










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista de Osteoporosis y Metabolismo Mineral
versión On-line ISSN 2173-2345versión impresa ISSN 1889-836X
Rev Osteoporos Metab Miner vol.15 no.4 Madrid oct./dic. 2023 Epub 19-Feb-2024
https://dx.doi.org/10.20960/revosteoporosmetabminer.00018
ORIGINAL
Impact of fragility fractures in postmenopausal Spanish women with osteoporosis
1Servicio de Traumatología. Hospital Alto Deba. Gipuzkoa
2Servicio de Traumatología. Hospital Clínico Universitario de Santiago. Santiago de Compostela, A Coruña
3Servicio de Medicina Interna. Hospital Universitario Virgen de la Macarena. Sevilla
4Sección de Medicina Interna. Hospital Central Universitario Cruz Roja “San José y Santa Adela”. Madrid
5>Servicio de Reumatología. Hospital Clínic de Barcelona. Barcelona
6Servicio de Geriatría. Hospital Universitario de Guadalajara. Guadalajara
7Servicio de Geriatría. Badalona Serveis Assistencials. Badalona, Barcelona
8Servicio de Reumatología. Hospital Universitario de Gran Canaria Doctor Negrín. Gran Canaria
9Servicio de Traumatología. Hospital Regional Universitario de Málaga. Málaga
10Servicio de Endocrinología. Hospital Universitario Quirón de Madrid. Madrid
11Departamento de Economía Aplicada, Estructura e Historia. Facultad de Ciencias Económicas y Empresariales. Universidad Complutense de Madrid. Madrid
12Asociación Española con la Osteoporosis y la Artrosis (AECOSAR)
15Outcomes'10, S.L.U. Castellón de la Plana
Objective:
given the impact of fragility fractures and their consequences on the lives of women with postmenopausal osteoporosis (PMO), the objective of this study is to describe and analyze the impact of this kind of fractures on this population.
Materials and methods:
a survey was conducted among postmenopausal women with fragility fractures in a cross-sectional observational design. Sociodemographic variables, fracture impact (need for care, work productivity), and data on health-related quality of life (HRQoL, assessed using the QUALEFFO-31 questionnaire), and willingness to pay (WTP) to regain HRQoL were collected.
Results:
a total of 120 women participated, with a mean age of 62 ± 7 years. The most frequent fractures described were distal radius fractures (29.9 %), followed by vertebral fractures (21.3 %). A total of 53.3 % required care during their recovery (76.5 %, informal; 24.9 %, formal), and 4.2 % had to be admitted to a health care or nursing home. Among those who were working when the fracture occurred (62.5 %), 56 % had their working life affected (69.3 %, temporary disability; 17.3 %, permanent disability; 10.7 %, reduced working hours; 10.7 %, quit their jobs; 5.3 %, leave of absence; and 3.6 %, early retirement). The impact of the fracture was primarily due to pain (71.7 %), difficulty performing activities of daily living (48.3 %), mobility problems (46.7 %), and emotional state (41.7 %). The highest WTP was offered to regain the ability to perform activities of daily living and improve the emotional state. The overall QUALEFFO-31 score (0-100) was 49.9 ± 10.8 (mental function, 68.3 ± 7.3; pain, 56 ± 22.6; physical function, 39.3 ± 15.5).
Conclusions:
fragility fractures play a significant role on the quality of life of women with PMO. It is of paramount importance to value the aspects that concern them the most to optimize their management.
Keywords: Fragility fracture; Postmenopausal osteoporosis; Quality of life; Disease burden; Willingness to pay; Intangible costs
INTRODUCTION
Back in 2017, a total of 327 600 fragility fractures occurred in Spain, 260 000 of them in women (1). Fragility fractures are defined as those due to low-impact events, such as falling from a standing height, and are the main consequence of osteoporosis, a disease affecting 22.5 % of Spanish women older than 50 (2), a percentage that goes up to 40 % in women aged 70 to 80 years (3).
The risk of experiencing this type of fracture after menopause ranges from 39 % to 53 % (4). Fragility fractures lead to over-use of health care resources because, in some cases, they require hospitalization, and their complications can increase the overall risk of mortality (5-7). Therefore, according to some estimates, they represent the 4th chronic disease causing the greatest impact (disability-adjusted life years), followed by ischemic heart disease, dementia, and lung cancer, thus leading chronic obstructive pulmonary disease (COPD), stroke, and rheumatoid arthritis (1,8). Also, an initial fracture increases the risk of further short-term fractures (1 year) by up to 5 times (9) and can trigger a cycle of health care dependence, increased cost for the health care system, and a worse health-related quality of life (HRQoL) (1). Still, it is estimated that approximately 3 out of every 4 patients do not receive treatment to prevent new fragility fractures (1,2).
The risk of suffering a new fragility fracture is significantly stressful for individuals affected by it. Among the main concerns are the fear of falling and fracturing, the inability to perform household tasks properly, or groom themselves without assistance, or the uncertainty surrounding the future (10-12). Long-term loss of independence is another major concern, especially in the case of hip fractures sustained at advanced ages (13,14).
