










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista de Osteoporosis y Metabolismo Mineral
versão On-line ISSN 2173-2345versão impressa ISSN 1889-836X
Rev Osteoporos Metab Miner vol.10 no.1 Madrid Jan./Mar. 2018 Epub 03-Abr-2023
https://dx.doi.org/10.4321/s1889-836x2018000100003
Originals
Relationship between the presence of anemia and the risk of osteoporosis in women with rheumatoid arthritis
1 Servicio Medicina Interna - Centro Médico ISSET (Instituto de Seguridad Social del Estado de Tabasco) - Villahermosa - Tabasco (México)
2 Departamento de Ciencias Biomédicas - Universidad Juárez Autónoma de Tabasco - Villahermosa - Tabasco (México)
Introduction:
Patients with rheumatoid arthritis present a high prevalence of osteoporosis, partly due to the use of glucocorticoids. However, there are other causal factors.
Material and methods:
122 women diagnosed with rheumatoid arthritis were studied. Serum hemoglobin concentrations were determined and bone densitometry carried out by dual energy X-ray absorptiometry. A multivariate logistic regression model was used to determine the association of the variables studied.
Results:
32.8% of the women studied presented hemoglobin <12 g/dL. The mean T-score in the lumbar spine was -1.8±1.5; 36.9% had a low bone mass, 32.8% osteoporosis criteria and 30.3% normal T-score. The mean of the femur T-score was -0.6±1.4; 63.9% was normal value, 23.8% presented low bone mass and 12.3% criterion of osteoporosis. Hemoglobin ≥12 g/dL and a bone mineral density (BMD) of the normal femur (p=0.003), and between hemoglobin <12 g/dL and BMD of femur with osteoporosis (p<0.000). There was an independent association between osteoporosis and body mass index <30 kg/m2 (OR=4.1, 95% CI: 1.4-11.4, p=0.009) and the presence of anemia (OR=8.9, 95% CI: 3.7-22.4, p=0.001).
Introduction
Patients with rheumatoid arthritis (RA), may suffer anemia associated with a chronic ailment, which tends to be normocytic, normochromic or, less frequently, microcytic, aregenerative with normal transferrin serum levels 1. Given the lack of effective treatment, anemia is very prevalent. It may range from 30 to 70%, according to different reported series 2.
Among the mechanisms involved in the development of anemia is the shortening of the useful life of erythrocytes, inadequate erythropoiesis, abnormalities in iron metabolism, as well as the inflammatory effect of cytokines, with interleukin-6 affecting hepcidin, a hormone that plays a significant role in the development of anemia in patients with RA. By decreasing iron levels, it regulates the transport of iron through the membranes and inhibits its intestinal absorption and release of iron, macrophages and hepatocytes 1.
Patients with RA usually have a higher risk of developing osteoporosis than the general population, increasing the risk of fractures and morbidity. The incidence is usually around 12-20% in the hip and spine 3.
Osteoporosis in patients with RA may be due to chronic inflammation, the activation and inhibition of bone cell function, modified body composition, the use of glucocorticoids, diet, low levels of physical activity and to the presence of anemia 4),5.
Researchers have linked the presence of anemia with osteoporosis. Excess effort of the hematopoietic system secondary to constant blood cell production in patients with anemia plays a major role in osteoporotic development. In support of this idea, hematological diseases that present chronic anemia (as in the case of beta thalassemia major, sickle cell anemia, chronic hemolytic anemia, pernicious anemia and hemophilia) have been found to concomitantly show osteoporosis 5.
A study in murine models reported that chronic blood loss produced an increase in the hematopoietic microenvironment, relatively reducing the amount of bone generated and activating its resorption process 6.
We carried out our study to determine the factors associated with osteoporosis of the femur (OF) and particularly, if the low levels of Hb (Hb <12 g/dL) are associated with OF in a female population with RA.
