










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
Permalink
Key messages
This systematic review showed that although interventions had educational components, it was not ascertained the knowledge acquired through the intervention. Therefore, it should be assessed considering the education levels of parents.
Studies included showed it is challenging to increase the consumption of recommended food groups, thus, new interventions should be considered to reach this objective.
Interventions seemed more effective as treatment than prevention for overweight or obesity in preschoolers.
4. Telephony was the most used technological tool for two main components of the interventions: motivational interviewing and coaching. Whereas direct contact was the most used traditional approach.
INTRODUCTION
The World Health Organization (WHO) estimated that factors related to nutrition influence 45% of deaths in children under five years old1. Child malnutrition has increased worldwide, for children under five years, stunting affects 149.2 (22.0%) million, wasting 45.4 (6.7%) million and overweight 38.9 (5.7%) million. In addition, the impact on lifestyles due to COVID-19 could increase all forms of malnutrition2.
Consuming a healthy diet early in life helps to prevent malnutrition in all its forms, it is important to ensure an adequate growth and development, moreover, reduce the risk of developing noncommunicable diseases (NCDs)3,4.
Eearly years of life are critical periods to develop a healthy lifestyle, therefore, eating behaviours must be taught in early childhood5,6. After the first three years of life, brain development is able to build the learning networks, thus, in the previous years it acquired the necessary elasticity where the nerve cells multiply rapidly, forming the structures that allow the learning process7. All this development and grow process needs a good font of good energy in order to succeed. Nevertheless, there are many factors that could influence this critical stage in preschoolers, such as access for parents to nutritional education8. What can influence the present feeding and the future feeding styles in this stage where they begin to take shape.
An innovative form to address health needs is eHealth, defined as the use of Information and Communication Technologies (ICT) in support of health related fields9. ICT are defined as tools and resources to transmit, store, create or share information, including computers, the Internet (websites, blogs, mails) live broadcasting technologies, recorded broadcasting technologies and telephony10. ICT-based interventions have been previously reviewed for different authors.
A systematic review focused on adolescents, reported effectiveness for increasing the intake of vegetables and decreasing junk food consumption. However, it was recognized that an additional comparison is necessary to identify if ICT are superior or equally effective than traditional programs11. Another systematic review about the effectiveness of technology-based interventions to address obesity in children, showed that video games, web-bases or mobile phone communications with further research have the potential of positive impact on weight-related outcomes12. In addition, for children, previous reviews already focused on interventions to prevent specific forms of malnutrition such as overweight13 and obesity14.
Others interventions evaluated the effectiveness of which ICT interventions improve specific dietary patterns as fruit and vegetables intake15. And more recently, one review evaluated interventions with direct parental involvement16, and just one more evaluated the use of digital tools17. Given its importance for health, it is important to begin to explore the benefits of ICT in preschool children and whether they can affect their future lives.
Although previous interventions, ICT-based or traditional approaches, exist, have not been compared. Specifically, in preschoolers, it is not clear about the benefits of ICT. In effort to address this evidence gap, this systematic review aimed to compare interventions using ICT tools in comparison to traditional approaches, targeting parents to improve healthy diet or BMI in preschoolers. Specifically, to know its effectiveness, which tools have been used and the main success factors in the interventions.
METHODOLOGY
This systematic review was registered on PROSPERO (ID. CRD42021251037) followed the PRISMA 2020 guidelines18, to state the comparisons the Population, Intervention, Comparison and Outcomes (PICO) framework was used as follows. P: preschoolers without diseases or treatments that influence weight or metabolism and their parents. I: interventions to improve a healthy diet or healthy BMI with ICT approach that include preschoolers and their parents. C: interventions with traditional approaches. O: Primary outcomes: “changes in healthy diet or healthy BMI” and “durability of the outcome (follow-up) and Secondary outcomes: “additional positive outcomes reported by the authors or impact between groups, duration or durability of the intervention and follow-up”.
Search criteria
The following databases were used: PubMed, Scopus, Springer Link and Cochrane Library. Terms from the Medical Subject Headings (MeSH) were used as keywords for search strategy, the following syntax was used: “Intervention AND Health Education OR Information Technology AND Healthy Diet AND Body Mass Index AND Parents AND Children Preschool NOT Infants NOT Adolescents”. Search strategy was the same for all the databases, in each one, the necessary filters to meet the inclusion criteria were applied.