The present study is based on a survey targeting Spanish women with PMO who sustained a fragility fracture in the past in an effort to provide information on its impact on activities of daily living. Specifically, we intend to describe a) sociodemographic and clinical aspects of women with PMO and fractures; b) dependence and time spent on care; c) work impact; d) the effect of fractures in different areas of life; e) willingness to pay to regain the pre-fracture situation; and f) HRQoL.
MATERIAL AND METHODS
STUDY DESIGN AND PARTICIPANTS
This was an observational cross-sectional study based on an online questionnaire aimed at adult women with PMO who had sustained, at least, 1 OP-related fracture (spontaneous or after a fall) and were Spanish residents (inclusion criteria). Candidates were invited to participate via email (through GfK, Growth from Knowledge), in an online survey designed for this purpose by the research team. Participants agreed to collaborate voluntarily without receiving any financial compensation from the study sponsor, or research team.
Based on the number of women older than 50 years in Spain (n = 10,184,457) (15), the prevalence of osteoporosis in this group (2), and the risk of fracture (3), the study population was estimated at around 1,221,340. Considering that most responses to the survey would be measured as a proportion, the sample size calculation applied the proportion estimation formula assuming maximum indeterminacy (16), with a 95 % confidence interval and a precision error of 9 %. As a result, a sample size of 120 participants was obtained. The survey was closed when the estimated sample size was reached.
THE QUESTIONNAIRE
The questionnaire was developed specifically for the study. A scientific committee including 10 health care professionals, a health economics specialist, a representative from the Spanish Association for Osteoporosis and Arthritis (AECOSAR), and an expert female patient, reviewed the questionnaire to determine the appropriateness of the questions and their comprehensibility. The study was evaluated and approved by the Drug Research Ethics Committee (DREC) of Hospital Universitario Puerta de Hierro Majadahonda (Madrid, Spain).
The questionnaire included a total of 33 questions distributed across 6 sections (supplementary data): a) sociodemographic variables (age, autonomous community of residence, family situation/living arrangements, membership in any OP-related patient association); b) clinical data (age at menopause, location, number, and year of fragility fractures, most affected fracture, comorbidities); c) caregiver-related data (after the fracture: need for admission to recovery centers and duration, need for a caregiver, hours/week of caregiver dedication); d) productivity-related data (current employment status, employment status before the fracture, impact of the fracture on work activity); e) impact of the fracture on activities of daily living (compared to the situation prior to the fracture: impact on activities of daily living, mobility, pain, leisure activities, family relationships, intimate life, and psychological/emotional well-being); and f) data related to willingness to pay (participants' willingness to pay to return to the pre-fracture state for each of the affected areas. Response ranges: < € 500, € 501-€ 1000, € 1001-€ 1500, € 1501-€ 2000, € 2001-€ 2500, € 2501-€ 3000, > € 3000). At the end of the survey, the specific QUALEFFO-31 questionnaire (17), validated in Spanish (18), was included to assess quality of life in women with osteoporosis. This questionnaire is divided into 3 different domains: pain, physical function, and mental function, with a total of 100 points possible in each domain and overall, indicating the highest scores a worse quality of life.
STATISTICAL ANALYSIS
Data analysis was conducted using the STATA v.14 statistical software package. For the descriptive analysis of the sample, relative and absolute frequencies were calculated for qualitative variables, while central tendency and dispersion statistics (mean, standard deviation [SD], minimum, maximum, and quartiles) were calculated for quantitative variables. To estimate the mean willingness to pay to improve several aspects of quality of life, only the responses of patients who had an impact in each area were considered. To do this, responses on monetary ranges were replaced by the midpoint of the interval, and a 50 % correction was applied (improvement for other reasons).
RESULTS
SOCIODEMOGRAPHIC CHARACTERISTICS
The study included a total of 120 participants, all of whom were women with PMO with > 1 previous fragility fractures. The patients' mean age was 62 years (SD, 7.1; range, 49-84). Participants were recruited from 16 Spanish autonomous communities, with the following distribution: Valencian Community (24.2 %), Canary Islands (16.6 %), Extremadura (11.6 %), Andalusia (10.8 %), Aragon (5.8 %), Balearic Islands (5 %), Asturias (4.2 %), Madrid (4.2 %), Murcia (2.5 %), Basque Country (2.5 %), La Rioja (2.5 %), Navarra (2.5 %), Castilla-La Mancha (2.5 %), Galicia (1.6 %), Cataluña (1.6 %), Castilla y León (1.6 %). A total of 74 % of participants (n = 89) were living with someone else, while the remaining 26 % (n = 31) lived alone. Most participants (97.5 %, n = 117) were not members of any patient association related to OP.
