










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
The World Health Organization (WHO) and the United Nations International Children's (UNICEF) in the Global Strategy for Infant and Young Child Feeding regulate the best feeding pattern for infants from birth to two years of age to improve the quality of health in infants and children by providing breast milk [1]. Mother (ASI) to the baby immediately within one hour after the baby is born, giving only breast milk or exclusive breastfeeding from birth until the baby is 6 (six) months old, providing complementary foods for breast milk (MPASI) since the baby is 6 (six) months to 24 months and continue breastfeeding until the child is 24 months or older [2, 3].
Inadequate breastfeeding is responsible for more than 236,000 child deaths each year and significantly increases the risk of death in infancy and childhood [4]. On the other hand, optimal and exclusive breastfeeding can protect against post-neonatal mortality [5]. In developing countries, infants who are not breastfed have higher rates of diarrhea and respiratory disease [6]. A cohort case study in Ghana found an increased risk of neonatal death with an increased delay in starting breastfeeding from 1 hour to the seventh day. Overall, 16% of neonatal deaths could be saved if all infants were breastfed from day 1 and 22% if breastfeeding was started within one day, the first hour after birth. In addition, a similar study in Bangladesh concluded that infant mortality could be reduced by almost one-third in prevalence because they do not breastfeed significantly increased the risk of the baby getting sick and infected with infectious diseases [7, 8].
Currently, Indonesia is trying to reduce the number of malnutrition, both stunting and wasting, as stated in the 2020-2024 National Medium Term Development Plan (NMTDP). In the national strategy to accelerate stunting prevention, it is stated that nutrition services are carried out inside and outside the building including promotive, preventive, curative and rehabilitative services with an intervention target of the first 1000 days of baby groups (Pregnant Mothers, Breastfeeding Mothers, infants 0-23 months), toddlers and adolescents [9]. The main nutritional service activities carried out are: counseling and nutritional supplementation for pregnant women such as Blood Boosting Tablets (BBT) and additional food for pregnant women with CED (Chronic Energy Deficiency), promotion and counselling of ICF (Infant and Child Feeding), IEB (Initiation Early Breastfeeding), Exclusive Breastfeeding, MP-ASI and continuing breastfeeding for up to 2 years or more, monitoring the growth of toddlers, nutritional supplementation for toddlers (vitamin A and additional food for undernourished children under five), handling malnourished toddlers, and BBT supplementation (Blood Supplement Tablets) in adolescent girls [10].
The low number of breastfeeding mothers is caused by the lack of awareness of a mother on breastfeeding for child growth. In addition, the level of education and low knowledge of access to complete information related to exclusive breastfeeding and its essential role in optimal child growth and development and protecting against infectious diseases, as well as breastfeeding by holding the child close to the body, also strengthens the emotions of the mother and child which can make children have personal resilience and can live independently in the future [11].
Other factors contribute to the low coverage of exclusive breast-feedings such as weaning early habitual of local people, no adequate socialization and advocacy, few hospitals carry out ten steps successful breastfeeding, lack of health workers concern, lacking breastfeeding counsellors, and incomplete recording and reporting from health facilities which only reached 55.56% out of the target 85%. Although it increased from the previous year, it was not significant and still far from the national target. It was recorded that only Kendari City approached the target with achievement of 80.43%. If it is associated with K4 coverage and delivery by health workers, these results do not seem to correlate positively, both regionally and in terms of achievement [12]. Based on the 2018 Basic Health Research (BHR) data, the rate of exclusive breastfeeding is only. The number of exclusive breastfeeding rates may be getting worse with the COVID-19 pandemic [13].
The outbreak of COVID-19, the emergency response status followed by the policy of Large-Scale Social Restrictions (LSSR), will have a significant impact not only on community activities but also on the economic conditions of most people who work in the informal sector. It is feared that it will affect the decline in access and purchasing power of the community to fulfil nutritious food [14]. If this is not anticipated, there will be food and nutrition insecurity, especially in areas identified as vulnerable. Food and nutrition insecurity increases the risk of acute nutritional problems (under-nutrition and malnutrition) in vulnerable groups; even chronic nutrition problems (stunting) may increase if the COVID-19 emergency response is established for a long time (prolonged emergency) [15].
