










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
Permalink10.53986/ibjm.2022.0035
A 78-year-old woman with a medical history of autoimmune hypothyroidism to ER with a 2-week history of discomfort in the left eye. The patient did not report diplopia or vision loss. Visual acuity was 20/20 in both eyes. Both pupils were equal sizes and reactive to light. Ophthalmological examination revealed unilateral left-sided ptosis and contralateral lid retraction (11 mm palpebral fissure in the right eye and 4 mm in left) without limitation of extraocular movements. Cogan’s eyelid twitch was present, as well as worsening of ptosis with sustained upgaze. An ice pack test was performed, with marked improvement of the palpebral aperture (Figure 1).
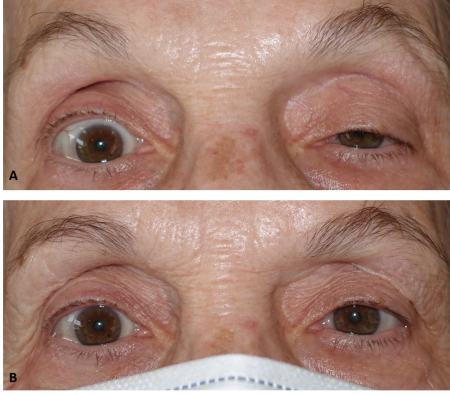
Figure 1 A: Clinical image in primary gaze, showing left-sided ptosis and right palpebral retraction. B Image after a 2-minute ice-pack test, showing resolution of the ptosis.

Figure 2. Anterior and inferior prevascular mediastinal solid mass compatible with Type A thymoma. No obvious or gross mediastinal lymph nodes.
Acetyl choline receptor antibodies (AchR-Ab) level was >20 nmol/L (reference Range: <0.02 nmol/L). Thoracic CT scan was performed, which showed an anterior and inferior mediastinal solid mass (Figure 2), compatible with Type A thymoma. A presumed diagnosis of ocular myasthenia gravis was made. The patient was referred to our local thoracic surgeon, and started on oral pyridostigmine with gradual improvement of the ptosis.
Ocular myasthenia gravis is an autoimmune disorder characterized by the presence of antibodies to postsynaptic nicotinic acetylcholine receptors (AChR) at the neuromuscular junction of striated muscle [1]. Patients typically present with bilateral ptosis, which often varies throughout the course of the day. Diplopia is also a common complaint, due to weakness of the extraocular muscles [2]. Antibodies in myasthenia gravis affect only striated muscles, therefore not being involved the pupillary dilator or sphincter muscles. In patients presenting with ptosis, external ophthalmoplegia or nonphysiologic anisocoria, an alternative diagnosis should be considered. Initial therapy for ocular myasthenia gravis typically consists of acetylcholinesterase inhibitors, such as pyridostigmine 60 mg three times daily [2, 3].
Other differential diagnosis to consider are oculomotor nerve dysfunction or Horner’s syndrome. Oculomotor or CN3 dysfunction can occur due to a pathology of the brainstem nucleus or an injury of the nerve anywhere along its course [4]. Typical clinical findings are unilateral ptosis, with deficits in adduction, supraduction and infraduction. Neuroimaging is usually required, especially if there is pupil involvement, to rule out a compressive aneurysm. Horner’s syndrome, or oculosympathetic paresis, usually presents as mild unilateral ptosis and a miotic pupil that dilates poorly in response to dim illumination [5].
This patient presented to the emergency eye clinic with a new-onset of left lid ptosis, and an otherwise normal neurological exam. Her chief complaint was an inability to open her left eyelid, which worsened at the end of the day. Upon examination, the main ophthalmological finding was a unilateral ptosis. A readily accessible test in the clinic is an ice pack test or rest test, which should result in an improvement in the ptosis, as was seen in this patient. Her palpebral fissure measured 4mmm before ice was applied, and 8mm 2 minutes after the application of ice. The ice test has been reported to have a sensitivity of 86% and specificity of 79% in ocular myasthenia [6]. The test is considered positive if there was an improvement of more than 2 mm on the basis of the distance between the center of the pupillary light reflex and the upper eyelid margin.
Myasthenia gravis’ presentation is widely variable and can mimic other conditions such as cranial nerve palsies. Clinicians should be aware of the potential manifestations of this condition in order to facilitate appropriate and timely testing and diagnosis. The ice pack test presents a high sensitivity and specificity index, and can be an effective method of diagnosis of MG. The clinician should also be familiar with treatment options, as well as their potential side effects, so they can effectively co-manage these patients with other specialists.

