertension | 56 (57.1) |
| Hypercholesterolemia | 41 (41.8) |
| Hypothyroidism | 7 (7.1) |
| Otherc | 16 (16.3) |
aNot all respondents answered each question
bMay not total to 100.0 due to rounding or if multiple responses were allowed
cOther reported health conditions where N≤3: Atrial fibrillation, arthritis, asthma, coronary artery disease, congestive heart failure, cancer, end stage renal disease, Factor 5 Leiden thrombophilia, human immunodeficiency virus, herniated disc, obstructive sleep apnea, venous thromboembolism
SD =standard deviation
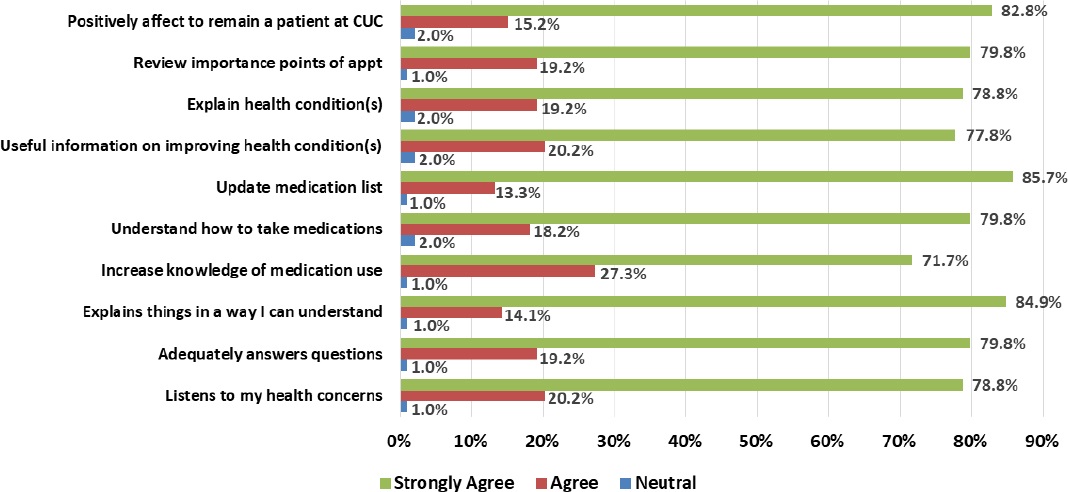
The overall 10-item scale score was 4.8, SD=0.4 (1 =strongly disagree to 5 =strongly agree) and the 1-item overall rating score was 4.9, SD=0.3 (1 =very poor to 5 =excellent). The 4 domains (pharmacist-patient interactions, information provision, support for self-care, and involvement in decisions) each had a mean score of 4.8, SD=0.4. These results show that patients were highly satisfied with their patient experience related to the clinical pharmacist visit. Reliability for the 10-item scale resulted in a Cronbach's alpha score of 0.96, which is deemed excellent. Table 2 summarizes the mean for each item and provides summary data and Figure 1 shows frequencies of responses for each item. None of the respondents selected “strongly disagree” or “disagree” for any of the items and the majority of responses were either “agree” or “strongly agree”.
Table 2. Means of Patient Experience Scale Items (N=99)
| Items | Mean, SD |
|---|---|
| Pharmacist-patient interactionsa | |
| My clinical pharmacist listens to my health concerns. | 4.8, SD=0.4 |
| My clinical pharmacist adequately answers my questions. | 4.8, SD=0.4 |
| My clinical pharmacist explains things in a way that I am able to understand. | 4.8, SD=0.4 |
| Domain Mean | 4.8, SD=0.4 |
| Information provisiona | |
| Appointments with my clinical pharmacist have increased my understanding of what my medications are used for. | 4.7, SD=0.5 |
| My clinical pharmacist is able to help me understand how to take my medications. | 4.8, SD=0.5 |
| My clinical pharmacist makes sure my medication list is up-to-date. | 4.8, SD=0.4 |
| My clinical pharmacist provides useful information on helping me improve my health condition(s). | 4.8, SD=0.4 |
| My clinical pharmacist is able to provide explanations of my health condition(s) in a way that I am able to understand. | 4.8, SD=0.5 |
| Domain Mean | 4.8, SD=0.4 |
| Support for self-carea | |
| At the end of my appointment my clinical pharmacist reviews what we talked about and tells me what is important. | 4.8, SD=0.4 |
| Involvement in decisionsa | |
| My clinical pharmacy appointments have positively affected my decision to remain a patient at CommUnityCare. | 4.8, SD=0.4 |
| Overall Total Scale | 4.8, SD=0.4 |
| Cronbach's Alpha | 0.96 |
| Overall rating of clinical pharmacist servicesb | 4.9, SD=0.3 |
a1=strongly disagree, 2=disagree, 3 =neutral, 4 =agree, 5=strongly agree
b1=very poor, 2=poor, 3 =good, 4 =very good, 5=excellent
SD =standard deviation
When examining the relationship between patient experience and demographic and health-related variables, ANOVA showed a significant difference in patient experience (mean, SD) and race/ethnicity (F=3.17, p=0.0466). Duncan's post-hoc test revealed that African Americans (5.0, SD=0.1) had significantly higher patient experience scores compared to Hispanics (4.7, SD=0.4); while there was no difference between whites (4.9, SD=0.3) and Hispanics nor whites and African Americans. No other demographic or health-related factors were significantly different.
