800,000 IU/mL in 67% (n = 36). Liver biopsy was performed in 86% (n = 46), 22% (n = 12) had advanced fibrosis. Forty were naïve, 4 relapsing and 10 non-responders. Ribavirin dose was modified in one patient alone due to adverse effects. End treatment response and sustained virological response (SVR) were 59 and 41%, respectively. A univariate analysis revealed a statistically significant association of SVR with baseline viremia (p = 0.006), baseline GGT (p = 0.025), and a reduction in viremia ≥ 2 logs at 2, 4 and 12 weeks (p = 0.001). The extent of viremia reduction at week 2 was associated with 100% SVR, and at 4 weeks the positive predictive values was 84% and the negative predictive values was 96.5%. A subanalysis of the naïve group yielded analogous results. Conclusions: in our study, a reduction in viremia ≥ 2 logs 2 weeks after treatment could ensure SVR. At 4 weeks, most non-responders could be identified.]]>
800.000 UI/ml en 67% (n = 36). Se realizó biopsia hepática en 86% (n = 46), 22% (n = 12) tenían fibrosis avanzada. 40 fueron naïves, 4 recidivantes y 10 no respondedores. La dosis de ribavirina se modificó por efecto secundario sólo en un paciente. La RFT y la RVS fueron de 59 y 41%, respectivamente. El análisis univariante mostró asociación estadísticamente significativa con RVS de la viremia basal (p = 0,006), GGT basal (p = 0,025) y el descenso en la viremia ≥ 2 logaritmos a las 2, 4 y 12 semanas (p = 0,001). El descenso de la viremia en la semana 2 se asoció con 100% de RVS y a las 4 semanas el VPP fue 84% y el VPN 96,5%. Se realizó un subanálisis en el grupo de pacientes naïves con resultados superponibles. Conclusiones: en nuestro estudio el descenso de la viremia ≥ 2 logaritmos a las 2 semanas de tratamiento aseguró la RVS. A las 4 semanas, identificamos a la gran mayoría de los pacientes no respondedores.]]>
Viral kinetics during the first month of treatment in patients with genotype 1 chronic hepatitis C
Cinética viral durante el primer mes de tratamiento en pacientes con hepatitis crónica C genotipo 1
A. Hernández, F. Domper, A. León1, R. Lorente, B. López, E. de la Santa, M. Cabanillas, R. Patón, J. Olmedo, M. D. Galván and E. Rodríguez
Units of Digestive Diseases and 1Research Support. Hospital General de Ciudad Real. Spain
]]>
ABSTRACT
Objective: to identify predictive factors of response to pegylated interferon alpha-2b and ribavirin in patients with genotype 1 chronic hepatitis C. Viral kinetics were studied in weeks 2 and 4.
Methods: a prospective and consecutive study of patients with genotype 1 chronic hepatitis C referred to our Hepatology Clinic between January 2004 and October 2006 for antiviral treatment. Baseline data were recorded and viremia levels were determined hours before the weekly dose of pegylated interferon by qualitative and quantitative PCR.
Results: 57 patients were included in the study, although 3 of these were excluded during follow up; 65% were male (n = 35), with a mean age of 42 (26-65) years. Baseline viremia levels were > 800,000 IU/mL in 67% (n = 36). Liver biopsy was performed in 86% (n = 46), 22% (n = 12) had advanced fibrosis. Forty were naïve, 4 relapsing and 10 non-responders. Ribavirin dose was modified in one patient alone due to adverse effects. End treatment response and sustained virological response (SVR) were 59 and 41%, respectively. A univariate analysis revealed a statistically significant association of SVR with baseline viremia (p = 0.006), baseline GGT (p = 0.025), and a reduction in viremia ≥ 2 logs at 2, 4 and 12 weeks (p = 0.001). The extent of viremia reduction at week 2 was associated with 100% SVR, and at 4 weeks the positive predictive values was 84% and the negative predictive values was 96.5%. A subanalysis of the naïve group yielded analogous results.
Conclusions: in our study, a reduction in viremia ≥ 2 logs 2 weeks after treatment could ensure SVR. At 4 weeks, most non-responders could be identified.
Key words: Hepatitis C. Treatment. Pegylated interferon. Viremia. Predictive factors.
