10 cells per high-power field in 1/7 patients, and more than 3 red blood cells per high-power field in 1/6. 1/7 patients presented proteinuria; and 1/77 presented casts. Urinary symptoms, proteinuria, and urinary casts appeared more frequently in patients older than 59 years; pyuria in the group between 15-19 years; and microhematuria in females. Pelvic and retrocecal appendix positions were associated with a higher incidence of voiding symptoms. Duration of abdominal pain and evolution stage did not have any statistical relationship with either symptoms or urine analysis findings. CONCLUSIONS: Urinary tract symptoms are frequent in acute appendicitis; their presence should not exclude the diagnosis of this disease. Urine analysis is not useful to rule out the existence of acute appendicitis.]]>
Urología General
MANIFESTACIONES URINARIAS DE LA APENDICITIS AGUDA.
Ángel Manuel Tundidor Bermúdez, José Antonio Amado Diéguez y Jorge Luis Montes de Oca Mastrapa.
Servicios de Urología y Cirugía General, Hospital General Docente "Guillermo Domínguez", Puerto Padre, Las Tunas, Cuba.
Resumen.- OBJETIVOS: Identificar los síntomas urinarios más frecuentes en la apendicitis aguda. Determinar los hallazgos en los análisis de orina. Relacionar estadísticamente edad, sexo, duración del dolor abdominal, posición del apéndice y estadio evolutivo, con los hallazgos al interrogatorio y en el análisis de orina.
MÉTODOS: Se estudiaron 500 pacientes consecutivos, operados de apendicitis aguda, recogiéndose los datos contemplados en "OBJETIVOS". Se utilizó la prueba de Chi Cuadrado para establecer la relación estadística prevista.
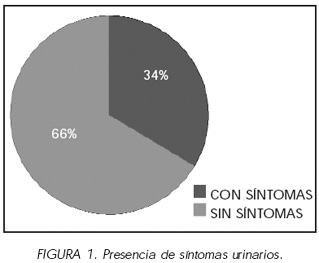
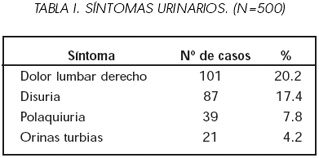
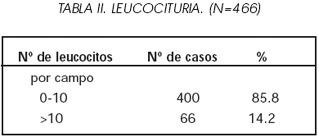
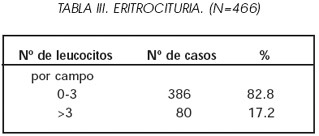
RESULTADOS: Uno de cada 3 pacientes presentó algún síntoma urinario; el dolor lumbar derecho y la disuria fueron los más frecuentes. El sedimento urinario mostró leucocituria superior a 10 células por campo en 1 de cada 7 enfermos, y eritrocituria superior a 3 células por campo en 1 de cada 6. Uno de cada 7 enfermos presentó proteinuria (trazas); y uno de cada 77, cilindruria. Los síntomas urinarios, la proteinuria y la cilindruria se presentaron con mayor frecuencia en mayores de 59 años; la leucocituria, en el grupo de 15-19 años; y la eritrocituria, en el sexo femenino. Las posiciones pelviana y retrocecal del apéndice se asociaron con mayor incidencia de polaquiuria. La duración del dolor abdominal y el estadio evolutivo no guardaron relación estadística con la presencia de síntomas ni con los resultados de los análisis de orina. ]]>
CONCLUSIONES: Los síntomas urinarios son frecuentes en la apendicitis aguda; su presencia no debe excluir el diagnóstico de esta enfermedad. El análisis de orina no es de utilidad para descartar la existencia de una apendicitis aguda.
Palabras clave: Apendicitis. Síntomas urinarios. Análisis de orina.
Summary.- OBJECTIVES: To identify the most frequent urinary tract symptoms of acute appendicitis. To determine the findings in urine analysis. To establish statistically the relationships between age, sex, duration of abdominal pain, appendix position and the evolution stage with the findings on clinical history and urine analysis.