Material and methods
A descriptive, observational, retrospective study was carried out, in which patients older than 18 years were included with the diagnosis of RA, according to the ACR/EULAR 2010 criteria, that attended our Rheumatology outpatient service during the period of January to June 2016. Clinical records were reviewed and age, gender, history of diabetes mellitus, systemic arterial hypertension and smoking were recorded as variables; as well as factors associated with RA, such as the duration of the disease and the use of glucocorticoids or disease-modifying antirheumatic drugs (DMARDs), such as methotrexate, leflunomide, azathioprine; no patient received biological treatment. Anthropometric variables were also measured. The participation in the study was authorized by each patient signing an informed consent.
Measurement of anthropometric variables
The patients were weighed with a scale, previously calibrated, barefoot and with light clothing, expressing the results in kilograms. The height was measured by means of a standard height rod with the patient standing, expressing the results in meters. With these results, the body mass index (BMI) was calculated by means of the weight/height 2 formula (kg/m2), classifying the results in the low weight ranges: <18.5 kg/m2; normal: 18.5-24.9 kg/m2; overweight: 25-29.9 kg/m2; obesity: >30 kg/m2.
Determination of biochemical parameters
With a minimum fast of 8 hours, serum albumin concentrations were determined (considering as hypoalbuminemia <4 g/dL), ultrasensitive C-reactive protein (CRP-Us, considering as a cut-off value ≥2 mg/dL due to its association with cardiovascular risk); and hemoglobin (Hb) <12 g/dL as anemia, since it is the cut-off point set by the World Health Organization (WHO) for non-pregnant women 7. The positive rheumatoid factor (RF) was considered with values above 15 IU/mL. Anti-citrullinated cyclic peptide (APCC) antibody values >5 IU/mL were considered positive.
Disease activity
Disease activity was assessed using the DAS-28 PCR tool (Disease Activity Score-28 C-Reactive Protein), classifying as remission a score <2.3, mild activity ≥2.3 to <3.8, moderate activity ≥3.8 to <4.9 and severe activity ≥4.9.
Determination of bone mineral density (BMD)
A G.E. Lunar (Madison, Wisconsin, USA) was used to carry out a scan by dual-energy x-ray absorptiometry in the lumbar spine (L1-4) and in the right and left hips (femoral neck, trochanter and Ward triangle). The latter were added and the average of both hips was determined as a result.
The results of the T-score were interpreted in line with the WHO8: T-score ≥-1.0: normal bone mass; T-score between -1.0 and -2.5: low bone mass; T-score <-2.5: osteoporosis. In this study, a T-score of <-2.5 was defined as osteoporosis in the lumbar spine or in the total femur measurement.
Statistical analysis
A statistical analysis was carried out using the SPSS 22.0 package. A value of p≤0.05 was considered a significant result.
The Kolmogorov-Smirnov test was used to determine the normal distribution of variables. The continuous ones were presented as mean and standard deviation or median and interquartile range, depending on whether or not they had a normal distribution, and were compared with the Student's t test or the nonparametric Mann-Whitney test, respectively. The categorical variables were presented as frequencies and percentages and were compared with the Chi square test.
Finally, a multivariate logistic regression model was used, using the Stepwise Forward regression method to determine the association of the variables studied and the presence of osteoporosis.
Results
A total of 122 women diagnosed with RA were studied. The average age of the studied population was 56.3±10.4 years, with an average disease evolution time of 7.4±3.5 years. Table 1 shows the characteristics of the study population distributed according to the presence or not of osteoporosis. 29.5% had osteoporosis of the femoral or lumbar head. With regard to comorbidities, 35.2% had diabetes mellitus and 18.8% systemic arterial hypertension. Also 8.2% of the population under study were smokers.
Table 1 Relationship between the general characteristics and the presence of osteoporosis in women with RA

RIQ: interquartile range; BMI: body mass index; SD: standard deviation; PCR-Us: ultrasensitive C-reactive protein; DAS-28 PCR: Disease Activity Score; APCC: anti-citrullinated cyclic peptide antibodies.