Inclusion, exclusion, and elimination criteria
The intervention group to improve healthy diet or BMI had to include one or both parents or guardians and target preschool children (2-5 years according with MeSH). Studies could include other group (teachers, staff or health professionals) as long as in conjunction with parental or guardian participation. The design of studies included were Randomized Controlled Trial (RCT) and systematic reviews. With publication date between 2017 and 2021, in English or Spanish and available in full text or Open Access. Interventions included could be worldwide. Interventions of any category that had ICT educational components or not were included. For this purpose, the ICT United Nations Educational, Scientific, and Cultural Organization (UNESCO) definition, previously mentioned, was used. Whereas traditional approaches were all those tools that are not included in ICT definition. Studies that included multiple ages of children, preschool ages, were excluded. Studies focusing on different populations as well as any variation of the healthy diet (e.g., vegan) were excluded.
Selection process
Reviewers worked independently for the screening process by title and abstract. Duplicate records were removed. Titles and abstracts of articles identified were screened independently for 4 authors, the differences in reviewer selections were resolved by a 3rd reviewers as moderators.
Data extraction
The following items were extracted from the included studies and were tabulated in an Excel table: 1) Identification data, such as the complete reference and the name of the study. 2) Purpose of the study, such as objectives, research question or hypothesis. 3) Methods, such as study design, location, target group, and sample size. 4) Preschooler data, such as age, gender, nationality, race, or ethnicity. 5) Intervention characteristics, such as description, duration, intensity, and follow-up. 6) Main outcomes: changes in healthy diet (CHD) and changes in BMI (CBMI) and use of ICT or other educational components. 7) Secondary outcomes: additional positive outcomes reported by the authors or impact between groups, duration or durability of the intervention and follow-up. For data extraction, reviewers worked independently. In case of missing data or additional details, we would contact the authors, but it was not necessary to do.
Synthesis methods
For the intervention effect, all favorable effects reported for the intervention group (IG) on healthy diet and BMI (e.g., p-value, effect size, odds ratio, standard deviation, confidence interval) were considered. Positive effects (+) refer to all measures of a variable (healthy diet or BMI) in the IG that had a significant difference. Mixed effects (/) means that only some measures in the IG were significant. Negative effects (-) refer to significant differences in the control group (CG). And undefined effects (*) refer to the absence of significant differences in the IG, for all measures of the variables.
Studies were synthesized according to interventional approaches used: 1) education with ICT tools (ICT-T): computers, internet, live broadcasting technologies, recorded broadcasting technologies and telephony, or 2) Interventions using Traditional Approaches (TA): printed materials, direct contacts, and didactic materials. Data were tabulated in an Excel table.
Risk of bias assessment
Methodological rigor was assessed according to the guidelines for assessing the different types of included studies (e.g., PRISMA 2020 checklist, CONSORT 2010 checklist), assigning each item a score, 0 points: totally incomplete; 5 points: partially complete; 10 points: totally complete. Then, the percentage of each study was calculated to define its risk of bias category: (A) low 80 to 100%, (B) medium 50 to 80% (C) high 0 to 50%. Reviewers worked independently.
Ethical considerations
This systematic review is considered without risk. In addition, the ethical standards established for the handling of information were compiled with rigor19.
RESULTS
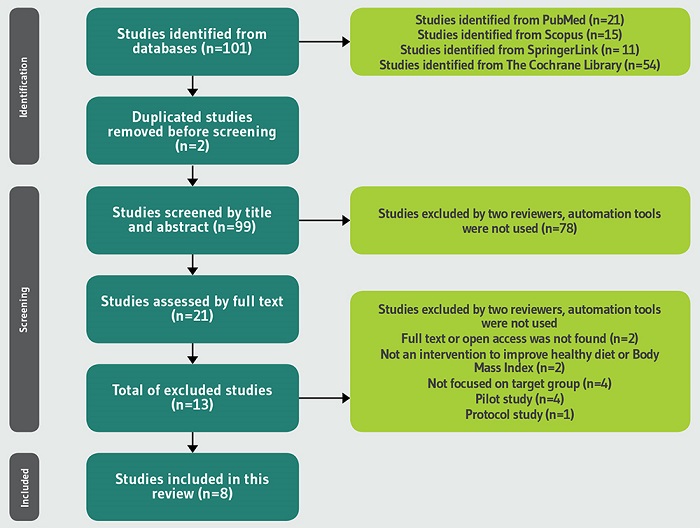
The following PRISMA flow diagram (Figure 1) shows the search and selection process. Two studies appeared to meet the inclusion criteria, however, some of the studies included were focused on different target groups, interventions did not have educational components, or some did not include parents. Therefore, they were excluded15,16. Eventually, a total of 8 studies were included.