CLINICAL DATA
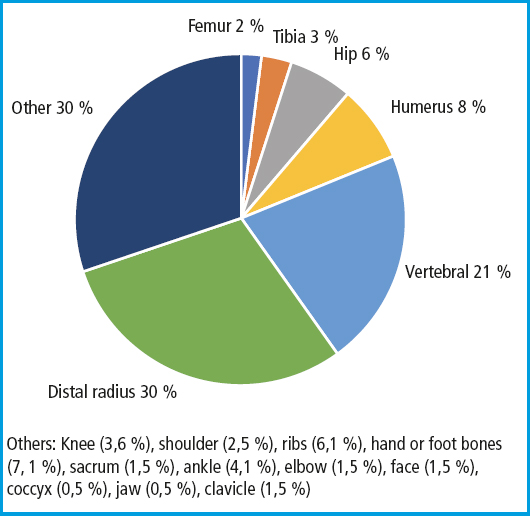
Menopause mean age was 49 years (SD, 5.2; range, 34-65). The mean number of fragility fractures sustained by the participants was 1.6 (SD, 1.2; range, 1-8), with 36.7 % of them having sustained 2 or more fractures. Among the different types of fractures reported in the survey, the most common ones were distal radius fractures (29.9 %), followed by vertebral fractures (21.3 %), proximal humerus fractures (7.6 %), and hip fractures (6.1 %) (Fig. 1). Accordingly, the type of fracture that had impacted the participants' activities of daily living more significantly was distal radius fractures (32 %), followed by vertebral fractures (18 %), proximal humerus fractures (11 %), and hip fractures (7 %). The mean time elapsed since the first fracture occurred was 7.5 years (SD, 5.8), and 5.5 years (SD, 3.1) since the last one.
In addition to osteoporosis, the most common conditions described among the participants were vision problems (20.8 %) and thyroid gland disorders (20.8 %), followed by early menopause, periods of amenorrhea, and ovariectomy (16.7 %), rheumatoid arthritis (15.8 %), osteoarthritis (14.1 %), COPD (10.8 %), and breast cancer (10 %). Diabetes, cardiopulmonary disease, and balance disorders were present in 6.7 % of the cases. Chronic kidney disease (3.3 %), peripheral neuropathy (1.7 %), and, with only 1 case (0.8 %), celiac disease, cerebrovascular disease, Parkinson's disease, and inflammatory bowel disease were among the least common diagnoses of all. Nearly 22.5 % of the patients said they had not been diagnosed of any other diseases and conditions.
IMPACT OF FRACTURES ON THE ACTIVITIES OF DAILY LIVING
