










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntrodution
During the last few decades, there is a new demographic behavior in the elderly, in which there is a progressive increase in the prevalence of the elderly population due to improvements in life expectancy and the increase in the proportion of elderly in the world's population. However, the search for strategies that seek to prolong the life expectancy free of functional and cognitive impairment is relevant. The elderly population is a group characterized by heterogeneity, so that we can find in the same age group, elderly with preserved functional capacity and the ones with memory impairment levels in an advanced state.1
The aging is a continuous process in which there is a progressive decline in physiological processes. Among the most apparent physiological changes during aging, there is a decrease in height by about 1cm per decade and structural and functional changes in the nervous system, due to reduction in the number of neurons. It is also usual to have increased arterial stiffness, increased blood pressure, a decreased cardiac output at rest and during exercise, and reduced bone mineral density.2-4
Specifically, regarding the changes that affect the central nervous system with the course of the aging process, there is the ventriculomegaly and reduced cortical mantle, usually accompanied by progressive cognitive impairment. However, regardless of degenerative diseases, cognitive dysfunction and dementia were observed. Dementia is the progressive reduction or loss of cognitive abilities, partial or complete, permanent or momentary form, enough to cause a loss of autonomy and functional decline.2
For Pedrosa and Holland,5 loss of independence and low levels of cardiorespiratory fitness are associated with risk of morbidity and mortality from chronic diseases, on the other hand the performance of daily activities of life and the maintenance of independence are linked to improved general health. In this sense, low levels of muscular strength and obesity are associated with functional decline and cognitive impairment.3,6 In addition, important measures related to functional capacity and maintenance of daily activities as the amount of motor units, the contraction speed, neurons driving speed, the reaction time, and volume of brain matter show worsening over the decrease in walk velocity.1,4,7
Accordingly, it appears that functional capacity, maintaining the autonomy are associated with a lower incidence of chronic degenerative diseases. Thus, there is a constant need for assessments and maintaining physical fitness, since it features associated with general health in the elderly, particularly in relation to cardiovascular disease, cognitive response and hospitalization.2 In this light, the aim of this study was to evaluate the cognitive profile of the elderly and its association with anthropometric and functional aspects.
Methods
Subjects
The sample consisted of 84 elderly of both sexes (15 male and 69 female) aged between 61 and 90 years living in the Federal District, selected by convenience. The inclusion criteria were: have over 60 years of age, a resident in own home, sign the informed consent term, participate in all data collections, show no neuropathy or musculoskeletal problem that precludes participation in physical tests.
Before data collection, the Ethics Committee on Research of the Hospital of the Forces Army (HFA) under protocol 016/2011/CEP/HFA approved this study. Volunteers or their guardians signed a free and informed consent form (ICF).