General characteristics and risk of bias of included studies are represented in Table 1 20-27. Two had a not defined setting by the nature of the intervention (ICT-T exclusively). See Supplementary Materialmaterial suplementario.
Table 1. General characteristics.
| Study | Design | Intervention characteristicsa | Preschoolers datab | Risk of biasc |
|---|---|---|---|---|
| Iaia et al., 201720 | RCT | Italy; multidimensional educational; 6 months; childcare centers. | n=425, IG=199, CG=226; 3 years; M (52%), F (48%). Italian (91.2%) or foreign (8.8%). | A (82%) |
| Barkin et al., 201821 | RCT | EEUU; multicomponent behavioral; 36 months; physicians' offices and community settings. | n=610, IG=304, CG=306; 3 to 5 years; M (49.3%), F (50.7%). Hispanic, Mexican origin (61.7%). Hispanic, Non-Mexican origin (30.4%); Non-Hispanic black (6.3%); Non-Hispanic white (0.7%); Non-Hispanic other (1.0%). | A (94%) |
| Steenbock et al., 201922 | RCT | Germany; multicomponent health promotion program; 40 weeks; daycare facilities. | n=831, IG=440, CG=391; 3 to 5 years; M (50.5%), F (49.5%). German no migration data (75.9%); Others (24.1%). | B (74%) |
| Romo et al., 201823 | RCT | Ecuador; educational and behavioral; 3 (PI) and 7 (EI) months in 2 sequential school years; school and home. | n=307, IG=152, CG=155; 3 to 4 years; M (53%), F (46.9%). N/R. | B (66%) |
| Nyström et al., 201724 | RCT | Sweden; mobile-based; 6 months; N/D. | n=313, IG=155, CG=158; 4 years; M (53%), F (47%). Sweden (98.1%); Other (1.9%). | A (86%) |
| French et al., 201825 | RCT | EEUU; multicomponent; 3 years; home and community. | n=534, IG=265, CG=269; 2 to 4 years; M (49.1%), F (50.9%). Non-Hispanic White (9.1%); Non-Hispanic Black (18.1%); Hispanic, any race (61.9%); Multiracial (9.1%); Other (1.9%). | A (82%) |
| Natale et al., 201726 | RCT | EEUU; multicomponent; 2 years over 3 academic school years; childcare centers. | n=1211, IG=754, CG=457; 46.7 monthsd M (49.88%), F (50.12%). Hispanic Cubans (15.35%); Other Hispanics (40.96%); Non-Hispanic blacks Haitians (14.12%); Other Non-Hispanic blacks (19.02%); Non-Hispanic whites (6.69%); Other (3.86%). | B (68%) |
| Karmali et al., 202027 | RCT | Canada; coaching-educational; 3 months; N/D. | n=50, IG=25, CG=25; 2 to 10 years; M (36%), F (64%). Caucasian (78%); African Canadian (8%); Native/Aboriginal (2%); Latin-American (4%); Asian (2%); Other (4%). | B (74%) |
EI: Enhance intervention for IG; N/D: Not defined; N/R: Not reported; PI: Pilot intervention for CG; RCT: Randomized control trial.
aLocation, type, duration, setting.
bSample size (n) sex masculine (M), feminine (F), nationality/race/ethnicity for the IG.
cA: low; B: medium; C: high.
dMean by month.
In Table 2 20-27 is reported effectiveness of the interventions. For CHD, the only study with negative effects reported that intake of fruits and vegetables (FV) and unsweetened beverages per day was more pronounced for children in the CG at baseline and follow-up. Otherwise, studies with positive effects had significant differences for all its measures, e.g., FV, sugar-sweetened beverages intake (SSB) and water consumption. For CBMI, the study with negative effects was the same that reported negative effects for CHD. For those with positive effects, one reported maintaining a healthy BMI percentile and less increase on the IG, while the other study showed significant differences for BMI-for-age Z score.