Overall, pain was the most common symptom (71.7 %) experienced after the fracture, followed, in almost half of the cases, by difficulties performing activities of daily living (dressing, showering, cleaning, shopping, etc.), and mobility problems (walking or moving inside or outside the house, getting up, bending down or kneeling, using public transportation, etc.), compared to the situation prior to the fracture (Fig. 2A). The same trend was seen when only women who had sustained vertebral fractures were considered (the second most common type of fracture), although in this case, pain affected more than 90 % of the patients. In the case of distal radius fractures (the most common fracture), pain and difficulty performing activities of daily living were also among the most common symptoms of all (55.2 % and 31.5 %), followed, in this case, by an impact on leisure activities (28.9 %).
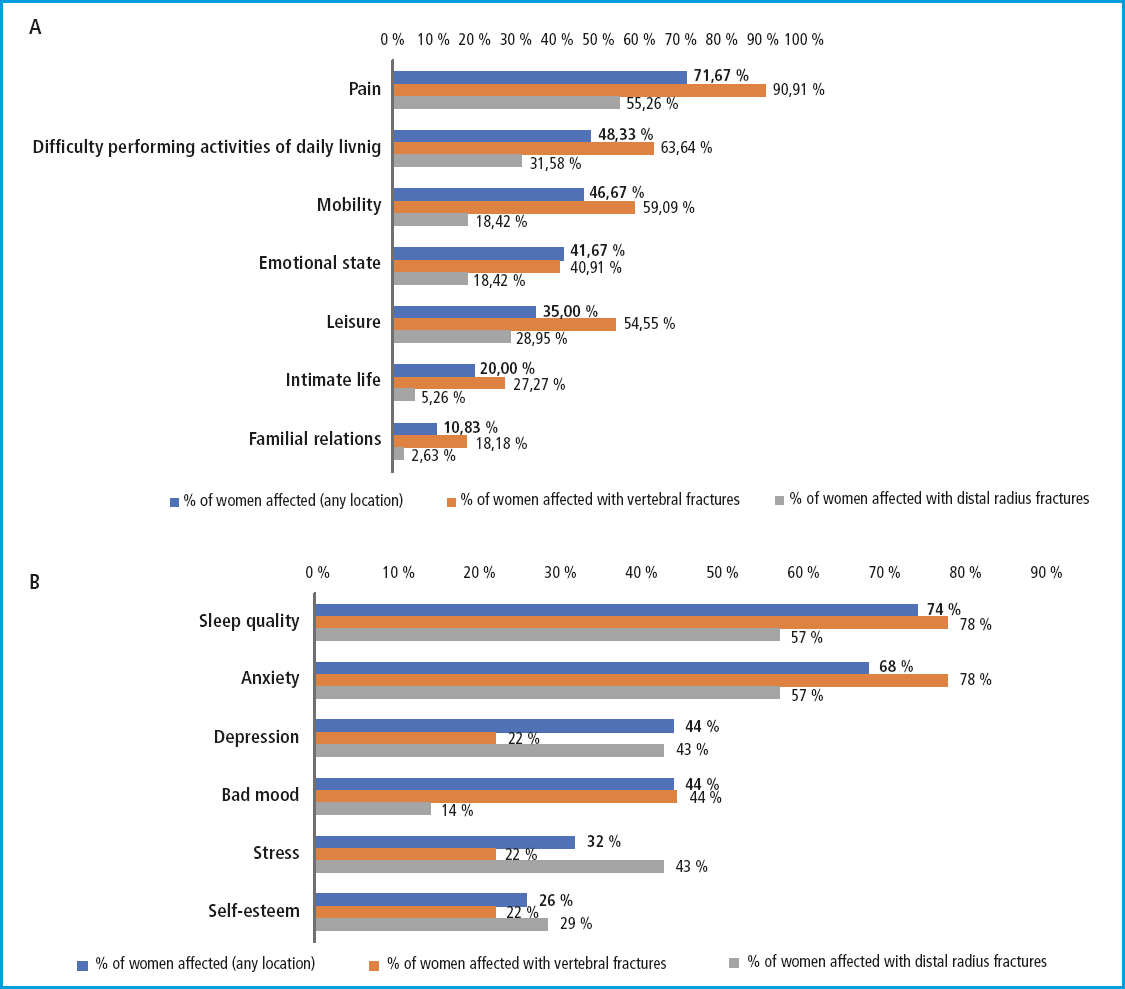
A total of 41.61 % of the patients (n = 50) reported that fractures had an impact on their emotional life. In the case of women who said that distal radius fractures and vertebral fractures had been the ones that had impacted the activities of daily living more significantly, the percentage with emotional impact was 18.4 % (n = 7) and 40.9 % (n = 9), respectively. Overall, most of them had experienced loss of sleep quality and anxiety. Depression, mood swings, stress, and low self-esteem were among the symptoms also reported by the patients (Fig. 2B).
QUALITY OF LIFE QUESTIONNAIRE
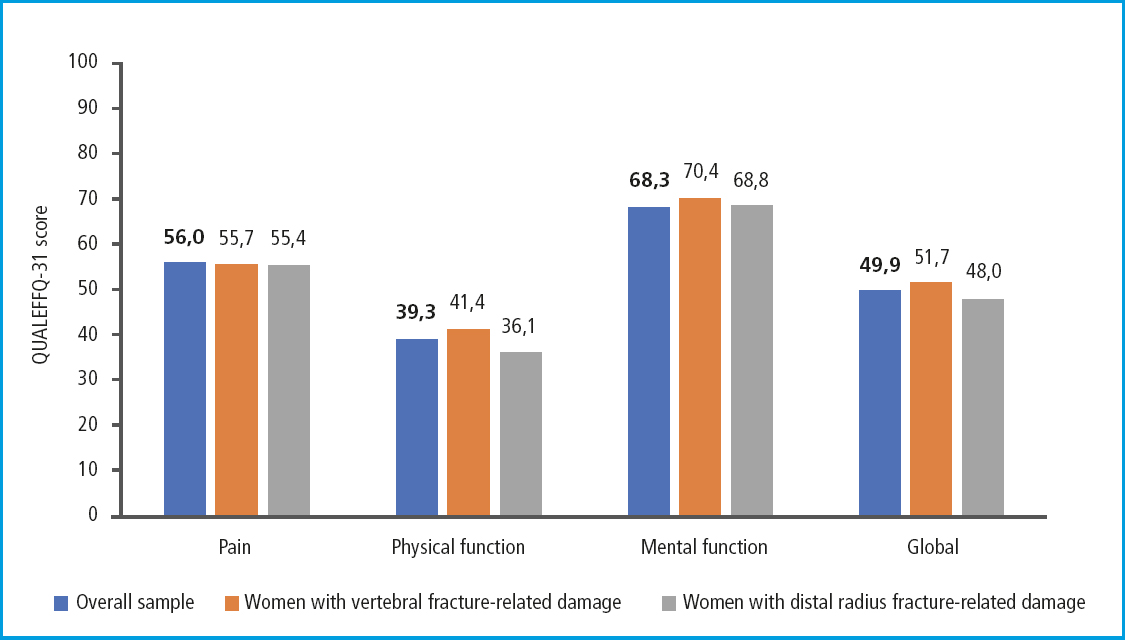
The mean overall score on the QUALEFFO-31 was 49.9 (SD, 10.8; range 33.5-83.2). Figure 3 illustrates the mean overall score, as well as the specific scores for the questionnaire domains for all participants and those with the most common fractures of all (distal radius and vertebral fractures). Overall, a poorer quality of life was seen in the mental function domain (mean, 68.3; SD, 7.3; range, 51.1-84.4), followed by pain (mean, 56; SD, 22.6; range, 20-100) and physical function (mean, 39.9; SD, 15.5; range, 18.9-94.4). The same trend was seen in women who said that distal radius and vertebral fractures were the ones that had the most significant impact on their activities of daily living.