METHODS: We studied 500 consecutive patients undergoing surgery for acute appendicitis registering all data specified in the objectives . The chi-square test was used to establish statistical relationships .
RESULTS: One third of the patients showed some urinary symptoms; right flank pain and dysuria were the most frequent symptoms. Urinary sediment showed pyuria > 10 cells per high-power field in 1/7 patients, and more than 3 red blood cells per high-power field in 1/6. 1/7 patients presented proteinuria; and 1/77 presented casts. Urinary symptoms, proteinuria, and urinary casts appeared more frequently in patients older than 59 years; pyuria in the group between 15-19 years; and microhematuria in females. Pelvic and retrocecal appendix positions were associated with a higher incidence of voiding symptoms. Duration of abdominal pain and evolution stage did not have any statistical relationship with either symptoms or urine analysis findings.
CONCLUSIONS: Urinary tract symptoms are frequent in acute appendicitis; their presence should not exclude the diagnosis of this disease. Urine analysis is not useful to rule out the existence of acute appendicitis.
Keywords: Appendicitis. Urinary tract symptoms. Urine analysis.
Correspondencia
Dr. Ángel M. Tundidor Bermúdez
Calle 5ª nº 22, Reparto Médico ]]>
77210 Puerto Padre. Las Tunas. Cuba.
e-mail: cmicm@villazul.ltu.sld.cu
Trabajo recibido: 24 de septiembre 2004
INTRODUCCIÓN
La apendicitis aguda es la más frecuente de las urgencias quirúrgicas (1), y no tratada oportunamente, suele conducir a graves complicaciones e incluso a la muerte (2). Debido a las limitaciones de las pruebas imagenológicas y de laboratorio empleadas para el diagnóstico de esta entidad (2-4), y a que un medio de mayor precisión como la endoscopia no se encuentra siempre disponible, el reconocimiento de sus variadas formas clínicas sigue siendo un reto para la profesión médica.
La mayoría de las veces, la presentación de la apendicitis es tan típica que no da lugar a dudas diagnósticas; pero en algunas ocasiones pueden aparecer dificultades debido a la presencia de manifestaciones de otros aparatos, lo que se ha relacionado con las variadas posiciones en que el apéndice se puede encontrar (5-13). La superposición de hallazgos inusuales como los relativos al tracto urinario, puede oscurecer el diagnóstico y retardar el tratamiento apropiado (6,8,11,14,15).
Entre las manifestaciones urinarias descritas en la literatura se encuentran síntomas como hematuria macroscópica, dolor lumbar, disuria, polaquiuria y retención urinaria (5,11,14,16-23); complicaciones como dilatación ureteropielocalicial y fístulas apendículo- vesicales o apendículo-ureterales (11,18-20,24- 28); y alteraciones del análisis de orina como bacteriuria, piuria, hematuria microscópica, proteinuria y cilindruria (5,9,11,15,16, 24,26,29-32).
Papazov et al., del Instituto Gorki, (Donietz, Ucrania), publicaron en 1989 una serie de 62 pacientes con apendicitis aguda diagnosticada tardíamente. El diagnóstico inicial fue cólico nefrítico en 49 casos, infección urinaria alta en 8 e infección urinaria baja en 5 (16).
Rothrock et al., de la Universidad de Loma Linda (California, EE.UU), encontraron a la disuria entre las principales causas de diagnóstico tardío de la apendicitis, en niños menores de 13 años (14). En un trabajo ulterior de este mismo autor, realizado en el Orlando Regional Center (Florida, EE.UU.), las infecciones urinarias aparecieron entre los 3 diagnósticos equivocados más frecuentes en mujeres en edad fértil, afectas de apendicitis (33).
]]> La presente investigación tuvo como objetivos:1. Identificar los síntomas urinarios más frecuentes en pacientes con apendicitis aguda, en nuestro medio.