Table 2. Effectiveness of interventions.
| Study and Effecta | CHD | CBMI | Additional outcomes |
|---|---|---|---|
| Iaia et al., 201720 (+) Healthy Diet (*) BMI | Low-risk score for fruit and vegetable (≥4 s/db: 19.9% vs. 9.5%; p=0.008) and SSB intake (0 glasses/day: 90.7% vs. 78.6%; pc=0.002) at 2-year-follow-up. | RWGd increase in BMI ≥1 SDe was smaller (9.9 vs. 14.1%) at 2-year follow-up. | Lack of changes among a low level of education (23% had ≤8 years of education). Low-risk for CHBSf among medium/high levels of education (ORg=2.48; p=0.006). |
| Barkin et al., 201821 (/) Healthy Diet (*) BMI | Fewer kcalh intake 95%CIi [38.0-160.7] p=0.002; corrected p=0.003. SD=(363 vs. 397). | No significant BMI difference (B=0.05, 95%CI [−0.29 to 0.38]; p=0.79). Lower risk of developing obesity at 3-month follow-up 0.51 95%CI [0.29-0.92]; p=0.02; corrected p=0.10. | Significant effects on the linear (p=0.03) and quadratic (p=0.02) growth of BMI of children who were food insecure with hunger at baseline. |
| Steenbock et al., 201922 (-) Healthy Diet (-) BMI | Recommended FV per day at baseline 12% vs. 9% and 13% vs. 11% at follow-up. Recommended glasses of unsweetened beverages per day 50% vs. 49% at intervention and 47% vs. 51% at follow-up. | Overweight or obese children increased (5.7 to 9.0 and from 4.6 to 6.25). Body fat increased (9.3 to 10.5%) whereas decreased in the CG (9.4 to 9.0%). | No additional differences were observed. |
| Romo et al., 201823 (+) Healthy Diet (+) BMI | Significant difference (p=0.05) for higher daily SSB consumption. For water consumption (+8.3%; p=0.04), SSB consumption (−16.8%; p<0.001), FV consumption (+15.9%; p=0.01). | Significant differences in mean BMI-for-age z score (−0.25; p<0.001). | 6.1% of children were at risk for being overweight, or had overweight or obesity, but at follow-up no children were in this category, representing a 6.1% reduction. |
| Nyström et al., 201724 (/) Healthy diet (*) BMI | Intake of sweetened beverages (p=0.049). IG had 99% higher odds of increasing the composite scorej for the dietary behaviors (OR: 1.99; 95%CI [1.20, 3.30]; p=0.008). | No difference (mean difference: −0.03 kg/m2; p=0.922). | Children with higher FMIk improved composite score (+0.65 ± 1.38 vs. +0.03 ± 1.33 units; p=0.019), whereas no differences for the children with a lower FMI (+0.04 ± 1.51 vs. −0.13 ± 1.34 units; p=0.506). |
| French et al., 201825 (/) Healthy diet (*) BMI | Fewer kcal per day at 24 (-90 kcal; 95% CI [−164, −16] and 36 months (-101 kcal; 95%CI [−164, −37]). Intake of added sugars was significantly lower (-5.7 g/dl; 95%CI [−10.4, −1.0]). | No significant difference in BMI (-0.12 kg/m2; 95%CI [−0.44, 0.19] or 36 months (-0.19 kg/m2; 95%CI [ −0.64, 0.26]). | Less increase in BMI for overweight or obese children at 36 months (-0.71) kg/m2; 95%CI [−1.30, −0.12]. Among Hispanic children effective in reducing BMI increases at 36 months (-0.59) kg/m2; 95% CI [−1.14, −0.04]. |
| Natale et al., 201726 (*) Healthy Diet (+) BMI | Not statistically significantly changes for FV consumption (b=0.04, [SEm]=0.04, p=0.34) and unhealthy food consumption (b=0.01, SE= 00.03, p=0.80) | Significant less increase in PBMIn (b=-1.95, [SE]=0.97, p=0.04). | Obese children significantly increased consumption of FV over time (b=0.24, SE=0.08, p=0.003). |
| Karmali et al., 202027 (*) Healthy Diet (N/R) BMI | No significant difference for children's protein intake, fiber intake, saturated fat intake, or sodium intake. | N/R | Parents in both groups reported developing changes in perspective, increased awareness of habits, and heightened accountability for making positive changes in themselves. |
a(+): positive; (/): mixed; (-): negative; (*): undefined.
bServings per day.
cp-value.
dRapid weight gain.
eStandard deviation.
fChildren's combined health behaviour score.
gOdds ratio.
hkilocalories.
iConfidence Interval.
jDifference in composite scores (follow-up minus baseline) was calculated for each child.
kFat Mass Index.
lgrams per day.
mStandard error.
nBMI percentile.