A preliminary study was conducted in the Poasia Health Center Work Area, where the number of babies in 2020 was 644 babies, 290 (45.03%) babies were exclusively breastfed, and 354 (54.97%) babies were not exclusively breastfed. The low level of exclusive breastfeeding in the region still needs to be studied and studied, especially from the causative factors. This problem underlies researchers to conduct research related to factors related to exclusive breastfeeding in the Work Area of the Poasia Health Center, Kendari City.
METHODS
The current cross-sectional study involved 100 participants in the working area of the Poasia Health Center, Kendari City, which was carried out on December 2020 - March 2021, selected by purposive sampling. Inclusion criteria are mothers who have babies aged 6-12 months, who are domiciled in the working area of the Poasia Health Center. while mothers who were sick during the study, mothers who gave birth to premature babies, mothers who were not willing to participate were excluded from the study.
Data were collected using a questionnaire containing questions about maternal characteristics, research variables, and exclusive breastfeeding. Characteristics of respondents include age, occupation, education and parity, family support, staff support, while exclusive breastfeeding means that infants up to 6 months of age do not receive additional food. The age variable is divided based on the age division from BPS Kendari City, 2016. The level of education is divided into high education and low education. Variable types of work are divided into working and not working. The sample criteria followed in this study were all mothers who were six months old and had a husband. Furthermore, the data that has been collected was analyzed bivariate using the Chi-Square test and logistic regression with the help of SPSS version 16.0 to determine the difference in proportions using the level of significance 0.05, which is presented descriptively and tables. This research has been approved by the Haluoleo University Health Research Ethics Commission numbered: 21/KEPK-IAKMI/III/2021.
RESULTS
The results of this study are presented in textual and tabular forms to simplify and facilitate data interpretation, and data presentation is made in the form of the frequency distribution of respondents according to the variables studied. The results of this study are also presented with univariate and bivariate analysis.
The description of the mother's characteristics, research variables and the results of the analysis with exclusive breastfeeding can be seen in Table 1.
Table 1. Results of analysis of respondents characteristics and research variables with exclusive breastfeeding
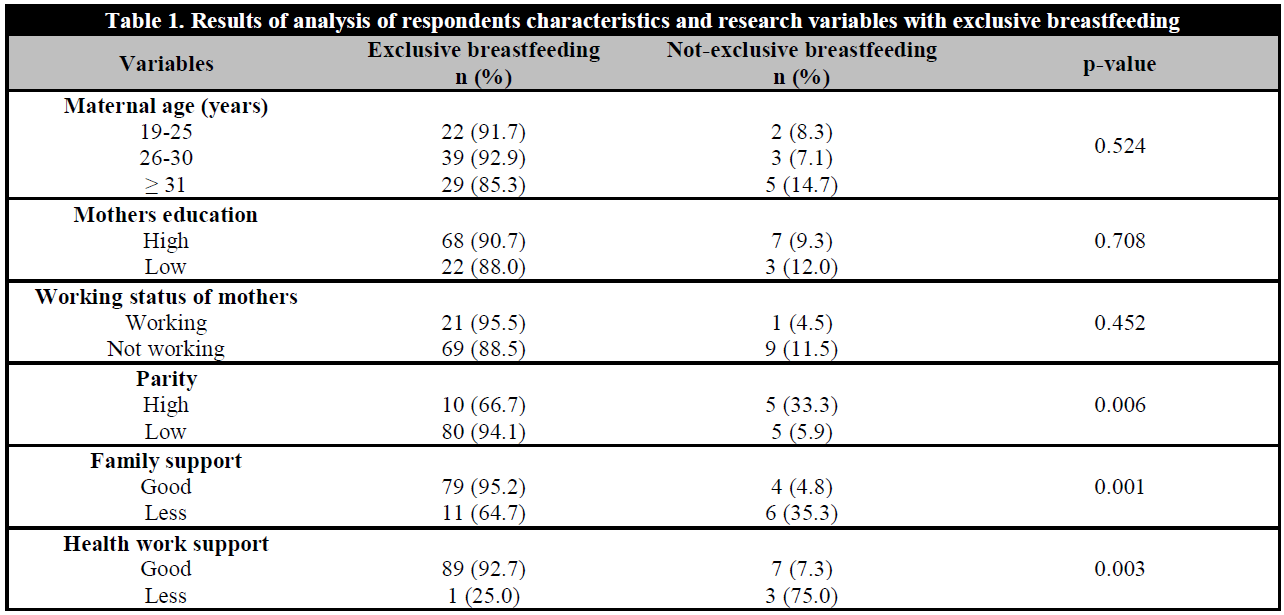
Most of the respondents shown in Table 1 who gave exclusive breastfeeding were 90%, the mother's age was dominated by 26-30 years in the exclusive breastfeeding group, the dominant mother's education level was high, and the work status was in the category of not working, low parity, good family support, and health worker support good. In the non-exclusive breastfeeding group, the distribution of respondents was dominant in the age of 30 years, the level of education was high, the employment status was more or less, the high and low parity were the same, the family support was in less, and the support from the health worker was dominantly good.