DISCUSSION
Patients receiving care in a FQHC highly rated their experience with the clinical pharmacist visit, with high individual domain and overall scores. The lack of significant findings for the relationship between patient experience and most demographic and health-related factors indicates that clinical pharmacists consistently provided a positive care experience, regardless of demographic or health-related characteristics. Although, African Americans had a significantly higher overall patient experience score when compared to Hispanics (5.0, SD=0.1 vs. 4.7, SD=0.1). The reason for this is not known but it may be due to language or cultural barriers that are not fully addressed in the clinical pharmacist visit. A previous study at CommUnityCare found that Spanish-speaking patients (n=101) reported a relatively high mean score of 3.6, SD=0.5 out of 4 points for their satisfaction with pharmacist communication and 3.6, SD=0.5 out of 4 points for their demonstration of cultural sensitivity.17 Spanish-speaking clinical pharmacists are available at CommUnityCare, but it is possible that not all patients in the current study had access to one at their visit and had to use an interpreter instead, which may have impacted their experience. The Spanish speaking ability of clinical pharmacists was not collected on this survey, and is therefore unknown.
This study is one of the first to collect information on patient experience with clinical pharmacist services in a FQHC. Additionally, the participants were comprised primarily (63%) of Hispanic patients, which provides unique insight into this group. Patients in other studies in outpatient settings such as HCV, rheumatology, and Medicare annual wellness visit clinics also highly rated elements of patient experience and overall satisfaction with pharmacist services.7 8-9 This study focused on patients that can be complex to manage and often require tailoring services to help patients meet treatment goals. The fact experience scores were so high indicates that clinical pharmacists were addressing important aspects of patient-centered care such as clear communication, provision of information for shared-decision making, and support for self-management of medications.18,20 This is important because patient experience is now being used by health care payers as a quality measure and linked with payment for patient outcomes. While patient experience is commonly measured for physicians in outpatient settings, pharmacists in outpatient settings may not be routinely evaluated. Thus, pharmacists in these settings should be proactive in requesting patient experience surveys at least annually to obtain objective feedback from patients.
At CommUnityCare Health Centers, the standard of care for clinical pharmacist appointments aligns with the domains contributing to patient experience. The pharmacist-patient interaction encompasses listening and answering questions and addressing health concerns adequately for the patient. The information provisions domain primarily relates to the patient's understanding of their medications and disease state. For a condition such as diabetes, clinical pharmacists assess patient knowledge about diabetes and will then provide handouts about diabetes, hypoglycemia, and adherence to medications based upon the level of understanding of the patient. Involvement in decisions and support ensures patients understand the important discussions during the appointment so patients return to follow-up appointments ready to progress forward in the health condition(s). To reinforce key discussion points, appointments are concluded with a patient plan for patients to take home with them. Therefore, it is not a surprise that the results were positive, considering the current clinical pharmacist practice model has been developed to focus on patient experience. The study findings validate that an intentional approach to patient-centered care can result in a quality patient experience. The information provisions domain had a mean rating that was similar to the other domains. However, when examining individual questions, an opportunity to improve patient understanding about what medications are used for was evident given this item had the lowest percentage of “strongly agree” responses (see Figure 1). One strategy to address this is to include the purpose of each medication in the care plan that is given to each patient at the end of the visit.
Limitations
This study had several limitations that require consideration. First, a convenience sample was used, which means that only patients who had visits during the study period were invited to participate. Also, some patients were not able to participate due to transportation issues, inability to read, or having another doctor's appointment after the clinical pharmacist visit. Finally, no information was collected about patients who chose not to participate, so we do not know if they differed from those who participated. All of these issues likely resulted in selection bias. Also, surveys were completed at ten clinics and multiple clinical pharmacists provided care which had the potential to bias findings based upon clinic characteristics or variations in clinical pharmacist delivered care. However, the impact on survey results was considered to be negligible based upon the upper range of responses (mostly 4s and 5s) for each question. One reason for this may be because CommUnityCare clinical pharmacists use the same care process in each clinic and practice using collaborative practice agreements. Generalizability of study findings may also be limited to other FQHCs or safety-net settings that have an embedded pharmacist model.
CONCLUSIONS
Patients indicated that care from clinical pharmacists in a FQHC resulted in a positive patient experience across four domains. An opportunity to improve patient understanding of what medications are used for exists in the information provisions domain. Patient experience should be regularly assessed, at a minimum annually, to ensure patients are having positive care experiences and to identify opportunities for improvement.