In Table 3 20-27 is reported intervention components. For ICT-T, there was a prevalence for telephony, e.g., telephone calls, while for the TA, there was a prevalence for direct contact, e.g., motivational interviewing (MI). Two studies used only ICT-T for their interventions, while the rest of the studies used mixed tools with predominantly use of TA. There were important differences between duration and intensity from each characteristic of the interventions, for some of them, duration and intensity were not specified. Four interventions added community components (e.g., use of parks); whereas two interventions used more creative tools to interact with parents and children (e.g., puppets). It is worth mentioning that telephone calls were used more than any other ICT-T for two specific components of the interventions: MI and coaching to change behaviours.
Table 3. Intervention components.
| Study | Description | Toola | ICT-Tb | TAc | Duration | Intensity |
|---|---|---|---|---|---|---|
| Iaia et al., 201720 | Interventionists were training for MI to parents. | TA | N/Ad | Interviewse | 20 minutes each one. | 2 MI, interval of 1-2 months. |
| Stories with FV characters. Good vs. bad rating of FV eaters and only water consumption. | N/A | Leaflet, manual, posterf | 1 hour/day | At least 1 learning experience. | ||
| Barkin et al., 201821 | Telephone calls regarding nutritional choices and PA. | ICT-T, TA | Telephone callsg | N/A | 12 weeks | Weekly 90-minute. |
| Coaching calls regarding nutritional choices and PA. | Telephone callsg | Personalized lettersh | 9 months | Monthly calls. | ||
| Steenbock et al., 201922 | One activity/game per week about food groups. Activities with parents. | TA | N/A | Newsletters.Card boxf | 40 weeks | Free to choose the modules. |
| PA games with parents and general information of PA. | N/A | Newsletters Card boxf | 40 weeks | Free to choose the modules. | ||
| Take home instructions for healthy meals and PA games. | N/A | Newslettersf | 40 weeks | Free to choose the modules. | ||
| Romo et al., 201823 | Story of 4 fictional children and a turtle, about how to grow and eat FV. | ICT-T, TA | N/A | Storytellinge | 10 months | Not specified. |
| Focused on drinking water, eating FV and engaging PA. | Songsi | Puppets, Models of foods. Pop-up booksh | 10 months | Daily. | ||
| A board with stickers to identify healthy habits and PA in children. | N/A | Board. Stickersh | 10 months | Daily. | ||
| Parents registered for activities and received a themed magnet. | N/A | Workbook Magneth | 10 months | Not specified. | ||
| Nyström et al., 201724 | Focused on healthy eating and PA in preschool children. | ICT-T | Smartphone applicationg | N/A | 6 months | N/A |
| Parents were able to record their children's FV and SSB intake. | Smartphone applicationg | N/A | 6 months | Once a week parents register information. | ||
| French et al., 201825 | Parenting classes with MI. | ICT-T, TA | Telephone callsg | MI Behavior changes modelse | 3 years | 1 hour duration and follow-up phone calls. |
| Natale et al., 201726 | Beverage policy, snack policy, PA policy. | ICT-T, TA | Music CD'si | Food tastinge | 2 years. | Not specified. |
| Staff conducted joint parent-teacher meetings that focused on a nutrition and PA curriculum. | N/A | Role modelinge | 2 years | In year 1, 6 sessions, In year 2, 4 sessions per year. | ||
| Weekly visits to promote positive dietary changes and PAk. | N/A | Visitse | 2 school years | It was implemented weekly at the school year. | ||
| Karmali et al., 202027 | Parents received online health education webinars. | ICT-T | Webinarsj | N/A | 3 months | Six webinars approximately 20-30 min each. |
| Parents received CALCl. The trainer used only his CPCCm skills. | Telephone callsh | N/A | 3 months | 20-30 minutes per coaching sesión. |
aType of tool used.
bName of ICT-T used.
cName of TA used.
dNot applicable.
eDirect contact.
fPrinted materials.
gTelephony.
hDidactic materials.
iRecorded broadcasting technologies.
jInternet.
kPhysical activity.
lCo-active life coaching.
mCertified Professional Coercive Coach.
