










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista de Osteoporosis y Metabolismo Mineral
On-line version ISSN 2173-2345Print version ISSN 1889-836X
Rev Osteoporos Metab Miner vol.10 n.4 Madrid Nov./Dec. 2018 Epub Apr 03, 2023
https://dx.doi.org/10.4321/s1889-836x2018000400004
Original Articles
Bone tissue mechanical strength is independent of age in healthy individuals
1Grupo de Investigación Musculoesquelética. IMIM (Instituto Hospital del Mar de Investigaciones Médicas). Centro de Investigación Biomédica en Red de Fragilidad y Envejecimiento Saludable (CIBERFES). Universidad Autónoma de Barcelona. Barcelona (España)
2Consejo Nacional de Investigación. Instituto de Fisiología Clínica. Lecce (Italia)
Objective:
Impact microindentation (IMI) is a technique that allows the measurement of mechanicalbone tissue resistance in vivo. IMI has proven to provide useful information on the evaluation of skeletal diseases, but the effect of age on the bone property that is measured by this technique is unknown. This study aims to analyzethe relationship between age and MIH.
Materials and methods:
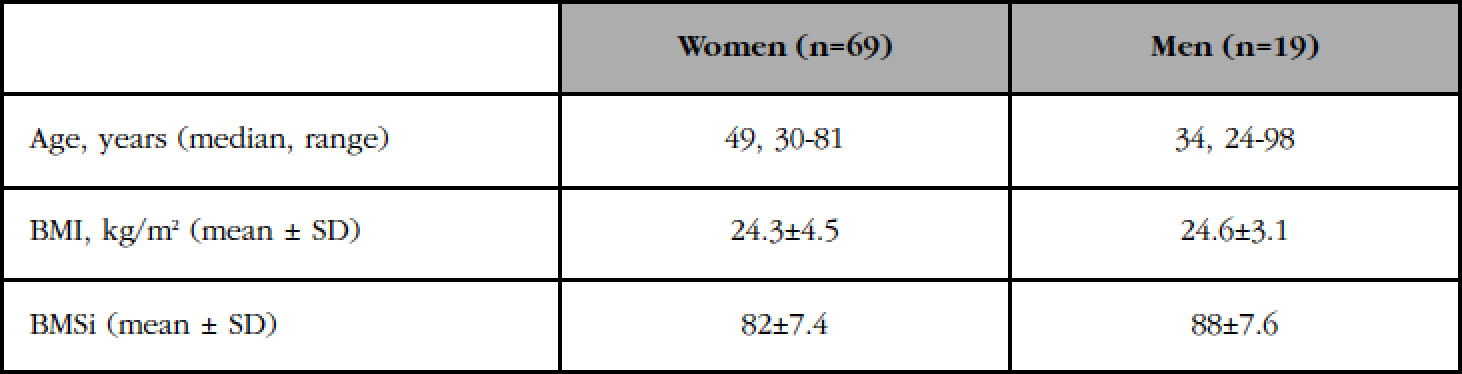
Bone Material Strength index (BMSi), IMI’s output variable, was measured in 69 healthy women (median age: 49 years, range: 30-81 years) and 19 healthy men (median age: 34 years, range: 24-98 years). The correlation between BMSi and age was analyzed by linear regression. The association between BMSi and age was evaluated by ANOVA after adjusting for body mass index. The potential effect of postmenopausal estrogenic depletion on BMSi was studied by comparing the younger vs the older subset of women through a t-student test.
