










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista de Osteoporosis y Metabolismo Mineral
On-line version ISSN 2173-2345Print version ISSN 1889-836X
Rev Osteoporos Metab Miner vol.12 n.4 Madrid Oct./Dec. 2020 Epub Apr 05, 2021
https://dx.doi.org/10.4321/s1889-836x2020000400009
POSITION PAPER
COVID-19 and vitamin D. Position paper of the Spanish Society for Bone Research and Mineral Metabolism (SEIOMM)
1Internal Medicine Service. Río Hortega University Hospital. Valladolid (Spain)
2Rheumatology Service. Parc Tauli University Hospital. Sabadell (Spain)
3Bone and Mineral Metabolism Clinical Management Unit. Central University Hospital of Asturias. Health Research Institute of the Principality of Asturias (ISPA). Oviedo (Spain)
4Rheumatology Service. Clinical hospital. Barcelona (Spain)
5Internal Medicine Service. Marqués de Valdecilla University Hospital. Santander (Spain)
INTRODUCTION
Vitamin D exerts its effect mainly through its active metabolite, 1,25-dihydroxycholecalciferol, by binding to a receptor with wide distribution in the different cells of the body. This receptor regulates the expression of genes involved in different biological functions, including organ development, cell cycle control, phosphocalcic metabolism, detoxification, and control of innate and adaptive immunity1,2. Regulation of the vitamin D receptor is determined by interacting environmental, genetic, and epigenetic factors.
Vitamin D increases intestinal absorption and tubular reabsorption of calcium, inhibiting PTH synthesis. This leads to a reduction in bone turnover, which helps maintain its strength and reduce the risk of fractures. In addition, it exerts an intraosseous effect, facilitating the mineralization of the matrix, which prevents the development of rickets in children and osteomalacia in adults. Numerous studies have been published showing an association between low levels of vitamin D and various chronic diseases, such as cancer, diabetes, cardiovascular diseases, multiple sclerosis, and infectious diseases, among others3. These associations can be explained through different pathophysiological mechanisms related to vitamin D deficiency.
In 2020, the pandemic derived from COVID-19 occurred with a high rate of contagion and mortality. The seriousness of the process has made it necessary to apply therapeutic measures without clear scientific evidence4. Many of them have not proved effective in subsequent cohort studies and clinical trials of a different nature, so they have been withdrawn. Some have shown usefulness in certain periods of the disease.
Vitamin D is a hormone whose deficiency has been associated with numerous acute and chronic diseases, both bone and non-bone. However, the studies carried out to demonstrate the causality of the association, in general, have not been positive. The fact that various risk factors associated with the incidence and severity of COVID-19, such as north latitude, advanced age, non-Caucasian races, high blood pressure and diabetes, have also been associated with vitamin D deficiency5, suggesting the possible link between COVID-19 infection and vitamin D deficiency.
This leads to the following questions:
- Is there a relationship between vitamin D deficiency and the risk of coronavirus infection?
- Is there a biological explanation for this association?
- Can the administration of vitamin D to deficient individuals prevent infection or alter its severity?
- What is the risk/benefit ratio of its administration?
Is there a relationship between vitamin D deficiency and the risk of coronavirus infection?