DISCUSSION
In the study with positive effects for CHD and CBMI, differentiating characteristics were identified. Were used mixed tools, created cartoons or fantasy characters to inspire healthy behaviors and had group activities. In comparison to other interventions in childcare centers or scholar settings, where parents only had instructions to do activities at home, in this study, its school-based activities had a continuation at home because parents were trained and encouraged to provide evidence of completion of a given activity. Moreover, studies had fictional characters as fruits and vegetables for its stories, but the characters used in the intervention with positive effects, were preschool-aged children and animals.
Additionally, most of its components had a daily intensity, in contrast to the intervention that had negative effects, where the dose of interventions was not defined.
Few studies had changes for FV intake. The result is consistent with a recent systematic review, reported that there were no short-term differences in child consumption of FV in meta-analyses of trials examining nutrition education and interventions15. In comparison, the only two studies that showed positive effects for CBMI were applied during scholar years, which is consistent with previous reviews where it mentioned that time is a main factor to evaluate the effectiveness of interventions in weight status, becoming a difficult variable to change in children16.
Some studies showed significant results for children with overweight or obesity, this is consistent with previous results that mention interventions can be more effective as treatment of childhood obesity14. In addition, it was reported that interventions show greater effects in weight loss compared to prevention in children13.
For studies with exclusively ICT-T, the intervention that used a smartphone app had mixed effects with significant results to reduce intake of sweetened beverage intake (p=0.049) at follow-up. Besides, children had 99% higher odds of increasing the composite score (OR: 1.99; 95%CI [1.20, 3.30]; p=0.008) and the effect was more pronounced for children with higher FMI. This is related to a recent systematic review, which mentions that website and app-based interventions can be effective for improving children's dietary intake and nutrition knowledge and can achieve small to moderate changes in nutrient-poor foods and drinks17. In addition, another study that tested the efficacy of a smartphone-delivered intervention to reduce parent provision of sugar-sweetened beverages among preschool children, showed that children had a greater reduction for consumption of SSB, even mothers in the IG had a significant weight loss28.
In contrast, two studies used exclusively TA. One study showed positive effects only for CHD (e.g., SSB intake). This result is related to a previous systematic review where successful strategies to reduce consumption of SSB had provision of written educational materials such as those used in the study included in this review29. The other study showed negative effects for CHD and CBMI. It is worth mentioning that this study had a daycare setting, and in a previous systematic review focused on childcare, less than half of included studies had a significant difference in BMI, BMI-Z score, waist circumference or body fat30. An important characteristic of this study included, is that it gave general information for healthy meals or PA to parents, and this has been previously described as a barrier to obesity prevention in childcare settings instead of being a facilitator, because some parents did nothing for their children to eat healthier when only received information31.
There were some limitations to this systematic review. Only studies written in English and Spanish were included, therefore, studies written in different languages that could increase the quantity and quality of the evidence reviewed were excluded. Moreover, studies were constrained to be available in open access, thus, some studies that seemed accomplished inclusion criteria, nevertheless had a cost to be full text read were excluded. Furthermore, all studies included different settings where its characteristics around healthy diet or BMI could condition outcomes. Similarly, its heterogeneity constrains an exact comparison. Finally, according to the methodological quality of the studies included, results and conclusions of this systematic review must be considered with caution.
On the other hand, to our knowledge, is the most recent evidence of comparison ICT-T and TA, where most of the studies had mixed effects and due to the heterogeneity of the studies, seemed difficult to exactly determine which factors were successful. However, differentiating characteristics were identified in the study with positive effects and should be considered for future interventions. In addition, this review showed that although studies had recent publication dates, there were few with ICT-T. In other words, there is a need to increase the use of ICT, as it is recognized that ICT are essential for achieving the Sustainable Development Goals and are innovative forms to address health needs9.
Furthermore, the results increase the evidence that interventions can be more effective in reducing consumption of not recommended food groups than increasing intake of recommended food groups, as well as are more likely to have effect on children with overweight or obesity. Additionally, interventionists did not evaluate the knowledge acquired through educational components. Therefore, it should be considered and assessed the role of parent's knowledge in children's nutritional status.
CONCLUSIONS
In conclusion, interventions first, seemed more effective as treatment than prevention for preschoolers with overweight or obesity, second, had better results with daily implementation and home settings, and third, showed being successful with a defined dose of the intervention. Similarly, although most used mixed tools, there were few which implemented new methods through ICT-T.