Results:
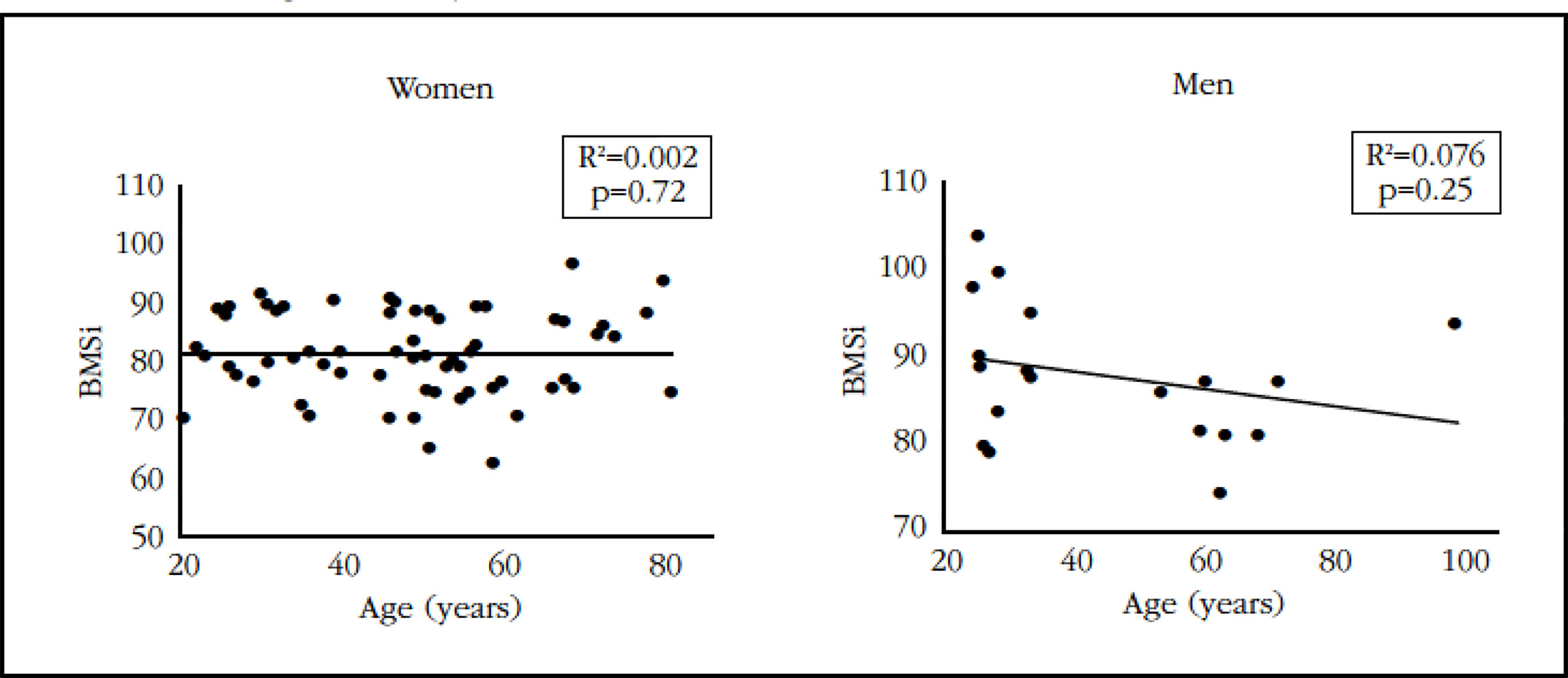
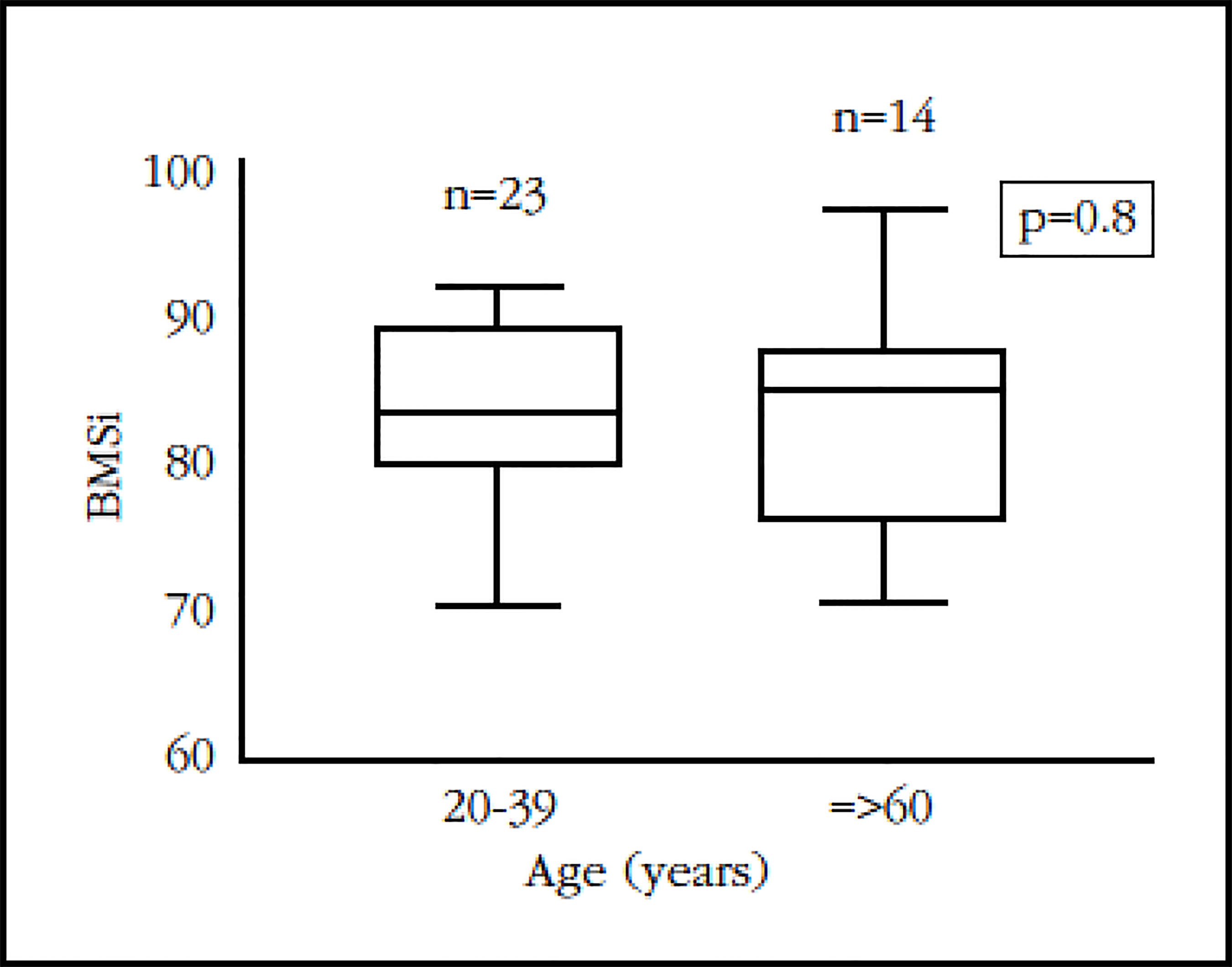
Linear regression analysis showed that BMSi was not correlated with age in either men (R2=0.0016, p=0.74) or women (R2=0.076, p=0.25). Similarly, the BMI-adjusted ANOVA model revealed a lack of association of BMSi with age in men (p=0.78) and women (p=0.73). Finally, there were not significant differences on BMSi detected between the younger and the older subset of women (p=0.8).
Conclusions:
Bone tissue mechanical resistance in healthy individuals is independent of age and postmenopausal estrogenic depletion.
Key words impact microindentation; Bone Material Strength index (BMSi)
Introduction
Osteoporotic fractures pose a serious public health problem given their high prevalence and enormous impact in terms of morbidity, mortality and economic cost1. Hence there is considerable interest in understanding the underlying pathophysiology of bone fragility, which, from a mechanical standpoint, is determined by bone strength. Bone resistance, in turn, comes from the integration of bone mineral quantity, bone architecture, and the material properties of bone.