CAREGIVER-RELATED DATA
At the time of the survey, most participants (79.1 %) did not have a caregiver. As a matter of fact, 4.2 % of them were in charge of the personal care of another patient. Nearly 15.8 % received care from a family member, and only 1 case (0.8 %) from a professional caregiver.
After sustaining a fragility fracture, 64 of respondents (53.3 %) required professional or family caregiver assistance during their recovery. Among them, 9 patients (14.0 %) had to pay for the caregiver (themselves or their families), 7 (10.9 %) had a home caregiving service provided by the health care system, and 49 (76.5 %) received non-professional care. Additionally, 5 participants (4.1 %) had to be admitted to a center or nursing home for their recovery, with a mean length of stay of 2.8 months (SD, 4).
The mean duration of the care and assistance provided by the caregivers was 8.8 months (SD, 17.7); for private assistance, 19 months (SD, 28.1); for health care assistance, 7.2 months (SD, 13.4); for non-professional care, a mean weekly caregiving time of 30.4 hours (SD, 52.8), 5.8 hours (SD, 6.9), and 21.3 hours (SD, 28.4), respectively.
WORK PRODUCTIVITY-RELATED DATA
A total of 62.5 % (n = 75) of the participants were actively employed at the time of the fracture. Among the working participants, 74.6 % (n = 56) reported that the fracture had affected their work life. Among them, 69.6 % had applied for temporary disability (with a mean duration of 120 days; SD, 117.6). Additionally, 17.8 % had to apply for permanent disability after a mean 23.1 months (SD, 28.4) following the fracture. Nearly 10.7 % had to reduce their working hours (averaging 4.4 hours per day; SD, 2.3 or 336 days on average; SD, 163.4), 10.7 % had to stop working or lost their jobs, 5.3 % had to take days off or leaves of absence (averaging 61.6 days; SD, 57.5), and 3.6 % had to take early retirement after a mean 13.5 months since the fracture occurred (SD, 14.8).
WILLINGNESS TO PAY-RELATED DATA
When participants were asked how much they would be willing to pay to regain their pre-fracture state in different aspects of their daily life, within specified ranges, the highest willingness to pay was observed for the ability to perform activities of daily living and emotional well-being. On the other hand, the lowest willingness to pay was reported for the work situation and family relationships (Table I).

DISCUSSION
This observational study provides valuable information to understand the impact of fragility fractures on the quality of life of women with PMO. Additionally, it provides novel data to assess the intangible burden and costs associated with this disease.
The survey results reveal the participation of relatively young women (mean age, 62 years), compared to the population typically observed in the routine clinical practice, where the mean age of women with PMO who have experienced fractures is closer to 75 years (19,20). However, these women had already experienced a mean of 1.6 fragility fractures. This mean age is also consistent with former studies (63 to 65 years) based on surveys targeting women with similar characteristics to assess HRQoL (21,22). The participants' age could explain the percentage and location of the fractures reported, being wrist fractures the most common and hip fractures the less common of all (1). This is likely due to the fact that the incidence of hip fractures increases exponentially with age, ranging from 7 % in women aged 55 to 59 years up to 34 % in those older than 85 years (23).
Fragility fractures not only had a physical impact but also an emotional one. Pain and psychological well-being are 2 dimensions of HRQoL significantly affected, according to the results, which prompts consideration of the appropriate management of the disease. Former studies have identified pain as one of the most affected domains in women with PMO who have sustained fractures (21,24). Additionally, vertebral fractures can cause long-term pain, with some women still experiencing it several years after having sustained their fracture (25). The results of the QUALEFFO-31 questionnaire show a greater dispersion in this area, with some women reaching the maximum possible score (100 points, which is indicative of a worse quality of life). This questionnaire was previously used in a study of Spanish women with PMO (mean age, 59 years) where fragility fractures were not considered (18). Therefore, the scores in all domains were likely lower than those obtained in the present study, being pain the least affected dimension (physical function, 21.6; mental function, 19.8; pain: 10.8) (18). The impact of pain and physical impairment is evident in women who have sustained fragility fractures. However, the mental function domain was the one where the worst quality of life was reported. Consistent with former studies conducted among postmenopausal women with osteoporosis (26), anxiety emerges as a prominent sign of emotional distress. The fear of sustaining yet another bone fracture is one of the main concerns of women who have previously sustained a fragility fracture (27). In this regard, secondary prevention plays a key role where there is large room for improvement, because most individuals with fragility fractures are not assessed or treated to reduce the risk of a second fracture (28,29). Regarding treatment, it has been estimated that only 28 % of Spanish women receive treatment to prevent fractures in the year following the index fracture (2). Also, treatment compliance is not even close to 35 % (30).