2. Determinar los hallazgos en los análisis de orina en dichos pacientes.
3. Relacionar estadísticamente la edad, el sexo, la duración del dolor abdominal, la posición del apéndice y el estadio evolutivo de la enfermedad, con los hallazgos al interrogatorio y en el análisis de orina.
MATERIAL Y MÉTODO
El universo estuvo constituido por 500 pacientes consecutivos con apendicitis aguda, operados en nuestra institución. Todos los pacientes con el diagnóstico operatorio de la enfermedad fueron entrevistados en las primeras 48 horas siguientes a la intervención.
A cada uno se le confeccionó un formulario donde se consignó edad, sexo, duración del dolor abdominal, síntomas urinarios preoperatorios, resultado del análisis de orina previo a la operación (realizado en 466 casos con apendicitis confirmada), posición del apéndice (según descripción en el informe operatorio) (7), y estadio evolutivo de la enfermedad (de acuerdo con el diagnóstico histopatológico) (34). Fueron excluidos del estudio aquellos pacientes cuyo diagnóstico no fue corroborado por la histología.
La edad de los pacientes estuvo comprendida entre 3 y 93 años (promedio: 26.3 años), distribuida de la siguiente forma: <15 años: 113 casos (22.6%), 15-59: 365 (73.0%) y >59: 22 (4.4%). Correspondieron al sexo masculino 309 casos (61.8%) y al femenino 191 (38.2%). La duración del dolor abdominal varió entre 5 y 168 horas (promedio: 30.8 horas), distribuida como sigue: ≤24 horas: 297 casos (59.4%), 25-72: 175 (35.0%) y >72: 28 (5.6%). La posición del apéndice fue retrocecal en 125 casos (25.0%) y pelviana en 67 (13.4%); se encontró en otras posiciones (iliaca, mesocelíaca o subhepática) en 308 pacientes (51.6%). Correspondieron al estadio precoz (catarral) 89 casos (17.8%), al supurado 372 (74.4%) y al gangrenoso 39 (7.8%).
Se utilizó la prueba Chi Cuadrado sobre diferencias de proporciones, para relacionar estadísticamente la edad, el sexo, la duración del dolor abdominal, la posición del apéndice y el estadio evolutivo de la enfermedad, con los hallazgos al interrogatorio y en el análisis de orina.
RESULTADOS
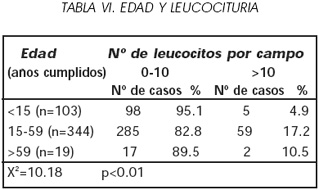
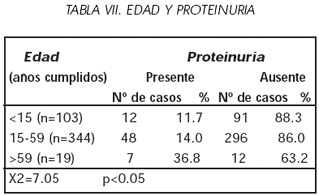
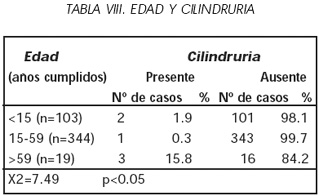
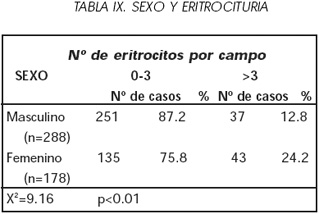
]]> Uno de cada 3 pacientes presentó algún síntoma urinario [Gráfico 1]; el dolor lumbar derecho y la disuria fueron los más frecuentes [Tabla I]. El sedimento urinario mostró leucocituria superior a 10 células por campo en 1 de cada 7 enfermos [Tabla II], y eritrocituria superior a 3 células por campo en 1 de cada 6 [Tabla III]. Uno de cada 7 enfermos presentó proteinuria (trazas); y uno de cada 77, cilindruria [Tabla IV].

La edad influyó en la presencia de síntomas urinarios (más frecuentes en los pacientes menos jóvenes [Tabla V]), de leucocituria (mayor en el grupo de 15-59 años [Tabla VI]), y de proteinuria y cilindruria (más alta incidencia en los mayores de 59 años [Tablas VII y VIII]). No estuvo, empero, relacionada con la magnitud de la eritrocituria.