The chi-square test showed that the variables that were statistically significant p < 0.25 and related to exclusive breastfeeding were parity, family support, and health care workers' support, while the variables of age, education level, and employment status were not related, so the three significant variables were included in the following analysis. The results of the logistic regression test can be presented in Table 2.
The variable most related to exclusive breastfeeding is family support with an Exponent value (B) = 8.549 with an R square value = 37.8%, meaning that the results of this test can explain exclusive breastfeeding by 37.8%. The three variables tested affected only 37.8% of exclusive breastfeeding, while 62.2% of mothers who gave exclusive breastfeeding were influenced by other factors not examined.
DISCUSSION
Respondents in the age range of 20-35 years are adults where at this age, mothers can solve problems well, one of which will seek accurate information related to exclusive breastfeeding. Mothers aged < 20 years are considered immature both spiritually and physically, so that mothers will rely on others to provide exclusive breastfeeding. Mothers >35 years old begin to experience changes in their hormonal system so that the milk production produced decreases and will become an obstacle for mothers to breastfeed exclusively [16].Most mothers who gave exclusive breastfeeding were aged 20-35 years and gave exclusive breastfeeding, although statistically, no significant relationship was found. In this study, almost all age ranges gave breastfeeding up to 6 months without complementary foods. This study showed that the prevalence of exclusive breastfeeding and the duration of breastfeeding for six months were higher in older mothers.
This is in line with a previous study conducted in the Sungai Raya Dalam PHC working area in 2013, which found that there was no relationship between age and exclusive breastfeeding with p value = 0.200. However, in contrast to previous studies that found a relationship between maternal age and exclusive breastfeeding, mothers aged 20-35 years gave more exclusive breastfeeding to their children, and the p-value = 0.025 with OR value = 2.967 [17].
Bayley and colleagues' research has found that older mothers have more positive attitudes toward breastfeeding [18]. This positive attitude is influenced by psychological factors. Young mothers are more likely to express shame about breastfeeding if there are other people around when they want to breastfeed compared to older mothers [18]. Physiologically, mothers who give birth at the age of more than 30 years tend to experience delayed lacto genesis than younger mothers [19]. Mothers who experience delayed lacto genesis often lose confidence in breastfeeding and often state that breast milk is not enough for the baby so that the baby is often given prelacteal food [20].
The current study found that more highly educated mothers gave exclusive breastfeeding than mothers with low education (SMP and below). This means that the tendency of mothers to breastfeed without complementary foods until the baby is 6 months old is influenced by the mother's understanding of the benefits of breastfeeding for the baby's growth and development.
In the current study, the variable level of maternal education was not associated with exclusive breastfeeding. In line with previous research, which found that education did not affect exclusive breastfeeding, the information obtained regarding exclusive breastfeeding could not be practiced well by breastfeeding mothers [21]. The results of Asare et al.'s research are in line with the results of our study, where mothers who give exclusive breastfeeding are not always mothers with high levels of education but mothers with low levels of education are more able to apply exclusive breastfeeding due to other factors that support it, one of which is the local community culture. It was also found that the culture of feeding babies after a baby is a few days old has been passed down from generation to generation in the community's family living around the Poasia Public Health Center, Kendari City, so that even though the mother breastfeeds her baby, the respondents also provide formula milk and other complementary foods with the purpose of the baby being full.