The mineral quantity of the bone is usually measured by bone densitometry (DXA), the most commonly used, standardized method for assessing bone mass and fracture risk2. Bone architecture, both at the micro- and macroscopic level, is examined using different imaging techniques, including high-resolution peripheral quantitative tomography, bone magnetic resonance and the more accessible Trabecular Bone Score3. However, the material properties of bone are difficult to assess due to its high complexity, reflected in its multiple constituents including non-collagenous proteins, crystallinity, hydration of bone tissue, and the characteristics of mineralization and collagen, among others4,5. Furthermore, as researchers need bone tissue samples for analysis, the study of these properties has traditionally been restricted to a few centers specialized in bio-mechanics.
Microindentation has been developed as a technique to measure the material properties of bone easily and non-invasively. However, the property specifically measured has not yet been determined, so for the time being, the mechanical strength of the bone is evaluated globally. This technique involves measuring the penetration distance of a needle in the cortical bone to gauge its mechanical resistance6. The procedure is usually carried out on the anteromedial side of the tibia in a practical, safe and painless way7. There are currently two types of clinical microindentation: the cyclic microindentation, using the BioDent® instrument (Active Life Scientific Inc., Santa Barbara, USA). The other is impact microindentation (IMI), carried out with the OsteoProbe®. Several clinical studies can provide relevant information on bone strength and risk of fracture with both types6,8. However, given its greater manageability, OsteoProbe® has replaced BioDent® in clinical studies. Despite its increasing use, there are still many unresolved basic issues surrounding IMI implementation including the effect of age on bony material properties. We examined the influence of age on bone tissue mechanical strength in a cohort of healthy men and women.
Material and methods
Participants
Healthy volunteers older than 18 years of age were recruited consecutively from Internal Medicine outpatient lists without bone metabolism-related diseases.
Those individuals with the following criteria were excluded from the study:
History of fragility fractures or traumatic fractures of the tibia.
History of primary bone diseases (including osteoporosis), secondary bone diseases, deformities in the lower extremities of congenital or acquired origin, and bone metastasis.
History of diabetes mellitus, chronic kidney disease and severe liver failure.
Previous or concurrent treatment with glucocorticoids, aromatase inhibitors, androgen deprivation therapy, chemotherapy and antiresorptive agents or osteo formers (bisphosphonates, teriparatide, denosumab, strontium ranelate and selective modulators of the estrogen receptor).
Participants’ height and weight were measured to calculate the body mass index (BMI, kg/m2).
The study protocol was approved by the Ethics Committee of the Mar Health Park and written informed consent of all the participants obtained.
Impact Microindentation
Impact microindentation (IMI) was evaluated using OsteoProbe®, a hand-held device with an impact mechanism, a disposable probe with a conical tip (radius of tip sharpness: <10 µm) and a displacement transducer. The procedure has been described in detail previously7. Prior to microindentation, a local anesthetic (2% mepivacaine) is applied to the anteromedial part of the non-dominant tibia. The probe is then inserted perpendicular to the bony cortex in the anesthetized region until it reaches the bone surface. The device is slowly compressed until it reaches a pre-load resistance of 10 Newtons (N), after which an impact load of 30 N is automatically activated. The displacement transducer measures indentation depth. The operator can eliminate the measurements that are considered incorrect.
After 8 valid indentations separated by approximately 2 mm, 5 additional indentations are made with the same probe in a polymethyl methacrylate (PMMA) block for calibration. The value obtained in the IMI is the Bone Mineral Resistance Index (or BMSi, from Bone Material Strength index), which is defined as 100 times the relation between the harmonic mean of the distance of the 8 bony indentations and that of the 5 indentations in the PMMA block. Nine different operators with experience in the technique carried out the measurements in our study.
Statistical analysis
Separate analyzes were carried out for women and men. Descriptive values are shown using mean and standard deviation, as well as median and total range, as appropriate. The correlation between age and BMSi was represented by a linear regression, and its association with BMI-adjusted ANOVA evaluated. Due to the lack of clinical information on the menstrual status of the participants, the potential effect of estrogen deprivation on the mechanical resistance of bone tissue was analyzed by comparing the BMSi of women between 20-39 years (most likely premenopausal) with women >60 years (most likely postmenopausal) using Student's t test.
The study figures were obtained through the Prism 7 program (GraphPad Software, La Jolla, California, USA). The statistical analyzes were performed with the SPSS program version 23 (IBM Corp®, Armonk, New York, USA), accepting as significant the results with p<0.05.