*Significant result.
Regarding disease activity, 63.1% of the patients were in remission, 31.9% had mild activity, 3.3% had moderate activity and 1.7% had severe activity.
The BMI that prevailed was indicative of obesity (59.8%), followed by overweight (23.7%) and finally normal weight (16.5%). Mean BMI was 30.6±5.5 kg/m2.
It was found that 54.1% of the patients used glucocorticoids with a minimum of three months; 78.7% used methotrexate and 18.9% used leflunomide.
The results of the evaluated biochemical parameters reported a mean Hb of 12.6±1.3 g/dL 32.8% of the patients presented anemia, the mean of the CRP-Us was 3.4±9.1 mg/dL and that of serum albumin of 4.05±2.5 g/dL. 69.7% presented RF and 10.7% positive CCP.
The mean T-score in the lumbar spine was -1.8±1.5 and the mean BMD in this location was 0.88±0.19 g/cm2. Low bone mass predominated (36.9%), followed by osteoporosis (32.8%) while 30.3% presented normal bone mass. The mean femur T-score was -0.6±1.4 and the mean BMD was 0.83±0.23. In this location, the criterion of normal bone mass prevailed (63.9%), followed by low bone mass (23.8%) and osteoporosis (12.3%). The characteristics of the densitometric results and the Hb concentrations are summarized in table 2.
Table 2 Relationship between serum hemoglobin concentrations and values of lumbar and femur bone densitometry
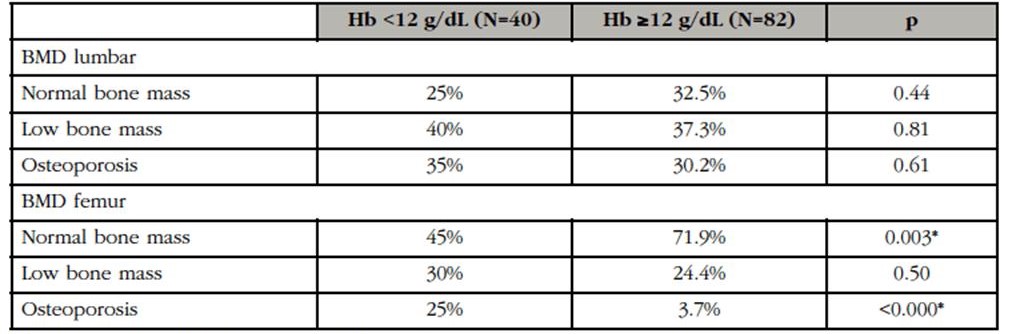
Hb: hemoglobin; BMD: bone mineral bone density.
*Significant result.
A multivariate logistic regression was performed with the presence of osteoporosis as dependent variables, determining its relation with the activity of the disease by DAS-28 CRP ≥2.3, BMI <30 kg/m2, age >55 years and Hb <12 g/dL. The results are summarized in table 3.

Discussion
We found that patients with RA and anemia ran a higher risk presenting osteoporosis compared to patients with normal Hb, mainly affecting the femoral bone density.
The frequency of anemia found in our population coincides with that reported in the literature 2.
It was found that women who presented a BMI less than 30 kg/m2 were more at risk of developing osteoporosis. This has been observed in multiple studies, mainly due to the fact that a higher body weight produces a greater mechanical load on the bone tissue, which results in an increase in bone mass. The effect of adipocytes and adipocytokines, such as leptin, waistband and amylin, has also been observed, which can act directly or indirectly on osteoblastic and osteoblastic activity, resulting in the formation of bone mass 9. On the other hand, adipose tissue indirectly protects against bone loss by providing a source and reservoir of peripheral conversion of androstenedione, which is the active metabolite of estrogen, whose decrease is associated with greater bone loss due to its regulatory effects on the immune system and on the oxidative stages and direct effects on bone cells 10.