RESUMEN
Objetivo: identificar qué factores predicen la respuesta al interferón pegilado alfa-2b y ribavirina en pacientes con hepatitis crónica C genotipo 1. Se estudió la cinética viral en la semana 2 y 4.
Métodos: se evaluaron de forma prospectiva y consecutiva a los pacientes con hepatitis crónica C genotipo 1 remitidos a nuestra consulta de hepatología entre enero de 2004 y octubre de 2006, para tratamiento antiviral. Se recogieron datos basales y la viremia se determinó horas antes de la dosis semanal de interferón pegilado por PCR cualitativa y cuantitativa. ]]>
Resultados: cincuenta y siete pacientes fueron incluidos aunque 3 fueron excluidos durante el seguimiento. Un 65% fueron varones (n = 35) con edad media de 42 (26-65) años. La viremia basal fue > 800.000 UI/ml en 67% (n = 36). Se realizó biopsia hepática en 86% (n = 46), 22% (n = 12) tenían fibrosis avanzada. 40 fueron naïves, 4 recidivantes y 10 no respondedores. La dosis de ribavirina se modificó por efecto secundario sólo en un paciente. La RFT y la RVS fueron de 59 y 41%, respectivamente. El análisis univariante mostró asociación estadísticamente significativa con RVS de la viremia basal (p = 0,006), GGT basal (p = 0,025) y el descenso en la viremia ≥ 2 logaritmos a las 2, 4 y 12 semanas (p = 0,001). El descenso de la viremia en la semana 2 se asoció con 100% de RVS y a las 4 semanas el VPP fue 84% y el VPN 96,5%. Se realizó un subanálisis en el grupo de pacientes naïves con resultados superponibles.
Conclusiones: en nuestro estudio el descenso de la viremia ≥ 2 logaritmos a las 2 semanas de tratamiento aseguró la RVS. A las 4 semanas, identificamos a la gran mayoría de los pacientes no respondedores.
Palabras clave: Hepatitis C. Tratamiento. Interferón pegilado. Viremia. Factores predictores.
Introduction
Chronic hepatitis caused by hepatitis C virus (HCV) has a strong impact in our setting and is the most common cause of cirrhosis and liver carcinoma in Western countries (1). Today, the prevalence of HCV infection is 1-2% in developed countries, and it is the first indication for liver transplantation in Europe and the United States (2). Around 20% of patients with chronic infection will develop hepatic cirrhosis, with an annual risk of progression to hepatocellular carcinoma of 1-4%.
Current therapy, based on pegylated interferon (pegIFN) and ribavirin (RBV), achieves an overall sustained virological response (SVR) of 54-56%, thus improving disease prognosis (3,4).
Therapeutic response can be influenced by patient characteristics, virus type, and treatment used. These variables help to identify the probable degree of response in each case, reducing unnecessary costs and side effects, improving adhesion to treatment, and helping to identify patients who could benefit from more intensive or prolonged treatment.
Viral kinetics (variations in viral load) during treatment is the most important factor predictive of response and can assist therapeutic decision-making. Early virological response (EVR) is defined as a reduction by at least 2 logs of baseline viral load at week 12 of treatment. If EVR is not achieved, the probability of SVR is greatly reduced, with a predictive negative value (PNV) approaching 100%, and today's clinical guidelines recommend treatment discontinuation (5,6). Rapid viral response (RVR), defined as a negative viral load obtained at week 4, is a good predictive factor of SVR, with a positive predictive value (PPV) of 91% (7-13). Although several studies have defined treatment duration, very few have assessed the value of viral kinetics early during the process.
The aim of this study was to identify which factors predict response to pegIFN alpha-2 and RBV in patients with genotype 1 chronic hepatitis C infection, and to evaluate baseline virus- and host-related factors, especially the dynamic factors of viral kinetics in the second and fourth weeks of treatment.
]]>Patients and methods
Patients with genotype 1 chronic hepatitis C referred to the Hepatology Clinic in our hospital between January 2004 and October 2006, and starting antiviral treatment with pegIFN alpha-2b and RBV were studied prospectively and consecutively.