Results
For our study, 69 women and 19 men of Caucasian origin were recruited. The participants’ characteristics and the BMSi measurements are shown in table 1. The coefficient of inter-operator variation was less than 5%.
Linear regression analyzes showed that BMSI does not correlate with age in women (R2=0.076, p=0.25) nor in men (R2=0.0016, p=0.74) (Figure 1). Likewise, no significant associations were detected between the BMSi and the age in the ANOVA analysis adjusted for BMI neither in women (p=0.73) nor in men (p=0.78). Finally, no significant differences were observed in the BMSi between the subgroup of women aged 20-39 years and those older than 60 years (p=0.8) (Figure 2).
Discussion
In the present study, the influence of age on the mechanical resistance of bone tissue measured by IMI in a cohort of healthy men and women was evaluated. The results indicate that bone tissue resistance is not determined by age in women or men, and that therefore, it is not affected by aging. Furthermore, no BMSi differences were found between the subset of younger women versus the subset of older women which would indicate that the depletion of estrogen that accompanies menopause does not exert a significant effect on the mechanical resistance of the bone tissue.
Bone microindentation has emerged as a promising new tool to evaluate bone mechanical resistance in living individuals6-8. Although it is still unclear which physical properties are specifically measured, several clinical studies reveal that this technique has a good discriminant capacity between patients with and without fragility fractures9-11, although studies in geriatric populations with osteoporotic fractures show discrepancies12.
The measurements that result in an altered BMSi seem to be especially informative in those conditions associated with an increased fracture risk that are not explained by abnormal BMD values13-16.
Given the increasing use of IMI as a complementary technique for assessing bone health in clinical research and its potential future role in clinical practice, it is imperative to clarify the possible effects of physiological factors, such as age, on the mechanical resistance of the bone tissue.
Our study results indicate that BMSi is not significantly affected by aging or estrogenic depletion. Mirzaali MJ, et al. observed through micromechanical studies in cadaver bone that the properties of microindentation in the elderly were constant with age17 which concurs with our study. On the contrary, aging and estrogenic depletion reportedly exert a negative effect on BMD and bone architecture18,19. This reinforces the notion that the microindentation technique measures a very specific characteristic of bone strength or bone quality completely different from other techniques available to date. Microindentation may cause the separation of the protein-based "glue" proteins, which hold together the mineralized collagen fibrils, a property that would constitute the first barrier of resistance to fracture20.
Currently, bone tissue resistance is considered to be genetically determined, but, at the same time, clinical studies show that it can be negatively influenced by non-genetic factors, such as a deficient glycemic control13,15,21, an excess of tissue local adipose16, treatment with glucocorticoids22, excess growth hormone23, chronic kidney disease24,25 and HIV infection26. In addition, alterations in certain signaling pathways and in the intracellular storage of lipids also seem to affect the mechanical resistance of bone tissue as has been observed in studies on the diseases of Camuratti-Englemann27 and Gaucher type 128, respectively.
Our study has several limitations. First, the small number of subjects included in the study limits the generalization of our findings. Another limitation is that the factors that can affect the mechanical resistance of the bone tissue are not yet fully known. Therefore, these factors have not been introduced as co-variates in the statistical model for the adjustment of the confounding factor. This has been tried to compensate by means of the strict exclusion criteria used at the moment of the recruitment of the individuals and thus control the possible heterogeneity of the studied cohort.
Another limitation lies in the fact that this technique is performed exclusively on the cortical bone of the anteromedial tibia, so the generalization of BMSi results to other skeletal sites is debatable. However, we believe that the values obtained by microindentation in the tibia reflect the mechanical strength of the bone globally, since clinical studies have shown an inverse correlation between BMSI values and the incidence of osteoporotic fractures in other skeletal locations such as hip, and even in bones with a greater trabecular component, such as the vertebrae10,11. Finally, the data on the menstrual status were not collected, thus limiting the evaluation of the effects of menopause on the mechanical resistance of the bone tissue. This problem was counteracted by categorizing the subgroup of younger women as premenopausal and the subset of older women as postmenopausal.