Experimental design
After contact with the elderly in their homes, we collected data related to anthropometric measurements, the Mini Mental State Examination (MMSE), and functional testing. The adapted Functional Fitness Test was used in this study.8-12
Romberg test: The researcher asked each volunteer to stay with his/her feet together, barefoot, with open eyes for about 30 s and then with eyes closed for 30 s. The standing position without loss of balance clocked the permanence time and the test was considered positive when the volunteer has failed to spend more than 10s with their eyes closed without body oscillations. It the time each volunteer had to have the first oscillation, considered equilibration time, was recorded similar to the procedure adopted by Cho et al.8
Handgrip test: After familiarization, the participants were seated, with the shoulder in neutral position, elbows bent at 90° and wrist in a neutral position. The subjects were instructed to perform a maximal isometric contraction to verbal command of the examiner. Three attempts were made by alternating members, with 60s interval. No encouragement was given by the researcher during the test. The procedure was carried out respecting the criteria described by Shiratori et al.9
Stand up and walk test (TSW) (Timed up and go - TUG): This test was measured using a stopwatch and recorded in seconds the time it takes to stand up from a chair, walk a distance of 3 m, turn around an obstacle and sit again. We used a chair 45 cm in height for the seat and 65 cm in height to the armrest with backrest, brand Grosfillex®. The TSW was done according to the procedure described by Hyun et al.10
Chair get up test: For this test, we used a chair with traditional back, without lateral support, with 45 cm height, and a stopwatch. The chair was supported on the wall to prevent the same from moving during the test period. A pre-test for familiarization was conducted to ensure that the participant sitting occupies most of the seat with his/her feet flat on the floor. He was spoken aloud each time the participant until the fifth time. This test was performed according to procedure described by Yamauchi et al.11
Mini Mental State Examination (MMSE): The MMSE consists of typical questions grouped into 7 categories, each of them designed in order to assess specific cognitive functions, with they being: time orientation, local, words registration, attention and calculation, memory, language, and visual constructive capacity. Leading questions and punctuation establishment based on pre-established scores on the instrument obtained responses. The cutoff points used in this study were adopted as model, as used previously in another study by Ferreira et al.12
Body mass and height: For the body mass a digital Britania® balance with a resolution of 0.1 kg was used. For this measurement, individuals were with minimum clothing, positioned to his feet, and remained motionless until the stabilization of the value displayed on device. A tape fixed to the wall was used for the height measurement. The head was positioned according to the Frankfurt plan in which an imaginary line was passing through the lowest point of the inferior orbital rim and the highest point of the upper edge of the right auditory meatus.13 After these adjustments, the most prominent point of the head to the realization of the measure was noted.
Waist and hip circumference: The measurement of waist circumference (WC) was carried out with a tape, 150 cm in length and resolution of 0.1 cm. It was measured in line with the navel, and evaluated without shirt. The measurement of the hip circumference (WHR) was held at the leading region of the hip, assessed with feet together and legs straight.14
Arm circumference: To measure the circumference of the arm, the same was flexed toward the chest at a 90° angle, and located and marked the midpoint between the acromion and olecranon. It was requested to the individual to stay with the arm extended along the body and with the palm facing down.15
Thigh circumference: The tape was placed across, half way between the inguinal line and the upper border of the patella. Feet were slightly apart and body weight distributed equally between them.14
Neck circumference: The measurement was performed with the participant standing with the back straight and head in the Frankfurt horizontal plane. The tape was positioned in the lower neck circumference just above the laryngeal prominence (Adam's apple).
Statistical analysis
Initially the data normality was checked, using the Shapiro-Wilk test when the group was stratified to 50 individuals and Kolmogorov-Smirnov when the group was more than 50 individuals. Descriptive statistics and frequency of measures were used to assess the prevalence of hypertension, diabetes, labyrinthitis, osteoporosis, physical activity and nutritional evaluation between different groups. We used the chi-square test to analyze the frequency ratios between the different groups. The test “t” independent was applied to analyze the anthropometric, hemodynamic differences, mental state and performance of functional tests in accordance with the level of physical activity, nutritional classification and sex.
To analyze the cutoff points of anthropometric indicators and performance of the studied functional tests that could identify dementia the ROC curve technique (receiver operating characteristic) was adopted. The bivariate regression models and multivariate logistic regression were used to calculate the Odds Ratio (OR), so that all the functional capacity and anthropometric variables were tested as controls in the regression models. p value < 0.05 was adopted to point out the significant differences. Statistical analysis was performed using SPSS 18.0 (SPSS Inc., Chicago, Illinois, USA) for Windows, and the Stata software version 9.1 (College Station, TX: StataCorp LP).
Results
Tables 1 and 2 presented the characteristics of the sample, with anthropometric data, hemodynamics performance and results of the MMSE test as well as the percentages of dementia and other chronic diseases.