Inclusion criteria were: age between 18 and 70, positive PCR in serum for HCV, ALT levels higher than normal (≤ 40 IU/L) in the past year. Exclusion criteria were: coinfection with HIV, HBsAg serology or positive hepatitis B viral DNA, contraindicated use of pegIFN or RBV, decompensated cirrhosis, active IVDU, and patients recruited from prisons.
Patients received pegIFN alpha-2b (PegIntron; Schering Plough) at a dose of 1.5 μg/kg weight once a week subcutaneously, and RBV (Rebetol; Schering Plough) orally with weight-based dosing (< 65 kg: 800 mg/day; 65-85 kg: 1,000 mg/day; > 85 kg: 1,200 mg/day) in fractionated morning and evening doses for 48 weeks.
Baseline clinical and laboratory data were recorded during treatment at weeks 2, 4, 8, 12, 16, 20, 24, 36 and 48, and after treatment completion at week 72. Viremia was determined hours before the weekly dose of pegIFN at weeks 2, 4, 12, 24, 48, 60 and 72.
Viral load was measured using the Cobas Amplicor HCV Monitor 2.0 technique (detection limit of 600 IU/mL) until October 2005. Negative samples were submitted for qualitative RNA determination in Cobas Amplicor HCV Test, version 2.0 (sensitivity of 50 IU/mL). After this time the technique used was COBAS Taqman HCV (sensitivity 15 IU/mL, with quantitative determination up to 43 IU/mL). A low baseline load was considered for ≤ 800,000 IU/mL (12,13).
HCV genotype was determined using the Inno-lipa II technique (Innogenetics).
Patients with RBV-induced anemia were administered human recombinant erythropoietin 40,000 IU/week subcutaneously as described in other studies to avoid having to reduce RBV dosing (14,15).
Sustained viral response (SVR) was described as HCV RNA negativity more than 6 months after treatment completion. End-of-treatment response (ETR) was HCV RNA negativity at week 48. Early virologic response (EVR) was a reduction by at least 2 logs of baseline viral load at week 12 of treatment. Viral response at week 4 (VR4) was established as a reduction by at least 2 logs of viral load at week 4. Rapid viral response (RVR) was defined as negative HCV RNA at 4 weeks. Viral load response at week 2 (VR2) was defined as a reduction by at least 2 logs of baseline viral load at week 2.
]]> Statistical analysisThe study design corresponded to a single-cohort, longitudinal follow-up study. Descriptive statistics for qualitative variables were defined using frequency distribution tables and pie charts. Quantitative variables were defined using central tendency statistics, dispersion, and histograms. Using inferential statistics, the main study variable, SVR, was analyzed using the χ2 test and Fischer's exact test for qualitative variables, and the Mann-Whitney and Kruskal-Wallis tests for quantitative variables.
Results
A total of 57 patients with genotype 1 chronic hepatitis C were included in the study, although three patients did not complete the study - two did not attend study visits and one was urgently operated upon for complicated abdominal hernia. Therefore, a total of 54 patients completed the follow-up.
Adherence to treatment was very good (> 80% of the dose) in 94.4% of patients; RBV dose was modified in just one patient with anemia and with partial response to erythropoietin.
Baseline characteristics of patients
Of all 54 patients completing the study, 35 were men (64.8%). Mean age at treatment onset was 42.7 years (26-65 years). Forty patients were naïve (74.1%), 4 had relapsed with previous treatment (7.4%), and 10 were non-responders (18.5%).
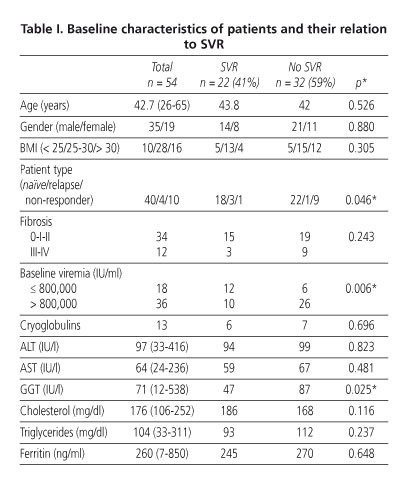
Liver biopsies were performed in 46 (85%). Ten had grade III-IV fibrosis. Baseline viral load was > 800,000 IU/mL in 36 (66.7%). Body mass index (BMI) was > 30 in 16 patients (30%). Thirteen patients had associated cryoglobulinemia (24%).