The degree of interdependence of individuals who suffer fragility fractures can vary depending on their age and type of fracture sustained. This variation is particularly evident considering that distal radius fractures typically occur around the age of 60, vertebral fractures around the age of 70, and hip fractures around the age of 80. Particularly the latter often require hospitalization and more extensive care (2). We should mention that because of the mean age of the study participants (62 years), hip fractures were underrepresented, and possibly because of this, at the time of the survey (a mean 5.5 years after sustaining the last fracture), most participants did not require a caregiver. However, more than half of them reported needing care during their recovery from the fracture, despite being relatively young women. This is a remarkable finding because it means that regardless of the location where fractures occur, they can lead to a significant degree of interdependence due to limited activities of daily living. Additionally, most care was provided by unpaid caregivers. The informal care required by women with PMO after sustaining a fragility fracture is one of the hidden burdens of these fractures impacting society (1), which is also evident in our study.
The loss of labor productivity is another social burden associated with fragility fractures that was also explored in the survey. Although these fractures primarily affect elderly individuals, around 20 % of them occur prior to retirement age (31). In our study, more than half of the participants sustained a fragility fracture while still actively working, and the data they provided is particularly valuable to estimate the indirect costs associated with the disease.
We should mention how important functionality was for the study participants, despite having sustained mostly fractures with less associated disability than hip fractures (2). In a hypothetical scenario where those affected could pay to regain their pre-fracture condition, they would pay the highest amount of money to regain their ability to perform activities of daily living. Once again, pain and the emotional state were among the aspects that patients assigned the highest value to. These results are fundamentally relevant to understand which aspects of the lives of women' who sustain fragility fractures are most important to them. Since participants had closed response ranges, the economic value per se should be assessed with caution. However, it can help estimate the intangible cost of the disease conservatively. The WTP to regain different aspects of daily living will depend on the condition under consideration, its consequences, and the characteristics of the individuals sustaining the fracture. Therefore, in a former study of patients with psoriasis where the same response ranges were used, the highest value was assigned to regain the ability to work (€ 843) and family life (€ 843), while the WTP to go back to performing activities of daily living was the lowest of all (€ 535) (30).
The survey has several limitations inherent to its design and the study population. The use of ad-hoc questions in the questionnaire can be a limitation too. Regarding the study population, we should mention that patients belonged to a panel of participants from a company specialized in conducting opinion and market research studies through digital media. Therefore, characteristics such as the mean age and, consequently, the type of fractures sustained may not be representative of the overall population with PMO, as previously mentioned. The impact of fractures may have been underestimated (greater if more hip fractures would have been collected), while the labor impact may have been overestimated (lower if fractures would have occurred after retirement). The participants' high comorbidity could also be partly attributed to the panel's characteristics (women motivated to answer questions on their health status). On the other hand, autonomous communities with large populations, such as Catalonia, Andalusia, and Madrid, were underrepresented. Another limitation associated with the type of study is that data are not supported by any particular physician or health record, which could have led to overestimating some fragility fractures, such as metatarsal fractures, which could have occurred due to causes unrelated to PMO, in addition to the fractures classified as “other” (where the exact location of those classified as femur is also unknown). Additionally, no questions were asked on whether vertebral fractures were clinical or only morphometric, although it is assumed that they were clinical due to the high percentage of individuals who sustained fractures and reported experiencing pain. Finally, the years passed since the last fracture occurred (mean, 5.5 years) could have affected the patients' subjective recall of the most immediate impact of the fracture. Despite these limitations, all the questions in the questionnaire were associated with osteoporosis and its consequences (including a specific HRQoL questionnaire). Also, the data provided are highly valuable when it comes to understanding aspects of daily living most generally affected after sustaining fragility fractures.
This study highlights the significant impact that fragility fractures have on the lives of women with PMO, where pain, the ability to perform activities of daily living, independence, and emotional state are primarily affected. Recognizing the aspects that are more concerning for patients is essential to prevent and optimize the management of fragility fractures. Due to its impact on HRQoL, we should focus our efforts on optimizing the management of PMO, secondary prevention, reducing the risk of sustaining new fractures, and avoiding their consequences.