En cambio, el sexo mostró diferencias significativas en lo tocante al conteo eritrocitario (que resultó superior en las mujeres [Tabla IX]), pero no estuvo relacionado con otras alteraciones en el análisis de orina ni con la presencia de síntomas urinarios.
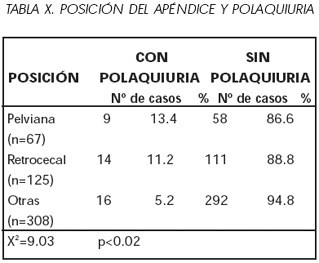
Las posiciones pelviana y retrocecal del apéndice se asociaron con una mayor incidencia de polaquiuria [Tabla X], y no con el resto de los síntomas urinarios ni con alteraciones del análisis de orina. La duración del dolor abdominal y el estadio evolutivo de la enfermedad no guardaron relación estadística con la presencia de los síntomas ni con los resultados de laboratorio.
DISCUSIÓN
]]> En la serie de Papazov et al.(16), compuesta por 62 pacientes con apendicitis diagnosticada tardíamente, el dolor lumbar estuvo presente en 30 casos, y la disuria en 18, contribuyendo a los errores diagnósticos iniciales. Estos fueron también los síntomas urinarios más frecuentes en nuestra casuística.Kretchmar y McDonald, de la Universidad de Rochester (Nueva York, EE.UU.), en un estudio de 113 apendicitis, encontraron que 21 pacientes (19%) presentaban de 5 a 20 leucocitos por campo, y 4 pacientes (3.5%) entre 5 y 30 eritrocitos por campo. La leucocituria resultó superior en mayores de 40 años, y en pacientes con apéndice retrocecal o pelviano; no hubo diferencias significativas en lo tocante al sexo (5).
Scott et al., de la Universidad de Louisville (Kentucky, EE.UU.), consideraron como anormal el sedimento de una muestra de orina recogida por micción espontánea y centrifugada, en el cual aparecieran más de 4 leucocitos o eritrocitos por campo; y encontraron un sedimento con esas características en el 30% de una serie de 100 apendicitis consecutivas. Estos hallazgos correspondieron al 36% de los mayores de 15 años y al 24% de los menores, lo que equivale al 13% de los niños, el 40% de las niñas, el 25% de los hombres y el 50% de las mujeres; este predominio del sexo femenino es atribuido por los autores de dicho artículo, a la contaminación genital de las muestras obtenidas por micción espontánea. El 53% de los análisis anormales correspondió a casos con apéndice retrocecal o pelviano. La incidencia de sedimento anormal en pacientes con apendicitis perforada fue del 50% (9).
Por su parte, Arnbjörnsson, de la Universidad de Lund (Suecia), aceptó como anormal el sedimento urinario que mostrara al menos uno de los siguientes criterios: presencia de cilindros, más de 2 eritrocitos por milímetro cúbico, más de 5 leucocitos por milímetro cúbico, más de 5 células epiteliales por milímetro cúbico, y más de 20 bacterias por campo. Este autor encontró un sedimento con alguno de esos criterios en 30 casos (15%) de una serie de 194 apendicitis (30).
De los casos de Papazov et al., 20 presentaron leucocituria superior a 10 células por campo, 8 tuvieron uno o más eritrocitos por campo, y en 9 se detectó proteinuria (16).
Puskar et al., del Hospital Nuevo de Zagreb (Croacia), siguiendo los criterios de Scott et al. (9), informaron análisis de orina anormal en el 48% de 66 enfermos de apendicitis. La frecuencia de los análisis anormales no estuvo relacionada con la posición anatómica del apéndice, pero resultó directamente proporcional al grado de inflamación (estadio evolutivo) apendicular (26).
Paajanen et al., del Hospital de la Universidad de Kuopio (Finlandia), reportaron la presencia de eritrocitos en la orina del 26% de 188 pacientes afectos de la enfermedad (31).