Laboratory data are recorded in table I.
]]> End-of-treatment response and sustained viral response
Per protocol, ETR was 59.3% (32/54) and SVR was 41% (22/54). By subgroups, SVR was 45% (18/40) in naïve patients, 75% (3/4) in relapsing patients, and only 10% (1/10) in non-responders to previous treatment (IFN or IFN + RBV).
Predictive factors of response
The primary objective of the study was to predict SVR by studying baseline characteristics and viral kinetics during treatment. Baseline characteristics and their relation to SVR are recorded in table I. In the comparative analysis, baseline viral load (p = 0.006), baseline GGT (p = 0.025), and patient type - naïve, relapsed or non-responder (p = 0.046) - reached statistical significance.
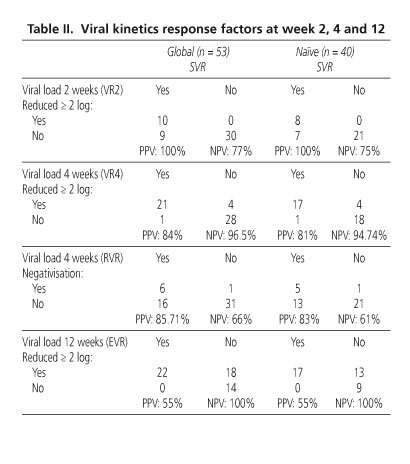
In the study, dynamic factors of viral kinetics such as reduced viral load by ≥ 2 logs at week 2 (VR2), week 4 (VR4), and week 12 of treatment (EVR), and also RVR, reached the greatest statistical significance (p = 0.001) (Table II). VR2 had a PPV of 100% that gradually decreased during treatment. Conversely, NPV increased steadily to 100% at week 12 (EVR). Rapid response predicts cure, while lack of response at 12 weeks indicates that the patient is unlikely to respond. In our study, NPV for ≥ 2 log reduction in baseline viral load at week 4 (VR4) was 96.5%.
Study in the naïve patient subgroup
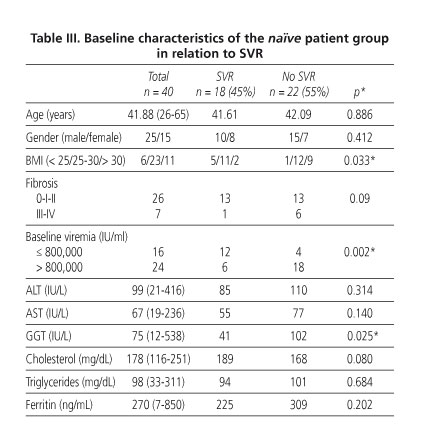
The comparative study was also conducted in the naïve patient subgroup (n = 40), in which baseline factors such as viral load (p = 0.002), GGT (p = 0.025) and BMI (p = 0.033) reached statistical significance. Advanced hepatic cirrhosis was associated with poor response to treatment without reaching statistical significance (p = 0.09), although this would probably reach significance in a larger series (Table III).
Adverse effects of treatment
Although mild adverse effects were common, treatment was not discontinued in any case. Subcutaneous erythropoietin was administered to one patient with hemoglobin under 10 g/dL. RBV dose was reduced in only one patient owing to partial response to erythropoietin. Neutropenia and platelet deficiency did not require dose adjustment. Significantly altered TSH levels were observed in 3.8%, and these patients were referred to the Endocrinology Clinic. Mood alteration was observed in 53%, and a small proportion of these were referred to the Psychiatry Clinic and started treatment with antidepressants.
Discussion
SVR rate for naïve patients with genotype 1 chronic hepatitis C treated with combined pegIFN and RBV for 48 weeks is 42-51% (3,4). In our series, SVR was 41% for the entire sample of patients and 45% for naïve patients. Non-responders had an SVR of 10%. These results were similar to those reported in the HALT-C and EPIC3 studies for previous non-responders to combined treatment with standard IFN with SVR rates from 12-14%, which rose to 53% in case of relapse (16,17).