Table 1 Characterization sample with anthropometric data and hemodynamic performance.
| Men n = 15 | Women n = 69 | Total sample n = 84 | |
|---|---|---|---|
| Body mass (kg) | 76.2 ± 10.0 | 68.9 ± 12.0* | 68.3 ± 13.3 |
| Height (m) | 1.6 ± 0.1 | 1.6 ± 0.1* | 15.5 ± 0.1 |
| Body mass index (kg/m2) | 28.5 ± 2.7 | 27.4 ± 4.4 | 27.6 ± 4.2 |
| Conicity index | 1.4 ± 0.1 | 1.4 ± 0.1 | 1.4 ± 0.1 |
| Waist hip ratio (cm) | 1.0 ± 0.1 | 0.9 ± 0.1* | 1.0 ± 0.1 |
| Waist height ratio (cm) | 0.64 ± 0.1 | 0.6. ± 0.1 | 0.6 ± 0.1 |
| Systolic blood pressure (mmHg) | 136 ± 13 | 131 ± 13 | 132 ± 13 |
| Diastolic blood pressure (mmHg) | 92 ± 13 | 85 ± 10 | 86 ± 11 |
| Mean arterial pressure (mmHg) | 106 ± 12 | 100 ± 10 | 101 ± 11 |
| Neck circumference (cm) | 43.0 ± 2.9 | 38.9 ± 4.0* | 39.1 ± 3.9 |
| Arm circumference (cm) | 31.4 ± 2.3 | 32.0 ± 4.2 | 32.0 ± 4.3 |
| Thigh circumference (cm) | 49.1 ± 4 | 49.0 ± 6.1 | 48.5 ± 5.6 |
| Hip circumference (cm) | 103.0 ± 6.8 | 103.0 ± 11.1 | 104.0 ± 9.7 |
| Waist circumference (cm) | 104.0 ± 9.3 | 97.0 ± 9.8* | 98.0 ± 10.6 |
| Dominance handgrip (kg) | 17.0 ± 8.0 | 20.4 ± 8.3 | 19.9 ± 8.3 |
| Non-dominance handgrip (kg) | 15.5 ± 8.5 | 18.7 ± 9.9 | 18.2 ± 9.7 |
| Test stand and walk (s) | 10.2 ± 3.3 | 11.3 ± 4.1 | 11.1 ± 4.0 |
| Chair get up (s) | 11.2 ± 6.0 | 12.1 ± 9.4 | 11.9 ± 3.5 |
| Mini-Mental State Examination (score) | 21.4 ± 3.8 | 21.9 ± 4.0 | 21.8 ± 4.0 |
*Significant difference between men versus women.
Table 2 Characterization of dementia data frequency and chronic diseases.
| Men | Women | Total sample | |
|---|---|---|---|
| Obesity | 77% | 56.5%* | 572% |
| Hypertension | 92.3% | 73.2%* | 76.2% |
| Diabetes Mellitus | 38.5% | 31% | 32.1% |
| Labyrinthitis | 23% | 32.4% | 31% |
| Osteoporosis | 15.4% | 26.8% | 25% |
| Dementia | 7.7% | 7% | 7.1% |
*Significant difference between men versus women.
There was a statistically significant difference for the variables: body weight, height, WHR, neck circumference and WC, in which men showed higher values when compared to women.
Table 3 shows the cutoffs and their sensitivity and specificity of anthropometric indicators and tests that measured the functional capacity in predicting dementia.
Table 3 Cutoffs, sensitivity and specificity of anthropometric measures and functional tests as predictors of dementia.