In conclusion, the mechanical resistance of the bone tissue does not seem to be affected by aging and estrogen-related depletion related to menopause. Additional studies are needed to corroborate these findings in order to facilitate the implementation of the IMI in research and clinical practice.
Bibliografía
1 Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17(12):1726-33. [ Links ]
2 Leslie WD, Brennan-Olsen SL, Morin SN, Lix LM. Fracture prediction from repeat BMD measurements in clinical practice. Osteoporos Int. 2016;27(1):203-10. [ Links ]
3 Hans D, Goertzen AL, Krieg MA, Leslie WD. Bone microarchitecture assessed by TBS predicts osteoporotic fractures independent of bone density: the Manitoba study. J Bone Miner Res. 2011;26(11):2762-9. [ Links ]
4 Bala Y, Seeman E. Bone's material constituents and their contribution to bone strength in health, disease, and treatment. Calcif Tissue Int. 2015;97(3):308-26. [ Links ]
5 Fantner GE, Hassenkam T, Kindt JH, Weaver JC, Birkedal H, Pechenik L, et al. Sacrificial bonds and hidden length dissipate energy as mineralized fibrils separate during bone fracture. Nat Mater. 2005;4(8):612-6. [ Links ]
6 Allen MR, McNerny EM, Organ JM, Wallace JM. True gold or pyrite: a review of reference point indentation for assessing bone mechanical properties in vivo. J Bone Miner Res. 2015;30(9):1539-50. [ Links ]
7 Diez-Perez A, Bouxsein ML, Eriksen EF, Khosla S, Nyman JS, Papapoulos S, et al. Technical note: Recommendations for a standard procedure to assess cortical bone at the tissue-level in vivo using impact microindentation. Bone Rep. 2016;5:181-5. [ Links ]
8 Herrera S, Diez-Perez A. Clinical experience with microindentation in vivo in humans. Bone. 2017;95: 175-82. [ Links ]
9 Malgo F, Hamdy NA, Papapoulos SE, Appelman-Dijkstra NM. Bone material strength as measured by microindentation in vivo is decreased in patients with fragility fractures independently of bone mineral density. J Clin Endocrinol Metab. 2015;100(5):2039-45. [ Links ]
10 Malgo F, Hamdy NAT, Papapoulos SE, Appelman-Dijkstra NM. Bone material strength index as measured by impact microindentation is low in patients with fractures irrespective of fracture site. Osteoporos Int. 2017;28(8):2433-7. [ Links ]
11 Sosa DD, Eriksen EF, Reduced bone material strength is associated with increased risk and severity of osteoporotic fractures. An impact microindentation study. Calcif Tissue Int. 2017;101(1):34-42. [ Links ]
12 Rozental TD, Walley KC, Demissie S, Caksa S, Martinez-Betancourt A, Parker AM, et al. Bone material strength index as measured by impact microindentation in postmenopausal women with distal radius and hip fractures. J Bone Miner Res. 2018;33(4):621-6. [ Links ]
13 Farr JN, Drake MT, Amin S, Melton LJ, 3rd, McCready LK, Khosla S. In vivo assessment of bone quality in postmenopausal women with type 2 diabetes. J Bone Miner Res. 2014;29(4):787-95. [ Links ]
14 Guerri-Fernandez RC, Nogues X, Quesada Gomez JM, Torres Del Pliego E, Puig L, Garcia-Giralt N, et al. Microindentation for in vivo measurement of bone tissue material properties in atypical femoral fracture patients and controls. J Bone Miner Res. 2013;28(1):162-8. [ Links ]
15 Nilsson AG, Sundh D, Johansson L, Nilsson M, Mellstrom D, Rudang R, et al. Type 2 Diabetes melli-tus is associated with better bone microarchitecture but lower bone material strength and poorer physical function in elderly women: a population-based study. J Bone Miner Res. 2017;32(5):1062-71. [ Links ]