In our study, we had very high treatment adherence (94.4%), possibly related to close monthly follow-up for the first 6 months and the use of erythropoietin in anemic patients to avoid having to reduce RBV dose in the first 6 months, as described in previous studies (14,15). This would suggest that the SVR rate in our study should have been even higher, although we did include a significant proportion of patients with severe fibrosis (22%), high baseline viral load (66.7%), BMI > 30 (30%), and cryoglobulins (24%), all of them factors associated with poor treatment response.
In recent years, several baseline factors and factors during treatment have been associated with SVR (18). In our study, baseline viral load and GGT reached statistical significance in both the whole patient group and the group of naïve patients. BMI was also a statistically significant factor in the naïve group, although not in the global patient group, possibly due to a larger heterogeneity of the patient group caused by the inclusion of non-responders. In the naïve group fibrosis almost reached statistical significance and would probably do so in a larger sample.
Predictive factors of response with the greatest statistical significance were those associated with viral kinetics. A reduction in viremia ≥ 2 logs 2 weeks after treatment onset confirmed SVR. Monitoring at 2 weeks would therefore be justified as patients could be encouraged to continue with treatment. At 4 weeks, we can identify the majority of non-responders and a high percentage of patients with SVR. Patients with a drop of ≥ 2 logs at week 4 have a PPV in our study of 84%, and a NPV of 96.5%, so only a small percentage of patients who continue on treatment will respond, although this should be confirmed in larger patient groups.
It seems, therefore, that two subgroups with different behavior can be defined: one group in which viral load does not drop, and another group with reduced viral load by ≥ 2 logs, which shows the importance viral suppression speed at week 4.
]]> The possibility of achieving SVR is related to two factors of viral kinetics: the speed of HCV RNA suppression and the duration of this suppression during treatment, as shown by Ferenci and colleagues (6). For genotype 1, they showed the value of viral load determination at week 4: if RVR was achieved, SVR was 91%, comparable to SVR of more favorable genotypes (genotypes 2 and 3). When there was no RVR, but instead complete EVR, with viral negativization at week 12, the reduction in SVR depended on whether the load at week 4 had dropped by ≥ 2 logs (SVR: 70%) or < 2 logs (SVR: 60%). In patients with partial EVR, with a drop in week 12 of at least 2 logs, but without viral negativization, SVR dropped to 43%, showing the importance of the whole period during which HCV RNA is undetectable for SVR prediction. This means that essentially two patient subgroups can be defined, which could receive different treatment regimens on the basis of their viral kinetics. Regardless of EVR, the longer patients take to achieve HCV RNA negativization the less likely they are to achieve SVR.Monitoring viral load in the treatment of genotype 1 chronic hepatitis C is beneficial for the patient. If predictive factors are favorable, the patient will be encouraged to adhere to treatment. From our findings it seems recommendable to extend viral load monitoring to week 2, and then corroborate the extent of response at week 4, taking into account not only RVR but also VR4, defined as a drop by at least 2 logs in baseline viral load, with a PPV similar to that of RVR, but a higher NPV.
