










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkCASE REPORT:
We present the case of a seventy-two-year-old male patient, smoker, who developed a poorly differentiated carcinoma in the oral cavity that was treated with radiotherapy and followed by psychiatry due to depression and suicidal ideation, three years before the current diagnosis.
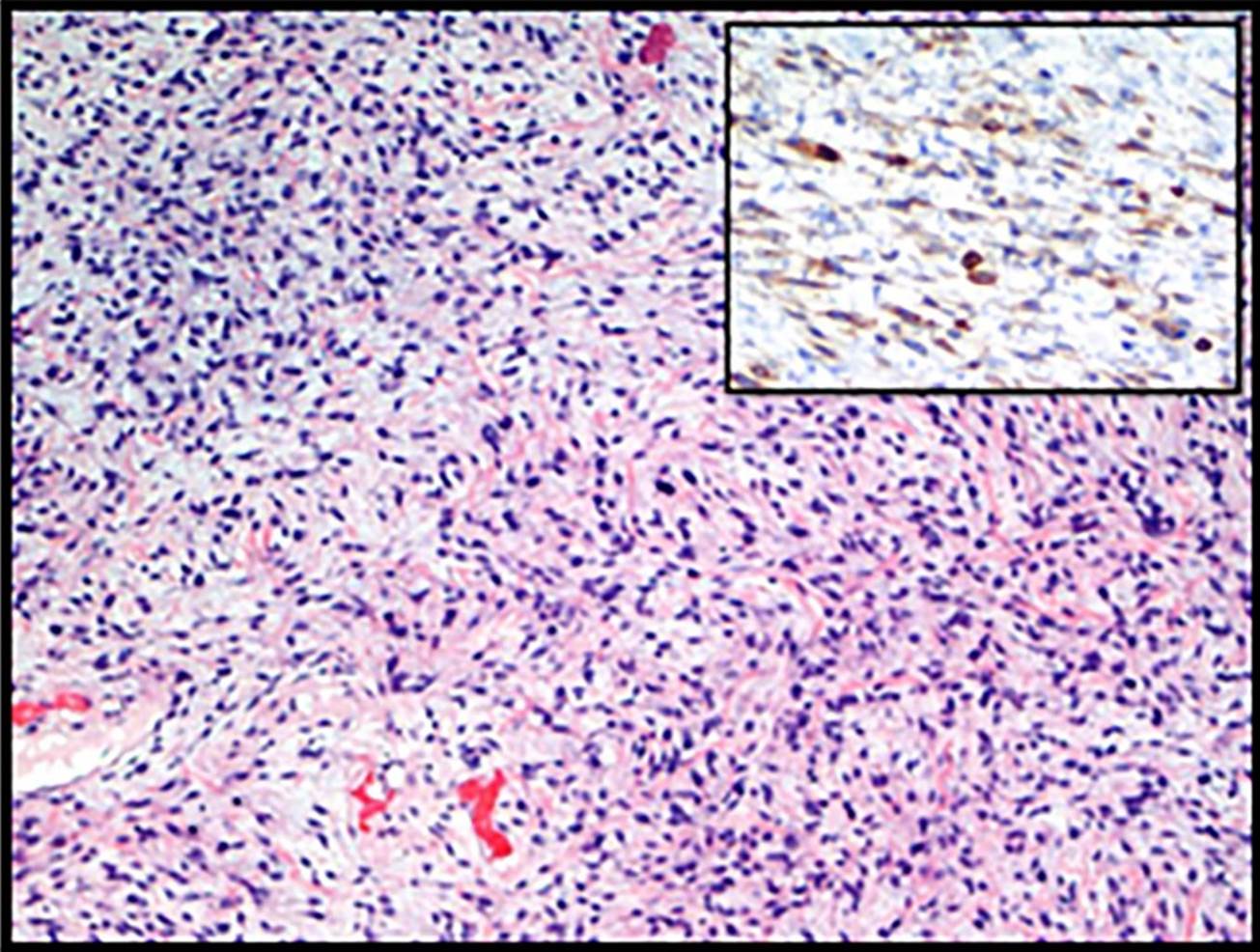
Currently, the patient shows an inguinal mass with two months of evolution, with rapid growth and indolent course. The therapeutic decision is to perform radical orchiectomy, including excision of spermatic cord. We can see in the image an ovoid mass of 12x7x6 cm and 440 g (Figure 1) and histological section with 200x magnification power and hematoxylin and eosin stain (Figure 2).

DIAGNOSIS: SOLITARY FIBROUS TUMOR
The anatomopathological diagnosis was Solitary fibrous tumor (SFT) grade 1 of FNCLCC (Fédération Nationale des centres de Lutte Contre le cáncer). American Joint Committee on Cancer (AJCC) 8 th Edition TNM stage: pT2.
SFT is a mesenchymal neoplasm and it was first reported in 1931 as a tumor of the pleura1. SFTs are uncommon that can appear in all sites of body. It represents 5% of soft tissue tumors and only 2% is extrathoracic. The incidence of paratesticular is low2 with 22 cases are reported in the literature3. Most neoplasm has occurred in male with ranges 42 to 67 years old, without predisposing factors, although some papers have associated it with trauma and IgG4 diseases. Typically, it containing a specific NAB2-STAT6 gene fusion and overexpressing STAT64.
Macroscopically, the lesion shows a fibroelastic consistency and a shiny surface. The cutting surface has whorled pattern and yellowish pearly (Figure 1).
Microscopically, the tumor is composed by heterogeneous areas settled by a population of spindled cells arranged in fascicles or patternless, with an underlying collagen-dense stroma, showing focal hemangiopericytoma-like changes (Figure 2).
Immunohistochemically the tumor shows CD34, CD99 and Bcl-2 immunoreactivity (Figure 2, Bcl-2 upper right), in a diffuse and strong pattern. The lesion is negative for epithelial marker (CKAE1/AE3), lymphoid (CD45) and melanic (HMB-45). The cells do not reactivity for SMA, C-Kit, Inhibin, S-100, PLAP, D2-40, CD31, WT-1 and Calretinin. Proliferation index, labelled by ki67 stain, shows a 5-20% rate.
Regarding the behavior of this neoplasm, it has been reported that 10 to 15% of extrathoracic SFT will recurs or metastasizes, so that strict surveillance is obliged5.
The differential diagnosis will include entities such as leiomyosarcoma, a relatively common mesenchymal tumor in this area, whose origin is smooth muscle. This neoplasm shows a similar histological pattern, but the immunohistochemical profile includes reactivity for smooth muscle actin and negativity for CD99 and Bcl-26. Others differential diagnoses will be neural tumors such as neurofibromas (S-100 positive) and vascular lesions (CD31 or D2-40 positive).