| Dementia (n = 84) | Cutoffs | Sensitivity | Specificity | Area under curve |
|---|---|---|---|---|
| Waist (cm) | 100 | 83.3 | 65.4 | 0.75 (0.57-0.93) |
| Body mass index (kg/m2) | 28 | 67 | 53 | 0.71 (0.47-0.94) |
| Conicity index | 1.41 | 50 | 62 | 0.57 (0.36-0.78) |
| Waist hip ratio (cm) | 0.92 | 50 | 52 | 0.46 (0.25-0.67) |
| Waist height ratio (cm) | 0.67 | 67 | 77 | 0.77 (0.61-0.93) |
| Dominance handgrip (kg) | 24 | 67 | 39 | 0.38 (0.16-0.59) |
| Non-dominance handgrip (kg) | 28 | 67 | 32 | 0.33 (0.11-0.54) |
| Test stand and walk (s) | 10.6 | 66 | 51 | 0.61 (0.3-0.92) |
According to Table 3, the WC and the waist/height ratio (WHeR) were considered predictors of dementia, since the lower limit of the confidence interval was above 0.50 (Li-IC > 0.5). Already body mass index (BMI), taper index, waist/hip ratio (WHR) and performance tests, as carried out in our methodology, showed no reliable values of sensitivity and specificity (Li-CI < 0.5). Fig. 1 shows the ROC curves of the key variables tested.
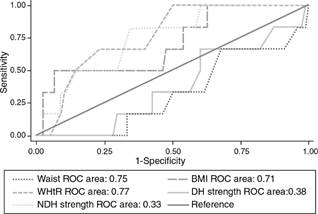
Fig. 1 ROC curves for the anthropometric indicators and functional tests as predictors of dementia. Abbreviations: BMI, body mass index; DH strength, dominant hand palmar pinch strength; NDH strength, nondominant hand palmar pinch strength; ROC, receiver operating characteristic; WHtR, waist-to-height ratio.
Table 4 presented the odds ratio of anthropometric measures and functional performance for dementia for the total sample.
Table 4 Odds Ratio for dementia for the total sample.
| Measures | Total sample |
|---|---|
| Body mass index (kg/m2) > 27kgm2 | 3.75 (0.5-30) |
| Conicity index > 1.25 | 1 |
| Waist > 100cm | 8.15 (0.99-66) |
| Waist height ratio (cm) > 0.67 | 5.63 (1.11-28)* |
| Sedentary lifestyle | 1.36 (0.26-7.0) |
| Dominance handgrip (kg) > 20 | 0.53 (0.10-2.7) |
| Non-dominance handgrip (kg) > 20 | 0.36 (0.05-2.9) |
| Test stand and walk (s) > 10.59 | 0.5 (0.05-2.6) |
| Balance | 0.15 (0.04-0.65) * |
| Chair get up (s) | 0.65 (0.12-3.2) |
*Significant odds ratio.
Initially the sex was tested as modifier effect; however, it showed no change in capacity, and we chose to analyze only the total sample without stratification by sex. Among the anthropometric and functional variables analyzed, only WHeR and the equilibrium showed risk/protection, respectively as significant. Seniors with above 0.67cm WHeR were 5.63 times more at risk of presenting dementia while older people who have balance were 15% less likely to have dementia.
Discussion
The main results of this study showed that the prevalence of dementia verified by the results of the MMSE in the elderly was 7%, and that among the anthropometric and functional variables tested, only WC and WHeR showed predictive capacity to dementia. When analyzed the odds ratio, it was found that the maker of the top WHeR to 0.67 cm is 5.6 times more likely to have dementia, while the balance of the presence means protection factor by 15%. It is important to understand that the MMSE results only suggest the presence of dementia, and despite having high correlation with the same, more specific tests are necessary for the diagnosis to be confirmed.