16 Sundh D, Rudang R, Zoulakis M, Nilsson AG, Darelid A, Lorentzon M. A high amount of local adipose tissue is associated with high cortical porosity and low bone material strength in older women. J Bone Miner Res. 2016;31(4):749-57. [ Links ]
17 Mirzaali MJ, Schwiedrzik JJ, Thaiwichai S, Best JP, Michler J, Zysset PK, et al. Mechanical properties of cortical bone and their relationships with age, gender, composition and microindentation properties in the elderly. Bone. 2016;93:196-211. [ Links ]
18 https://www.nof.org/patients/what-is-osteoporosis/ [ Links ]
19 Dufour R, Winzenrieth R, Heraud A, Hans D, Mehsen N. Generation and validation of a normative, age-specific reference curve for lumbar spine trabecular bone score (TBS) in French women. Osteoporos Int. 2013;24(11): 2837-46. [ Links ]
20 Hansma PK, Fantner GE, Kindt JH, Thurner PJ, Schitter G, Turner PJ, et al. Sacrificial bonds in the interfibrillar matrix of bone. J Musculoskelet Neuronal Interact. 2005;5(4):313-5. [ Links ]
21 Furst JR, Bandeira LC, Fan WW, Agarwal S, Nishiyama KK, McMahon DJ, et al. Advanced glycation endproducts and bone material strength in type 2 diabetes. J Clin Endocrinol Metab. 2016;101(6):2502-10. [ Links ]
22 Mellibovsky L, Prieto-Alhambra D, Mellibovsky F, Guerri-Fernandez R, Nogues X, Randall C, et al. Bone tissue properties measurement by reference point indentation in glucocorticoid-induced osteoporosis. J Bone Miner Res. 2015;30(9):1651-6. [ Links ]
23 Malgo F, Hamdy NA, Rabelink TJ, Kroon HM, Claessen KM, Pereira AM, et al. Bone material strength index as measured by impact microindentation is altered in patients with acromegaly. Eur J Endocrinol. 2017;176(3):339-47. [ Links ]
24 Perez-Saez MJ, Herrera S, Prieto-Alhambra D, Nogues X, Vera M, Redondo-Pachon D, et al. Bone density, microarchitecture, and tissue quality long-term after kidney transplant. Transplantation. 2017;101(6):1290-4. [ Links ]
25 Perez-Saez MJ, Herrera S, Prieto-Alhambra D, Vilaplana L, Nogues X, Vera M, et al. Bone density, microarchitecture, and material strength in chronic kidney disease patients at the time of kidney transplantation. Osteoporos Int. 2017;28(9):2723-7. [ Links ]
26 Guerri-Fernandez R, Molina D, Villar-Garcia J, Prieto-Alhambra D, Mellibovsky L, Nogues X, et al. Brief Report: HIV infection is associated with worse bone material properties, independently of bone mineral density. J Acquir Immune Defic Syndr, 2016;72(3):314-8. [ Links ]
27 Herrera S, Soriano R, Nogues X, Guerri-Fernandez R, Grinberg D, Garcia-Giralt N, et al. Discrepancy between bone density and bone material strength index in three siblings with Camurati-Engelmann disease. Osteoporos Int. 2017;28(12):3489-93. [ Links ]
28 Herrera S, Perez-Lopez J, Molto-Abad M, Guerri-Fernandez R, Cabezudo E, Novelli S, et al. Assessment of bone health in patients with type 1 Gaucher disease using impact microindentation. J Bone Miner Res. 2017;32(7):1575-81. [ Links ]
Received: June 19, 2018; Accepted: July 27, 2018
 Este es un artículo publicado en acceso (Open Access) abierto bajo la licencia Creative Commons Attribution Non-Commercial, que permite su uso, distribución y reproducción en cualquier medio, sin restricciones siempre que sin fines comerciales y que el trabajo original sea debidamente citado.
Este es un artículo publicado en acceso (Open Access) abierto bajo la licencia Creative Commons Attribution Non-Commercial, que permite su uso, distribución y reproducción en cualquier medio, sin restricciones siempre que sin fines comerciales y que el trabajo original sea debidamente citado.