Work is not a reason to stop exclusive breastfeeding. A study explains the relationship between employment status and exclusive breastfeeding where working mothers tend not to give exclusive breastfeeding. With the proper knowledge about breastfeeding, equipment for expressing breast milk, and support for the work environment, a mother can continue breastfeeding exclusively. With the demands and opportunities to help the family's economy, some mothers choose to work outside the home. Therefore, by working, mothers cannot have complete contact with their babies. As a result, mothers are more likely to give formula milk, which causes breastfeeding frequency to decrease and milk productivity to decrease. This situation causes mothers to stop breastfeeding, while mothers who do not work have free time and can make direct contact with babies while breastfeeding so that milk productivity becomes a lot [22]. Other studies also explain the possibility that working mothers are relatively burdened with office and home activities, so that mothers do not have sufficient time for direct contact with their babies [23].
The results of the existing research are in line with research conducted in Pelamunan Village, PHC Kramatwatu Work Area, namely mothers who give exclusive breastfeeding mostly are mothers who do not work where mothers who do not work have much free time so they can freely contact directly in the breastfeeding process and give breast milk exclusive [24].
Parity is a woman who has given birth [25]. Parity is divided into several terms such as primipara, which is a woman who has given birth to a fetus for the first time, multipara, which is a woman who has given birth to a fetus more than once; and grande multipara, which is a woman who has given birth to a fetus more than five times [26]. This study found a relationship between parity and exclusive breastfeeding where low parity (1-2) times tended to give exclusive breastfeeding to their babies during the COVID-19 pandemic.
Not in line with previous research explaining the relationship between parity and exclusive breastfeeding (p = 0.278) [27], however, the results of this study were different from our research, wherein this study the mother multi-para or grande-multipara have the opportunity to provide exclusive breastfeeding by 4.60 times compared to primi-parous mothers. This difference may be due to the parity categorization in our study being divided into high parity if the mother has given birth ≥ three times so that many mothers have given birth twice (multi-para) but are still in the low parity category. Parity was associated with the mother's experience of breastfeeding. Mothers with more than one Parity will be more confident and able to overcome obstacles during the breastfeeding process (for example, how to overcome breast milk not coming out) so that multiparous or grande multiparous mothers are more likely to breastfeed exclusively [28].
Husband's support is one of the factors that influence the success of exclusive breastfeeding [29, 30]. In this study, it was shown that mothers who received husband's support were more likely to give exclusive breastfeeding than mothers who did not receive husband's support. The best way husbands can provide support to breastfeeding mothers is to act as breastfeeding fathers. A breastfeeding father is the support of a husband as a father to his wife to be successful in the breastfeeding process [31].The current study explains that with the support of the husband, the mother's emotional stability will be stable and motivated to provide her baby with good nutrition, namely exclusive breastfeeding, as evidenced by very few babies who are given additional food after being given education to husbands to provide support to their wives to breastfeed exclusively [32].The results of this study are in line with the theory of family or husband support in exclusive breastfeeding. Most of the husbands in the work area of the Kendari City Poasia support their wives in exclusive breastfeeding so that mothers get emotional support and practical assistance in exclusive breastfeeding.
The role of health workers at the research sites has been perfect. It was also found that mothers who received support from health workers were more likely to give exclusive breastfeeding than mothers who did not receive support from officers. Health workers always provide counselling to pregnant women and breastfeeding mothers about exclusive breastfeeding. Health workers are responsible for infant nutrition and health care [33]. Health workers have a unique position that can affect maternal health services, both before, during, and after pregnancy and childbirth [34]. Respondents received information about the Exclusive Breastfeeding program through the midwife, where they checked their pregnancy and had their baby checked after delivery. Midwives in the PHC area now also always carry out early initiation of breastfeeding in every delivery. In several clinics in the location of this study, there are also particular records regarding infants who are exclusively breastfed.
Under the Government's policy that supports Early Initiation of Breastfeeding and the success of exclusive breastfeeding is influenced by health workers who can provide information about exclusive breastfeeding. In addition to providing counselling about exclusive breastfeeding, health workers also provide other assistance, such as conducting home visits and counselling about the Family Planning (KB) program [35].
LIMITATIONS
We encountered several difficulties in collecting primary data through distributing questionnaires directly to the intended respondents, which became a limitation of the study; so that researchers needed a long time to find respondents who met the research criteria. This is related to the incomplete data on mothers who have babies aged 6-24 months and gave birth outside the Poasia Health Center.