Initially, mortality from COVID-19 was reportedly higher in northern latitudes, which could be attributed to decreased production of vitamin D due to the effect of ultraviolet radiation. However, Spain and Italy, located in southern Europe, presented a very high mortality, as well as a high prevalence of hypovitaminosis D6. Illie et al.7 carried out an ecological study in 20 European countries. They found an inverse relationship of vitamin D levels with the incidence of COVID-19 (r:-0.443; p=0.05) and mortality due to disease (r:-0.4378; p=0.05). In another study carried out in 117 countries, an association between latitude and mortality was observed (p<0.033), after adjusting for age8. Meltzer et al.9, in a 489-patient cohort, with 75% women, found that COVID-19 infection risk was associated with advanced age, non-Caucasian race and vitamin D deficiency. The risk of infection in individuals with vitamin D sufficiency was 12.2%, compared to 21.6% in those with insufficiency (p=0,02). D’Avalio et al.10 reported that patients with positive PCR had vitamin D levels of 11.1 ng/ml, while, among those with negative PCR for COVID-19, the levels were 24.6 ng/ml; p=0.004. Another study linked vitamin D levels with mortality, finding that patients with vitamin D below 10 ng/ml had a 50% chance of dying, compared to 5% of those with a higher level, although the study sample size was small11. Hernández et al.12 found lower levels of vitamin D in hospitalized patients, unrelated to the severity of the disease, although they observed an inverse relationship with the levels of ferritin and Ddimer, both parameters related to the severity of the infection.
The relationship between low vitamin D levels and the risk of infection by COVID-19 has been observed in a recent meta-analysis13. Pereira et al.14 conducted a meta-analysis that included 8,176 patients with COVID19 infection. These authors did not find a relationship between vitamin D deficiency and an increased risk of infection, but did find a relationship with its severity. A study conducted in England with biobank samples also found no association between vitamin D and COVID1915. It must be taken into account that, in critical patients, there is a high prevalence of vitamin D deficiency, although we do not know if it is an “innocent bystander”, a marker of severity or a real and modifiable risk factor. The stimulation of renal 1α-hydroxylase in the face of inflammatory processes means that the association of various acute processes has the possibility of being an effect rather than a cause, with 25-hydroxyvitamin D levels being a negative acute phase reactant16.
So, although the studies carried out have different approaches and their results are not uniform, in general an association, not necessarily causal, is observed between vitamin D deficiency and the incidence and mortality from COVID-19.
Is there a biological explanation for the association between vitamin D deficiency and incidence and mortality?
Vitamin D may play a role in reducing the incidence and mortality of COVID-19 through various mechanisms, such as the maintenance of epithelial integrity, the production of antimicrobial peptides, the reduction of the inflammatory response and the modification of the relationship between ACE/ACE2 (classical angiotensin converting enzyme/angiotensin converting enzyme 2) by increasing ACE2 expression.
a) Epithelial integrity: vitamin D stimulates the expression of gap protein and tight junction protein that help to maintain the integrity of the epithelium, preventing the penetration of the virus. Furthermore, it acts indirectly by stimulating autophagy and facilitating the death of epithelial cells occupied by the virus. This effect is carried out through modulation of the mTOR metabolic pathway17.
b) Production of antimicrobial peptides: 25-hydroxycholecalciferol is transformed into 1,25-dihydroxycholecalciferol (calcitriol) at the level of monocytes and macrophages that express CYP27B1 (1-α hydroxylase), and facilitates the development of antigen-presenting cells. Calcitriol stimulates the production of cathelicidin, defensin and NOD2 (nucleotide binding oligomerization domain-containing protein 2), facilitating the destruction of microorganisms. In addition, it increases the synthesis of hepcidin, which accumulates iron at the cellular level, preventing its use by microorganisms and stimulates the production of nitric oxide and superoxide. All these proteins have an antiviral action and are produced by stimulating innate immunity18,19.
c) Stimulation of innate immunity, mediated by vitamin D, decreases the proliferation of types 1 and 17 helper T lymphocytes and increases that of helper 2 lymphocytes and regulatory T lymphocytes. The result is a decrease in pro-inflammatory cytokines (IL1, IL6, IL12, TNFα, IL17, and interferon γ) and an increase in anti-inflammatory cytokines (IL10). This decrease in inflammatory cytokines can be mediated through the metabolic pathway of NFkβ. All these effects modify acquired immunity17,20.
d) The entry of SARS-COV-2 into the body's cells, and, therefore, the start of the infectious process, is carried out through the ACE 2 receptor. A paradoxical phenomenon occurs, since ACE 2 is expressed less intensely in men and the elderly who, on the other hand, are those who present a greater risk of serious infection by COVID1921. Vitamin D is a potent renin inhibitor, so its administration facilitates a decrease in the classic ACE/ACE2 ratio that reduces cardiovascular morbidity and mortality.