CONFLICTS OF INTEREST
IE has received fees for presentations and consultancy jobs done for UCB, Amgen, Lilly, Theramex, Grunenthal, and Italfármaco. JRC has received fees as a consultant and/or speaker from Amgen, Gebro, Gedeon-Richter, Grünenthal, Lilly, MSD, UCB, Synthex (J&J), Stryker, and Theramex. FJO and TP declared no conflicts of interest whatsoever. MJM-A has received lecture fees, travel grants, and advisory fees from Stada, Amgen, UCB, Grünenthal, Gedeon Richter, and Rubió. PP has received speaking fees from Amgen, UCB, Lilly, and Kyowa Kirin Farmacéutica. AN has received fees for presentation jobs done for UCB, Amgen, Galapagos, Abbvie, and Lilly; consultancy fees from Abbvie and UCB; and for attending conferences on behalf of UCB, Amgen, Pfizer, and Abbvie. VPdR has received fees from Amgen, UCB, Stada, and Grünenthal. EJ has received consultancy fees from Amgen, AstraZeneca, FAES, Helios-Fresenius, Italfármaco, Lilly, MSD, Mundipharma, Novo Nordisk, UCB, and Viatris; as a clinical researcher, he has received fees from Amgen, Boehringer, AstraZeneca, FAES, Janssen, Lilly, MSD, Novo Nordisk, Pfizer, Sanofi, Shire, and UCB; and as a speaker he has received fees from Amgen, Asofarma, Astellas, AstraZeneca, Bayer, Boehringuer, BMS, FAES, Lilly, MSD, Mundipharma, Novo Nordisk, Technofarma, UCB, and Viatris. MGG has received presentation and consultancy fees from UCB, consultancy fees from Astellas, Vifor, Angelini, and Janssen, and through a competitive grant from MSD. JV declares that UCB and AMGEN collaborate in supporting AECOSAR patient educational programs, an association I am the president of. SM is an employee of UCB. ICT is an employee of Amgen. LB-P and SA are both employees of Outcomes'10, an independent research company that has received funding from UCB for coordinating this study.
BIBLIOGRAFÍA/REFERENCES
1. Huesos rotos, vidas rotas:guía para mejorar la atención a las fracturas por fragilidad en España. Available from:http://share.iofbonehealth.org/EU-6-Material/Reports/IOF Report_SPAIN_DIGITAL_SP.pdf [ Links ]
2. Borgström F, Karlsson L, Ortsäter G, Norton N, Halbout P, Cooper C, et al. Fragility fractures in Europe:burden, management and opportunities. Archives of Osteoporosis 2020;15:59. DOI:10.1007/s11657-020-0706-y [ Links ]
3. Díaz Curiel M, García JJ, Carrasco JL. Prevalencia de osteoporosis determinada por densitometría en la población femenina española [Med Clin(Barc).2001]-Medes. Medicina Clínica 2001;116(3):86-8. DOI:10.1016/S0025-7753(01)71732-0 [ Links ]
4. Díaz Curiel M. Osteoporosis:concepto. Fisiopatología. Clínica. Epidemiología. Revista de Osteoporosis y Metabolismo Mineral 2018;10(Supl 1):52-4. [ Links ]
5. Bouza C, López T, Palma M, Amate JM. Hospitalised osteoporotic vertebral fractures in Spain:Analysis of the national hospital discharge registry. Osteoporosis International 2007;18(5):649-57. [ Links ]
6. Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporosis International 2006;17(12):1726-33. DOI:10.1007/s00198-006-0292-x [ Links ]
7. Grupo de Trabajo de Enfermedades Reumatológicas de la sem FYC. Osteoporosis. Manejo:prevención, diagnóstico y tratamiento (PDF) - semFYC 2014. Available from:https://www.semfyc.es/formacion-y-recursos/osteoporosis-manejo-prevencion-diagnostico-y-tratamiento-pdf/ [ Links ]
8. Hernlund E, Svedbom A, Ivergård M, Compston J, Cooper C, Stenmark J, et al. Osteoporosis in the European Union:medical management, epidemiology and economic burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch Osteoporos 2013;8(1):136. DOI:10.1007/s11657-013-0136-1 [ Links ]
9. Geel TA, van Helden S, Geusens PP, Winkens B, Dinant GJ. Clinical subsequent fractures cluster in time after first fractures. Ann Rheum Dis 2009;68(1):99-102. DOI:10.1136/ard.2008.092775 [ Links ]
10. Lizán Tudela L, Badía Llach X. La evaluación de la calidad de vida en la osteoporosis. Atención Primaria 2003;31(2):126-33. DOI:10.1016/S0212-6567(03)79150-1 [ Links ]
11. Kerr C, Bottomley C, Shingler S, Giangregorio L, de Freitas HM, Patel C, et al. The importance of physical function to people with osteoporosis. Osteoporosis International 2017;28(5):1597-607. DOI:10.1007/s00198-017-3911-9 [ Links ]
12. Jakobsen PR, Hermann AP, Søndergaard J, Wiil UK, Dixon RF, Clemensen J. Left in limbo –Experiences and needs among postmenopausal women newly diagnosed with osteoporosis without preceding osteoporotic fractures:A qualitative study. Post Reproductive Health 2018;24(1):26-33. DOI:10.1007/s00198-017-3911-9 [ Links ]