When we compared the patients with or without osteoporosis and the presence of disease activity from slight to severe activity, with a cutoff of DAS-28 PCR ≥2.3 points, we found that women with osteoporosis had higher disease activity. This could be due to the impact brought on by inflammation in bone remodeling. The inflammation of the synovial joint increases cytokine expression, as is the case of tumor necrosis factor, IL-1 and IL-6, as well as the stimulating factor of macrophage colonies and the ligand of the nuclear factor activating receptor Kappa-β (RANK), which increase osteoclastogenesis and bone destruction 11. Based on the principle that the activation of T cells is fundamental for the etiology of RA and the presence of cytokine-like activity in media with activated T cells observed in previous investigations, Rifas et al. 12 conducted a study to identify the factors secreted by T cells that induce IL-6 by osteoblasts, stimulating osteoclastogenesis and osteoclast production independently of RANK. A cytokine was found which they termed SOFAT (secreted osteoclastogenic factor of activating T cells), which may exacerbate inflammation and bone turnover in inflammatory conditions, as is the case of RA.
However, although we found differences between the activity of the disease and the presence of osteoporosis, no significance was found when performing the logistic regression. This may be due to the fact that more than half of the patients were in remission and that most of the patients with activity were of the mild type, with less than 2% being of severe activity.
We found an association between anemia and the development of OF, as reported in the inCHIANTI study 13, which aimed to evaluate the relationship between bone mass and density measurements with anemia, finding that anemia and low Hb levels they are negatively and independently associated with bone mass and density, bordering on trabecular bone density (lumbar T-score) and mainly on cortical bone (T-score femoral).
Díaz et al. 14 carried out a study on Wistar rats, finding that iron deficiency anemia had a significant impact at the bone level, affecting its mineralization, decreasing the formation of the matrix and increasing its resorption, this associated to the metabolism of the Collagen It has been observed that iron participates in the enzymatic processes involved in the synthesis of collagen, which is an important component of bone tissue since about 90% is composed of collagen type I 15. It has also been observed that iron is necessary for the metabolism of vitamin D, since the cytochromes that are related to vitamin D use iron to carry out their actions 16.
Another explanation of the relationship between anemia and osteoporosis in patients with RA could be that observed in patients with sickle cell anemia, where bone loss is attributed to hyperplasia, to inflammation secondary to chronic anemia, to hypoxia and ischemia of the bone marrow 17.
Similarly, patients with anemia, regardless of etiology, have a higher degree of hypoxia, which is an important stimulator of bone resorption inducing osteoclastogenesis and later osteoblastogenesis 18.
A study by Rutten et al. 19 in patients with COPD found an association between low Hb levels and the development of osteoporosis, associating it with hypoxia and inflammation.
Among the limitations of our study is the failure to classify morphologically anemia, which could help determine the etiology. Microcytic anemia, for example, could be attributed to atrophic gastritis, which decreases acid secretion and leads to poor absorption of calcium ion, which may contribute to the development of osteoporosis. Furthermore, since this is a cross-sectional study, it cannot ascertain whether osteoporosis occurred before the development of anemia. Another limitation is the lack of determinations of vitamin D and parathormone levels. Finally, the failure to collect the prevalence of fragility fractures, which is the main clinical complication of osteoporosis is a further limitation.
Conclusions
From this study, we may conclude that there is a link between anemia and low bone mineral density in patients with RA mainly in the femoral region, although we cannot infer a causal relationship. Chronic anemia can predispose to bone loss, the development of osteoporosis and increase the risk of fractures. It is important to determine the hematological and bone parameters in our patients with RA, in order to correct Hb values and reduce the risk of fracture.
Conflict of interests: The authors declare they have no conflicts of interest in this study and they have followed all the ethical rules for conducting clinical studies.