All these facts represent the biological bases that could explain the possible beneficial effect of vitamin D.
Can administering vitamin D to deficient individuals prevent infection or alter its severity?
The evidence to indicate the administration of vitamin D in the prevention or treatment of COVID-19 is scarce and presents numerous limitations.
At this time, we do not know the vitamin D threshold that must be reached to achieve the objective, the most suitable metabolite or the doses to be used.
Can administering vitamin D to deficient individuals prevent infection or alter its severity?
A meta-analysis that included more than 11,000 patients, from 25 clinical trials, showed a beneficial effect of vitamin D in reducing infectious diseases of the respiratory tract. The effect was greater in situations with severe vitamin D deficiency (<10 ng/ml) and with daily or weekly administrations22. Taking into account these data, the existence of hypovitaminosis D in patients with COVID-19 and a biological explanation that offers plausibility to a beneficial effect, 18 clinical trials have been proposed that try to demonstrate this hypothesis10. The beneficial effects could take place both in the early viremic phases, preventing the development of the disease, and in late hyperinflammatory phases.
However, the evidence available so far is very scarce. Several case/control studies have been published that we can call quasi-experimental and a pilot study from a cohort of patients infected with pneumonia (Table 1). Their sample size is small, except for one of them, which included 1,476 patients. Some favorable results have been obtained, although their limitations should be taken into account23-28. There are no data on baseline and final 25-hydroxyvitamin D values, although they all assess important outcome variables, such as incidence of disease and mortality.
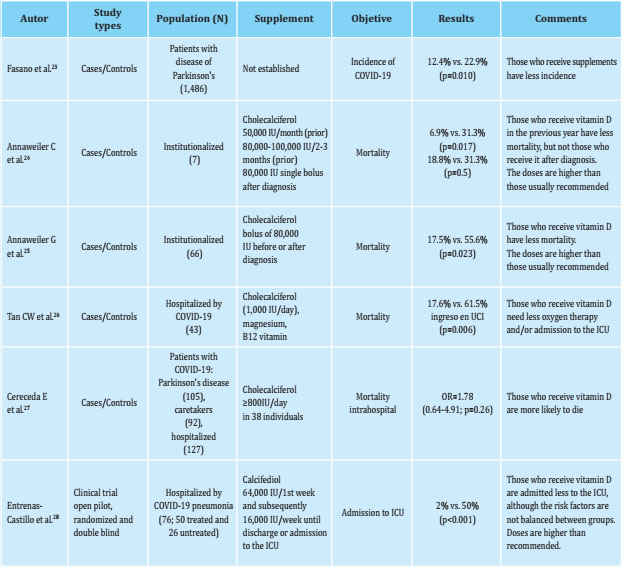
Some studies in an institutionalized geriatric population that analyze the effect of boluses of cholecalciferol (80,000 IU) prior and/or at the time of infection, report a better evolution of the disease and a decrease in mortality, while in other studies of the same characteristics, this effect is observed in individuals who are treated with periodic boluses of cholecalciferol during the year prior to infection24,25. In both cases, the doses used are higher than those recommended. In a study carried out in China with a cohort of asymptomatic patients with COVID-19, the effect of the administration of supplements associating cholecalciferol (1,000 IU), magnesium and vitamin B12 on the evolution of the disease was assessed26. Those who received supplements were admitted to the intensive care units (ICU) less and required less oxygen therapy. However, another study, with cholecalciferol, did not confirm these data. The administration of supplements was associated with a tendency to increase mortality, although not statistically significant27. However, it is important to mention the methodological limitations of these studies. The only study with calcifediol (25-hydroxyvitamin D) has been carried out in Spain and shows a reduction in the severity of the disease and in mortality. Relatively high doses of calcifediol were used (0.532 mg, followed by 0.266 mg at 3 and 7 days and subsequently weekly until the patient was discharged), without baseline or during vitamin D treatment determinations, which could raise safety concerns28. In fact, with the administration of calcifediol (0.266 mg) every two weeks, 25-hydroxyvitamin D concentrations greater than 30 ng/ml are reached in most individuals. Although with this type of dosage, the development of hypercalcemia, around 38% of individuals present concentrations greater than 60 ng/ml29. Another study with weekly dosing showed mean concentrations of 93.2±32.4 ng/ml30.