We believe that the highest amount of abdominal fat was verified by WC and WHeR. According to Matsudo et al.,16 the anthropometric measures (greater deposition of fat in the central region) are associated with lower levels of physical fitness and a less active lifestyle. The gain in body weight as well as body fat accumulation particularly in the central region appears to result from a standard genetically programmed, changes in diet and physical activity level, age-related or an interaction between these factors. Lower levels of muscle strength, as well as obesity (BMI ≥ 30), higher waist circumference and percentages of fat are associated with functional declinel.3
The grip strength is the only muscle strength measurement recommended for clinical practice, so that it is increasingly used for clinical diagnosis in elderly.17 Lower strength scores can be considered an independent predictor of overall mortality in the elderly over 85 years noninstitutionalized.18 The lower level physical fitness, lifestyle and excess weight are closely related to social isolation and physical mobility, and in some cases lead to loss of functional independence and neurological disorders, affecting performance cognitive test, as observed in this study. With increasing age, people become less active, their physical capabilities diminish and psychological changes appear as a feeling of old age, stress and depression. Concurrently, there is the appearance of chronic diseases that contribute to deteriorate the aging process; however, it seems that the disuse of physiological functions creates more problems than most of the effects of aging.16
In this sense, our study found that the balance was considered a protective factor for dementia. Since subjects with higher performance, in the balance of capacity, possibly present greater physical mobility and functional autonomy, which corroborates Borges et al.,19 appointed that the practice of physical activity and functional autonomy both promote rehabilitation, as maintaining the overall health of the elderly maintaining physical fitness, independence and autonomy in activities of daily living. Currently there are various methods for measuring body stability, which is an important component in maintaining the standing position of equilibrium and during daily activities and movements, especially for elderly people, since they are considered to fall-risk population.20 The system postural control depends on an intact ability (unharmed) to correctly perceive the environment by peripheral sensory system, as well as the processing and integration of proprioceptive pathways, visual and vestibular in the central nervous system.20
The risk of falls increases with aging, and can have a devastating effect on the independence and quality of life. Often it leads to a vicious cycle of inactivity with future decline in functionality, increased risk of falls, and more likely to need an attendant. Balance tests are useful tools to diagnose the loss of this physical ability. Encouraging seniors to improve physical feature can help them maintain independence and reduce the need for live assistance.21 Corroborating the findings of this study, Hanna et al.,22 indicated that the moderately active people presented a lower risk by mental disorders than those sedentary, showing that participation in physical exercise programs exerts benefits in the physical domain. Furthermore, psychologically and physically active people probably have a faster cognitive processing. This can be explained in part by a direct and indirect effect of exercise on cognitive function, such that the mechanisms that act directly increase the speed of cognitive processing, leading to an improvement in cerebral circulation and changes in the synthesis and degradation neurotransmitters.
In addition, direct mechanisms, such as low blood pressure, decrease in LDL and triglyceride in the blood plasma and inhibition of platelet aggregation appear to act indirectly by enhancing these functions and the overall functional capacity, reflecting in this way on mental health in the elderly.23 The prevalence data of our study were similar to those presented by Oliveira et al.,24 which also show that cognitive impairments in the elderly detected by the MMSE were not associated with the mobility test assessed by TSW. These results coincide with the literature and can be explained by the fact that some cases of dementia, patients have exessiva movement and unrest for much of the day. What they are not perceived in Alzheimer's dementia due to lack of extrapyramidal signs and motor slowness.
One limitation of the present data is the sample size and the disproportion between male and female elderly; however, the literature still lacks investigations like this, making relevant the results of this study. Another limitation was the instrument used since the MMSE despite being a widely used test, still lacks studies to better determine its use, as well as the adoption of appropriate points of cuts in the Brazilian population. Applicable, the present study showed low prevalence of dementia in the elderly; however, it is important to keep the concern for variables related to functional capacity, as well as the anthropometric profile, as they present relationship with the cognitive deficits.25-27 In this sense, health professionals should provide an environment that encourages physical activity safely, maintenance of functional capacity and avoidance of excess weight, particularly in the central part of the body.
In conclusion, the prevalence of dementia in the elderly was considered lower, however similar between male and female. Waist circumference and waist/height ratio showed predictive ability for dementia verified by MMSE, and seniors with greater deposition of fat in the central region of the body showed 5.6 times more likely to have dementia, while those with more balanced presence of a protective factor, with 15%, were less likely to have dementia.