Bibliografía
1. Masson C. Rheumatoid anemia. Joint Bone Spine. 2011;78:131-7. [ Links ]
2. Ganna S. The prevalence of anemia in rheumatoid arthritis. Rev Bras Reumatol. 2014;54:257-9. [ Links ]
3. Lodder MC, Haugeberg G, Lems WF, Uhlig T, Orstavik RE, Kostense PJ. Radiographic damage associated with low bone mineral density and vertebral deformities in rheumatoid arthritis: the Oslo-Truro-Amsterdam (OSTRA) collaborative study. Arthritis Rheum. 2003;49:209-15. [ Links ]
4. Sarkis KS, Salvador MB, Pinheiro MM, Silva RG, Zerbini CA, Martini LA. Association between osteoporosis and rheumatoid arthritis in women: a cross-sectional study. Sao Paulo Med J. 2009;127:216-22. [ Links ]
5. Gurevitch O, Salvin S. The hematological etiology of osteoporosis. Med Hypotheses. 2006;67:729-35. [ Links ]
6. Gurevitch O, Khitrin S, Valitov A, Slavin S. Osteoporosis of hematologic etiology. Exp Hematol. 2007;35:128-36. [ Links ]
7. Beutler E, Waalen J. The definition of anemia: what is the lower limit of normal of the blood hemoglobin concentration? Blood. 2006;107:1747-50. [ Links ]
8. Prevention and management of osteoporosis. World Health Organ Tech Rep Ser. 2003;921:1-164. [ Links ]
9. Mazocco L, Chagas P. Association between body mass index and osteoporosis in women from northwestern Rio Grande do Sul. Rev Bras Reumatol. 2017;57:299-305. [ Links ]
10. Khosla S, Oursler MJ, Monroe DG. Estrogen and the skeleton. Trends Endocrinol Metab. 2012;23:576-81. [ Links ]
11. Manzano F, Riesco M. Osteoporosis en la artritis psoriasica. Semin Fund Esp Reumatol. 2013;14:72-9. [ Links ]
12. Rifas L, Weitzmann M. A novel T cell cytokine, secreted osteoclastogenic factor of activated T cells, induces osteoclast formation in a RANKL-independent manner. Arthritis Rheum. 2009;60:3324-35. [ Links ]
13. Cesari M, Pahor M, Lauretani F, Penninx BW, Bartali B, Russo R, et al. Bone density and hemoglobin levels in older persons: results from the InCHIANTI study. Osteoporos Int. 2005;16:691-99. [ Links ]
14. Díaz-Castro J, López-Frías MR, Campos MS, López Frías M, Alférez MJ, Nestares T, et al. Severe nutritional iron-deficiency anaemia has a negative effect on some bone turnover biomarkers in rats. Eur J Nutr. 2012;51:241-7. [ Links ]
15. Schaffler MB, Cheung WY, Majeska R, Kennedy O. Osteocytes: Master orchestrators of bone. Calcif Tissue Int. 2014;94:5-24. [ Links ]
16. Jones G, Prosser DE, Kaufmann M. Cytochrome P450-mediated metabolism of vitamin D. J Lipid Res. 2014;55:13-31. [ Links ]
17. Gupta R, Marouf R, Adekile A. Pattern of bone mineral density in sickle cell disease patients with the high-Hb F phenotype. Acta Haematol. 2010;123:64-70. [ Links ]
18. Arnett TR, Gibbons DC, Utting JC, Orriss IR, Hoebertz A, Rosendaal M, et al. Hypoxia is a major stimulator of osteoclast formation and bone resorption. J Cell Physiol. 2003;196:2-8. [ Links ]
19. Rutten EP, Franssen FM, Spruit MA, Wouters EF. Anemia is Associated with Bone Mineral Density in Chronic Obstructive Pulmonary Disease. CODP. 2013;10:286-92. [ Links ]
Received: May 17, 2017; Accepted: November 14, 2017
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