Although it seems reasonable to use faster and more powerful supplements to achieve sufficient concentrations of vitamin D, it is advisable to carefully consider the dose and frequency of administration.
At the moment, it is not known what is the optimal vitamin D threshold that we must achieve in the prevention or treatment against COVID-19 to reach the objective, as well as the doses that should be used. In a study carried out in China with a small sample size (62 cases and 80 controls), this threshold was set at 16.5 ng/ml31. It seems reasonable to achieve levels above 20 ng/ml and preferably above 30 ng/ml.
In conclusion, we can say that the evidence to indicate the use of vitamin D in preventing and/or treating COVID-19 is scarce and with numerous limitations, with insufficient clinical information to recommend one or another metabolite.
What is the risk/benefit ratio of its administration?
Pending the publication of clinical trials that confirm or not its usefulness, the risk/benefit ratio could be favorable to the use of vitamin D in compassionate use (off-label) in the prevention and treatment of COVID-19 in patients with risk, in which it might be reasonable to prevent or treat deficiency, given the known beneficial effect on immunity and respiratory infections.
What is the risk/benefit ratio of its administration?
In the SARS-COV-2 infection, various treatments have been used, with a certain biological basis for their possible usefulness, but without supporting evidence. In addition to the effective measures implemented (use of masks, distancing, reduced social contact), it is necessary to find some pharmacological measure that reduces the incidence of infection (prevention) or improves its prognosis (therapy). As mentioned before, a higher frequency of hypovitaminosis D has been found in patients with COVID-19.
This finding has been previously observed also in chronic diseases and in some acute diseases, such as respiratory infections. However, the causality of this association has not been clearly established. In the case of SARS-COV-2 infection, there is a biological plausibility for the possible beneficial effect of vitamin D. However, the available evidence is scarce, although, with its limitations, it tends to show a favorable effect.
When using a drug as “compassionate use” without sufficient clinical evidence, the risk/benefit ratio must be assessed. Thus, the first aspect to consider is security. Vitamin D supplements are safe, with very few cases of toxicity, hypercalcemia being the most serious manifestation. The administration of 10,000 IU/day of cholecalciferol or 4,000 IU/day of calcifediol is considered safe32. A safety threshold for serum levels of 25-hydroxyvitamin D has been established at 80 ng/ml, while clinical manifestations could appear from 100 ng/ml. Lewiecki33, in a recent editorial, comments that vitamin D in the treatment of COVID-19 is not dangerous and probably harmless. The risk/benefit ratio could be favorable to the use of vitamin D in compassionate use, off-label, in the prevention and treatment of COVID-19, pending the publication of clinical trials that confirm or not its usefulness. However, given the known beneficial effect on immunity and respiratory infections, it seems reasonable to prevent or treat the deficit in patients at risk.