La disparidad de criterios sobre el sedimento urinario anormal nos impide comparar con exactitud los resultados de los autores citados, con los nuestros.
CONCLUSIONES
1. Los síntomas urinarios son frecuentes en la apendicitis aguda, sobre todo en mayores de 59 años. Su presencia no debe excluir el diagnóstico de esta enfermedad.
]]> 2. Los síntomas urinarios más frecuentemente encontrados fueron dolor lumbar derecho y disuria.3. El análisis de orina no es de utilidad para descartar la existencia de una apendicitis aguda.
4. La duración del dolor abdominal y el estadio evolutivo de la enfermedad no guardaron relación estadística con la presencia de síntomas urinarios ni con el resultado del análisis de orina.
5. Los síntomas urinarios (excepto la polaquiuria) y las alteraciones del análisis de orina, no estuvieron relacionados con la proximidad del apéndice inflamado a las vías urinarias.
BIBLIOGRAFIA y LECTURAS RECOMENDADAS (*lectura de interés y **lectura fundamental)
1. LIU, C.D.; McFADDEN, D.W.: "Acute abdomen and appendix". Greenfield, L.J. (Ed): Surgery: scientific principles and practice. 2 ed. Pp 1246, Lippincott- Raven, Philadelphia, 1997. [ Links ]
*2. WILCOX, R.T.; TRAVERSO, L.W.: "Have the evaluation and treatment of acute appendicitis changed with new technology?". Surg. Clin. North Am., 77: 1355, 1997. [ Links ]
]]>*3. HARDIN, D.M.: "Acute appendicitis: review and update". Am. Fam. Physician, 60: 2027, 1999. [ Links ]
4. FLUM, D.R.; MORRIS, A.; KOEPSELL, T. y cols.: "Has misdiagnosis of appendicitis decreased over time? A population-based analysis". JAMA, 286: 1748, 2001. [ Links ]
*5. KRETCHMAR, L.H.; McDONALD, D.F.: "The urinary sediment in acute appendicitis". Arch. Surg., 87: 209, 1963. [ Links ]
6. MONDOR, H.: "Abdomen agudo". Pp 162, Toray- Masson, Barcelona, 1963. [ Links ]
7. TORROELLA MATA, E.: "Cirugía". T1, Pp 282, Pueblo y Educación, La Habana, 1976. [ Links ]
]]>8. CLAIN, A.: "Hamilton Baileys demonstrations of physical signs in clinical surgery". 16 ed. Pp 293, Year Book Medical Publishers, Chicago, 1980. [ Links ]
*9. SCOTT, J.H.; AMIN, M.; HARTY, J.I.: "Abnormal urinalysis in appendicitis". J. Urol., 129: 1015, 1983. [ Links ]
10. YAMAMOTO, M.; ANDO, T.; KANAI, S. y cols.: "Abnormal urinalysis in acute appendicitis". Hinyokika Kiyo 31: 1723, 1985. [ Links ]
**11. JONES, W.G.; BARIE, P.S.: "Urological manifestations of acute appendicitis". J. Urol., 139: 1325, 1988. [ Links ]
12. DIANA, M.; ZOPPE, C.; MASTRANGELI, B.: "Lematuria di origine appendicolare". Arch. Ital. Urol. Androl., 71: 229, 1999. [ Links ]
]]>13. DELIC, J.; SAVKOVIC, A.; ISAKOVIC, E.: "Variations in the position and point of origin of the vermiform appendix". Med. Arh., 56: 5, 2002. [ Links ]
14. ROTHROCK, S.G.; SKEOCH, G.; RUSH, J.J. y cols.: "Clinical features of misdiagnosed appendicitis in children". Ann. Emerg. Med., 20: 45, 1991. [ Links ]
15. MAHMOODIAN, S.: "Appendicitis complicating pregnancy". South Med. J., 85: 19, 1992. [ Links ]