13. Hallberg I, Rosenqvist AM, Kartous L, Löfman O, Wahlström O, Toss G. Health-related quality of life after osteoporotic fractures. Osteoporos Int 2004;15(10):834-41. DOI:10.1007/s00198-004-1622-5 [ Links ]
14. Cooper C. The crippling consequences of fractures and their impact on quality of life. Am J Med 1997;103(2a):12S-7S;discussion 7S-9S. DOI:10.1016/S0002-9343(97)90022-X [ Links ]
15. Instituto Nacional de E. Cifras de población a 1 de julio de 2019. [ Links ]
16. Marrugat J, Vila J, Pavesi M, Sanz F. Estimación del tamaño de la muestra en la investigación clínica y epidemiológica. Med Clin (Barc) 1998;111(7):267-76. [ Links ]
17. van Schoor NM, Knol DL Fau - Glas CAW, Glas Ca Fau - Ostelo RWJG, Ostelo Rw Fau - Leplège A, Leplège A Fau - Cooper C, Cooper C Fau - Johnell O, et al. Development of the Qualeffo-31, an osteoporosis-specific quality-of-life questionnaire. Osteoporosis International 2006;17(4):543-51. DOI:10.1007/s00198-005-0024-7 [ Links ]
18. González Matarín PJ, Martínez-Amat A, Lomas-Vega R, De Guevara NML, Díaz-Mohedo E, Martínez López E, et al. Validation of the quality of life questionnaire of the European foundation for osteoporosis-31 in Spanish postmenopausal women. Menopause 2014;21(5):469-76. DOI:10.1097/GME.0b013e3182a6cc64 [ Links ]
19. Sosa Henríquez M, Canario GdTeO. Las mujeres osteoporóticas con fracturas muestran mayor cumplimiento terapéutico que las no fracturadas. Rev Osteoporos Metab Miner 2014;6(1):8-13. DOI:10.1097/GME.0b013e3182a6cc64 [ Links ]
20. Aguilar del Rey FJ, Pérez-González O. Epidemiología de las fracturas osteoporóticas en Andalucía en el período 2000-2010. Medicina Clínica 2018;150(8):297-302. DOI:10.1016/j.medcli.2017.06.070 [ Links ]
21. Ciubean AD, Ungur RA, Irsay L, Ciortea VM, Borda IM, Onac I, et al. Health-related quality of life in Romanian postmenopausal women with osteoporosis and fragility fractures. Clin Interv Aging 2018;13:2465-72. DOI:10.1016/j.medcli.2017.06.070 [ Links ]
22. Palacios S, Neyro JL, Fernández de Cabo S, Chaves J, Rejas J. Impact of osteoporosis and bone fracture on health-related quality of life in postmenopausal women. Climacteric 2014;17(1):60-70. DOI:10.3109/13697137.2013.808182 [ Links ]
23. Pfeilschifter J, Cooper C, Watts NB, Flahive J, Saag KG, Adachi JD, et al. Regional and age-related variations in the proportions of hip fractures and major fractures among postmenopausal women:the Global Longitudinal Study of Osteoporosis in Women. Osteoporos Int 2012;23(8):2179-88. DOI:10.1007/s00198-011-1840-6 [ Links ]
24. Bączyk G, Samborski W, Jaracz K. Evaluation of the quality of life of postmenopausal osteoporotic and osteopenic women with or without fractures. Arch Med Sci 2016;12(4):819-27. DOI:10.5114/aoms.2015.55012 [ Links ]
25. Hasserius R, Karlsson MK, Jónsson B, Redlund-Johnell I, Johnell O. Long-term morbidity and mortality after a clinically diagnosed vertebral fracture in the elderly - A 12- and 22-year follow-up of 257 patients. Calcif Tissue Int 2005;76(4):235-42. DOI:10.1007/s00223-004-2222-2 [ Links ]
26. Shorey S, Chan V. Women Living With Osteoporosis:A Meta-Synthesis. Gerontologist 2021;61(3):39-47. DOI:10.1093/geront/gnz173 [ Links ]
27. Olsen CF, Bergland A. The effect of exercise and education on fear of falling in elderly women with osteoporosis and a history of vertebral fracture:results of a randomized controlled trial. Osteoporos Int 2014;25(8):2017-25. DOI:10.1007/s00198-014-2724-3 [ Links ]
28. Dreinhöfer KE, Mitchell PJ, BéguéT, Cooper C, Costa ML, Falaschi P, et al. A global call to action to improve the care of people with fragility fractures. Injury 2018;49(8):1393-7. DOI:10.1016/j.injury.2018.06.032 [ Links ]
29. Akesson K, Marsh D, Mitchell PJ, McLellan AR, Stenmark J, Pierroz DD, et al. Capture the Fracture:a Best Practice Framework and global campaign to break the fragility fracture cycle. Osteoporos Int 2013;24(8):2135-52. DOI:10.1007/s00198-013-2348-z [ Links ]
30. Wu CH, Tu ST, Chang YF, Chan DC, Chien JT, Lin CH, et al. Fracture liaison services improve outcomes of patients with osteoporosis-related fractures:A systematic literature review and meta-analysis. Bone 2018;111:92-100. DOI:10.1016/j.bone.2018.03.018 [ Links ]
31. Kanis JA, Johnell O, Oden A, Sembo I, Redlund-Johnell I, Dawson A, et al. Long-term risk of osteoporotic fracture in Malmö. Osteoporos Int 2000;11(8):669-74. DOI:10.1007/s001980070064 [ Links ]
Received: June 01, 2023; Accepted: September 26, 2023
 This is an open-access article distributed under the terms of the Creative Commons Attribution License
This is an open-access article distributed under the terms of the Creative Commons Attribution License