Bibliografía
1 Long MD, Sucheston-Campbell LE, Campbell MJ. Vitamin D receptor and RXR receptor in the postgenomic era. J Cell Physiol. 2015;230:758-66. [ Links ]
2 Brown AJ, Dusso A. Vitamin D. Am J Physiol. 1999;277:F157-75. [ Links ]
3 Bouillon R, Marcocci C, Carmelit,, Bikle D, White JH, Dawson-Hughes B, et al. Skeletal and extraskeletal actions of vitamin D: Current evidence and outstanding questions. Endocr Rev. 2019; 40:1109-51. [ Links ]
4 Pascarella G, Strumia A, Piliego C, Bruno F, Del Buono R, Costa F, et al. COVID-19 diagnosis and management: a comprehensive review. J Intern Med. 2020;288:192-206. [ Links ]
5 Bergman P. The link betqeen vitamin D and COVID-19: distinguishing facts from fiction. J Intern Med. 2021;289:131-3. [ Links ]
6 Rhodes JM, Subramanian S, Laird E, Griffin G, Kenny RA. Perspective: Vitamin D deficiency and COVID-19 severity- plausibility linked by latitude, ethnicity, impacts on cytokines, ACE2 and thrombosis. J Intern Med. 2021; 289:97-115. [ Links ]
7 Illie PC, Stefanescu S, Smith L. The role of vitamin D in the prevention of coronavirus disease 2019 infection and mortality. Ag Clin Exp Res. 2020;32: 1195-8. [ Links ]
8 Rhodes J, Dunstan F, Laird E, Subramanian S, Kenny RA. COVID-19 mortality increases with northerly latitude after adjustment for age suggesting a link with ultraviolet and vitamin D. BMJ Nutr Prev Health. 2020;3:118-20. [ Links ]
9 Meltzer DO, Best TJ, Zhang H, Volves T, Arora V, Solway J. Association of vitamin D status and other clinical characteristics with COVID-19 test results. JAMA Netw Open. 2020;3:e2019722. [ Links ]
10 D´Avolio AV, Avataneo A, Manca J, Cusato J, De Nicolo A, Lucchini R, et al. 25-Hydroxyvitamin D concentrations are lower in patients with positive PCR for SARS-Co-V-2. Nutrients. 2020; 12:1359. [ Links ]
11 Carpagnano GE, Di Lecce V, Quaranta VN, Zito A, Buonamico E, Capozza E, et al. Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID-19. J Endocrinol Invest. 2020 Aug 9;1-7. [ Links ]
12 Hernandez JL, Nan D, Fernandez-Ayala M, García-Unzueta M, Hernandez-Hernandez MA, Lopez-Hoyos M, et al. Vitamin D status in hospitalized patients with SARS-CoV-2 infection. J Clin Endocrinol Metab. 2020 Oct 27:dgaa733. [ Links ]
13 Liu N, Sun J, Wang X, Zhang T, Zao M, Li H. Low vitamin D status is associated with coronavirus disease 2019 outcomes. A systematic review and meta-analysis. Int J Inf Dis. 2021;104: 58-64. [ Links ]
14 Pereira M, Damascena AD, Galvao Azevedo LM, Olivera TA, Da Mota Santana J. Vitamin D deficiency aggravates COVID-19: systematic review and meta-analysis. Crit Rev Food Sci Nutr. 2020 Nov 4;1-9. [ Links ]
15 Hastie CE, Pell JP, Sattar N. Vitamin D and COVID-19 infection and mortality in UK biobank. Eur J Nutr. 2020;26:1-4. [ Links ]
16 Le Fevre ML. Screening for vitamin D deficiency in adults: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2015;20: 162:133-40. [ Links ]
17 Bilezikian JP, Bikle D, Hewinson M, Lazaretti-Castro M, Gupta A, Madhavan MV, et al. Vitamin D and COVID-19. Eur J Endocrinol. 2020;183:R133-47. [ Links ]
18 Ali N. Role of vitamin D in preventing of COVID-19 infection, progression and severity. J Infect Public Health. 2020;13:1373-80. [ Links ]
19 Mohan M, Cherlan JJ, Sharma A. Exploring links between vitamin D deficiency and COVID-19. Plos Pathogens. 2020;16:e1008874. [ Links ]