References
1. Shepard CW, Finelli L, Alter MJ. Global epidemiology of hepatitis C virus infection. Lancet Infect Dis 2005; 5: 55. [ Links ]
2. Di Bisciglie A. Hepatitis C. Lancet 1998; 351: 351-5. [ Links ]
3. Manns MP, McHutchinson JG, Gordon SC, Rustgi VK, Shiffman M, Reindollar R, et al. Peginterferon alfa-2b plus ribavirin compared with interferon alfa-2b plus ribavirin for initial treatment of chronic hepatitis C: a randomized trial. Lancet 2001; 358: 958-65. [ Links ]
4. Fried MW, Shiffman ML, Reddy KR, Smith C, Marinos G, Goncales FL Jr, et al. Combination peginterferon alfa-2a plus ribavirin for chronic hepatitis C virus infection. N Engl J Med 2002; 347: 975-82. [ Links ]
5. Davis G, Wong J, McHutchison J, Manns M, Harvey J, Albrecht J. Early virologic response to treatment with peginterferon alfa-2b plus ribavirin in patients with chronic hepatitis C. Hepatology 2003; 3839: 645-52. [ Links ]
6. Ferenci P, Fried MW, Shiffman ML, Smith CI, Marinos G, Goncales FL Jr, et al. Predicting sustained virological responses in chronic hepatitis C patients treated with peginterferon alfa-2a (40KD)/ribavirin. J Hepatol 2005; 43: 425-33. [ Links ]
7. Fried MW, Hadziyannis SJ, Shiffman M, Messinger D, Zeuzem S. Rapid virological response is a more important predictor of sustained virological response (SVR) than genotype in patients with chronic hepatitis C virus infection. J Hepatol 2008; 48: S5. [ Links ]
8. Dalgard O, Bjoro K, Hellum KB, Myrvang B, Ritland S, Skaug K, et al. Treatment with pegylated interferon and ribavarin in HCV infection with genotype 2 or 3 for 14 weeks: a pilot study. Hepatology 2004; 4: 1260-5. [ Links ]
9. Von Wagner M, Huber M, Brg T, Hinrichsen H, Rasenack J, Heintges T, et al. Peginterferon-alpha-2a (40kD) and ribavirin fop 16 or 24 weeks in patients with genotype 2 or 3 chronic hepatitis C. Gastroenterology 2005; 129: 5-7. [ Links ]
10. Mangia A, Santoro R, Minerva N, Ricci GL, Carretta V, Persico M, et al. Peginterferon alfa-2b and ribavirin for 12 vs 24 weeks in HCV genotype 2 or 3. N Egl J Med 2005; 352: 2609-17. [ Links ]
11. Zeuzem S, Buti M, Ferenci P, Sperl J, Horsman Y, Cianciara J, et al. Efficacy of 24 weeks treatment with peginterferon alfa-2b plus ribavirinin patients with chronic hepatitis C infected with genotype 1 and low pre-treatment viremia. J Hepatol 2006; 44: 97-103. [ Links ]
12. Zeuzem S, Awlotsky JM, Lukasiewicz E, Von Wagner M, Goulies I, Lurie Y, et al. International, multicenter, randomized, controlled study comparing dynamically individualized versus standard treatment in patients with chronic hepatitis C. J Hepatol 2005; 43: 250-7. [ Links ]
13. Sánchez-Tapias JM, Diago M, Escartín P, Enriquez J, Romero-Gómez M, Bárcena R, et al. Peginterferon alfa-2a (40KD) plus ribavirin for 48 versus 72 weeks in patients with detectable HCV-RNA at week 4 of treatment. Gastroenterology 2006; 131: 451-60. [ Links ]
14. Pockros PJ, Shiffman ML, Schiff ER, Sulkowski MS, Younossi Z, Dieterich DT, et al., Proactive Study Group. Epoeitin alfa improves quality of life in anemic HCV-infected patients receiving combination therapy. Hepatology 2004; 40: 1450-8. [ Links ]
15. Afdhal N, Dieterich DT, Pockros PJ, Schiff ER, Shiffman ML, Sulkowski MS, et al., Proactive Study Group. Epoetin alfa maintains ribavirin dose in HCV-infected patients: a prospective double-blind randomized, controlled study. Gastroenterology 2004; 126: 1302-11. [ Links ]
16. Shiffman M, Di Bisciegle A, Lindsay K, Morishima C, Wright E, Everson G, et al. Peginterferon alfa 2a and ribavirin in patients with chronic hepatitis C who have failed prior treatment. Gastroenterology 2004; 126: 1015-23. [ Links ]
17. Poynard T, Schiff E, Terg R, Moreno Otero R, Flamm S, Schmidt W, et al. Sustained viral response is dependent on baseline characteristic in the retreatment of previous alfa interferon/ribavirin no responders: final results from the EPIC program. J Hepatol 2008; 48(Supl. 2): S369. [ Links ]
18. Alberti A, Chemello L, Benbegnu L. Natural history of hepatitis C. J Hepatol 1999; 31(Supl. 1): 17-24. [ Links ]
![]() Correspondence:
Correspondence:
Francisco Domper Bardají.
C/ Hospital de la Misericordia, 9, 5º D.
13003 Ciudad Real, Spain.
e-mail: franciscodomper@telefonica.net
Received: 24-03-09. ]]> Accepted: 26-05-09.
]]>