*16. PAPAZOV, F.K.; TIKHI, A.T.; BELIK, I.E. y cols.: "Errors in diagnosis of acute appendicitis in dominating urological symptoms". Vestnik Khirurgii, 142: 120, 1989. [ Links ]
17. FARIÑA, L.A.; ALLENDE, L.; HOCSMAN, H.: "Absceso pelviano y retención aguda de orina por apendicitis". Arch. Esp. Urol., 45: 71, 1992. [ Links ]
]]>18. MAIO, G.; ARAGONA, F.; CISTERNINO, A. y cols.: "Urological manifestations of acute appendicitis: report of two new cases". Urol. Int., 48: 242, 1992. [ Links ]
19. KUBO, M.; TAGUCHI, K.; FUJISUE, H. y cols.: "Hydronephrosis as a complication of appendicitis: a case report". Hinyokika Kiyo, 42: 679, 1996. [ Links ]
20. IDA, K.; YAMAGUCHI, K.; NISHIMURA, Y. y cols.: "Hydronephrosis as a complication of the apendiceal abcess: report of a case". Hinyokika Kiyo, 46: 181, 2000. [ Links ]
21. GALINKIN, D.; KATZ, S.; GREENWALD, M. y cols.: "Pseudotumor of the bladder as a manifestation of uncomplicated appendicitis". J. Clin. Gastroenterol., 32: 367, 2001. [ Links ]
22.PREECE, J.M.; BEVERLEY, D.W.: "Acute urinary retention: an unusual presentation of acute apendicitis in a 3 year old boy". Arch. Dis. Child, 84: 269, 2001. [ Links ]
]]>23. SALIM, A.S.; AHMED, T.M.: "Acute appendicitis presenting as urinary retention: a note of caution". Saudi Med. J., 23: 353, 2002. [ Links ]
24. SELMAN, S.H.; GRECOS, G.P.: "Appendico-ureterocutaneous fistula: report of a case". J. Urol., 128: 593, 1982. [ Links ]
25. REIG RUIZ, C.; VILA BARJA, J.; QUINTANILLA MUÑOZ, B. y cols.: "Fístula apendicovesical secundaria a apendicitis. Revisión de la literatura". Arch. Esp. Urol. 46: 340, 1993. [ Links ]
26. PUSKAR, D.; BEDALOV, G.; FRIDRIH, S. y cols.: "Urinalysis, ultrasound analysis, and renal dynamic scintigraphy in acute appendicitis". Urology, 45: 108, 1995. [ Links ]
27. MONTERO SÁNCHEZ, M.; GÓMEZ TELLADO, M.; MÉNDEZ GALLART, R. y cols.: "Ureterohidronefrosis secundaria a absceso apendicular". Arch. Esp. Urol., 50: 972, 1997. [ Links ]
]]>28. IZAWA, J.I.; TAYLOR, B.M.; DENSTEDT, J.D.: "Appendicovesical fistula: case report and review". Can. J. Urol., 5: 566, 1998. [ Links ]
29. GRAHAM, J.A.: "Urinary cell counts in appendicitis". Scot. Med. J., 10: 126, 1965. [ Links ]
*30. ARNBJÖRNSSON, E.: "Bacteriuria in appendicitis". Am. J. Surg., 155: 356, 1988. [ Links ]
31. PAAJANEN, H.; TAINIO, H.; LAATO, M.: "A chance of misdiagnosis between acute appendicitis and renal colic". Scand. J. Urol. Nephrol., 30: 363, 1996. [ Links ]
32. PUSKAR, D.; VUCKOVIC, I.; BEDALOV, G. y cols.: "Urinary tract infection in acute appendicitis". Acta Med. Croatica, 51: 197, 1997. [ Links ]
]]>33. ROTHROCK, S.G.; GREEN, S.M.; DOBSON, M. y cols.: "Misdiagnosis of appendicitis in nonpregnant women of childbearing age". J. Emerg. Med., 13: 1, 1995. [ Links ]
34. ROBBINS, S.L.; COTRAN, R.S.; KUMAR, V.: "Patología estructural y funcional". 3 ed. Pp. 862, Interamericana, México D.F., 1988. [ Links ]
]]>