20 Grant WB, Lahore H, McDonnell SL, Baggerly CA, French CB, Aliano JL, et al. Evidence that vitamin D supplementation reduce risk of influenza and COVID-19 infections and deaths. Nutrients. 2020;12:988. [ Links ]
21 Martin Gimenez VM, Inserra F, Tajer CD. Lungs as target of COVID-19 infection: Protective common molecular mechanisms of vitamin D and melatonin as a new potential synergistic treatment. Life Sci. 2020;254:117808. [ Links ]
22 Martineau AR, Jolliffe DA, Hooper R , Greenberg L, Aloia JF, Bergman P, et al. Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. Brit Med J. 2017:356:16583. [ Links ]
23 Fasano A, Cereda E, Barichella M, Cassani E, Ferri V, Zecchinelli AL, et al. COVID-19 in Parkinson´s disease patients living in Lombardy, Italy. Mov Dis. 2020;35:1089-93. [ Links ]
24 Annweiler G, Corvaisier M, Gautier J, Dubée V, Legrand E, Sacco G, et al. Vitamin D supplementation associated to better survival in hospitalized frail elderly COVID-19 patients: The GERIA-COVID quasi-experimental study. Nutrients. 2020; 12:3377. [ Links ]
25 Anneweiller C, Hanotte B, Grandin de L´Eprevier C, Sabatier JM, Lafaie L, Celarier T. Vitamin D and survival in COVID-19 patients: a quasi-experimental study. J Ster Biochem Mol Biol. 2020;204:105771. [ Links ]
26 Tan CW, Ho LP, Kalimuddin S, Zhi Cherng BP, Ean The Y, Yee Thien S, et al. Cohort study to evaluate the effect of vitamin D, magnesium and vitamin B12 in combination on progression to severe outcomes in older patients with coronavirus (COVID-19). Nutrition. 2020;79-80:111017. [ Links ]
27 Cereda E, Bogliolo L, Lobascio F, Barichella M, Zecchinelli AL, Pezzoli G, et al. Vitamin D supplementation and outcomes in coronavirus disease 2019 (COVID-19) patients from the outbreak area of Lombardy, Italy. Nutrition. 2021; 82:111055, [ Links ]
28 Entrenas Castillo M, Entrenas Costa L, Vaquero Barrios JM, Alcala Diaz JF, Lopez Miranda J, Bouillon R, et al. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. J Ster Biochem Mol Biol. 2020;203:105571. [ Links ]
29 Olmos JM, Arnaiz F, Hernández JL, Olmos-Martínez JM, Gonzalez-Macías J. Calcidiol mensual frente a calcifediol quincenal en el tratamiento de pacientes osteoporóticos. Estudio en la vida real. Rev Osteoporos Metab Miner. 2018:10;89-95. [ Links ]
30 Navarro-Valverde C, Sosa M, Alhambra MR, Quesada JM. Vitamin D3 and calcidiol are not equipotent. J Ster Biochem Mol Biol. 2016;164:205-8. [ Links ]
31 Ye K, Tang F, Liao X, Shaw BA, Deng M, Huang G, et al. Does serum vitamin D level affect COVID-19 infection and its severity? A case-control study. J Am Coll Nutr. 2020;13:1-8. [ Links ]
32 Bischoff-Ferrari HA, Shao A, Dawson-Hughes B, Hathcock J, Giovannucci E, Willett WC. Benefit-risk assessment of vitamin D supplementation. Osteoporos Int. 2010;21:1121-32. [ Links ]
33 Lewiecki M. Vitamin D and COVID-19: Is something better than nothing? Osteoporos Sarcopenia. 2020;6:95-6. [ Links ]
 Este es un artículo publicado en acceso (Open Access) abierto bajo la licencia Creative Commons Attribution Non-Commercial, que permite su uso, distribución y reproducción en cualquier medio, sin restricciones siempre que sin fines comerciales y que el trabajo original sea debidamente citado.
Este es un artículo publicado en acceso (Open Access) abierto bajo la licencia Creative Commons Attribution Non-Commercial, que permite su uso, distribución y reproducción en cualquier medio, sin restricciones siempre que sin fines comerciales y que el trabajo original sea debidamente citado.
