Chronic hepatitis C treatment in a cystic fibrosis patient in the pulmonary pre-transplant stage
Tratamiento de hepatitis crónica C en un paciente con fibrosis quística en situación de pretrasplante pulmonar
L. Adán Merino1, A. Olveira Martín1, C. Prados2, F. Gea Rodríguez1, P. Castillo Grau1, E. Martín Arranz1, J. C. Sáenz3 and J. M. Segura Cabral1
Departments of 1Gastroenterology, 2Pulmonary Medicine and 3Pathology. La Paz University Hospital. Madrid, Spain
]]>
ABSTRACT
The standard treatment of chronic hepatitis C, pegylated interferon and ribavirin (pegI/R), has many limitations in both effectiveness and secondary effects, which makes it unsuitable or even contraindicated for some patients. In hepatitis C virus-infected cystic fibrosis patients this treatment could increase respiratory infections with subsequent pulmonary function deterioration. On the contrary, hepatitis C virus (HCV) infection may make lung transplant (LT) unfeasible. We present the case of a cystic fibrosis-young man diagnosed with HCV infection during LT assessment who was treated with pegI/R. In spite of the lung function worsening and respiratory infections, he managed to complete treatment and even sustained virological response (SVR). At present he is on LT waiting list.
Key words: Hepatitis C. Cystic fibrosis. Lung transplant. Pegylated interferon. Ribavirin. Respiratory infections.
RESUMEN
El tratamiento estándar de la hepatitis crónica C, interferón pegilado (INF-peg) y ribavirina (RBV), puede ser inadecuado o incluso estar contraindicado en algunos pacientes debido a sus limitaciones en cuanto a eficacia y efectos adversos. En pacientes con fibrosis quística infectados por el virus de la hepatitis C (VHC) el tratamiento antiviral podría aumentar las infecciones respiratorias con el consiguiente empeoramiento de la función pulmonar. Por contra, la infección por VHC podría desestimar a estos pacientes para un necesario trasplante pulmonar. Presentamos el caso de un varón con fibrosis quística diagnosticado de infección VHC durante su evaluación previa al trasplante pulmonar. El paciente fue tratado con INF-peg y RBV. A pesar del empeoramiento en la función pulmonar y numerosas infecciones respiratorias intercurrentes, logró completar el tratamiento y obtener respuesta viral sostenida, encontrándose actualmente en lista de espera.
Palabras clave: Hepatitis C. Fibrosis quística. Trasplante pulmonar. Interferón pegilado. Ribavirina. Infecciones respiratorias.
Introduction
Pegylated interferon (pig-INF) and ribavirin (RBV) combination is the standard treatment of chronic hepatitis C (CHC), although it has many limitations in both effectiveness and secondary effects, which makes it unsuitable or even contraindicated for some patients (1). Neither specific studies nor case reports exist for hepatitis C virus-infected cystic fibrosis (CF) patients who have received peg-INF and RBV. This treatment may cause and increase respiratory infections with subsequent lung function worsening, taking into account that for non-CF HCV-infected people this treatment involves a higher risk of infections in different foci (urinary, dental, respiratory...) (2). It would be worse in the pre-lung transplant stage, in which 1.9% of patients are infected by hepatitis C virus (HCV) (3). On the other hand, HCV infection may make lung transplant (LT) unfeasible (3,4).
]]> We report a case of a CF-young man diagnosed of HCV infection during LT assessment. As CHC was considered as contraindication to the necessary LT, treatment with peg-INF and RBV was started causing development of numerous respiratory infections and worsening of pulmonary function. However, the patient managed to complete treatment and even sustained virological response (SVR) was obtained. At present he's on a LT waiting list.
Clinical case
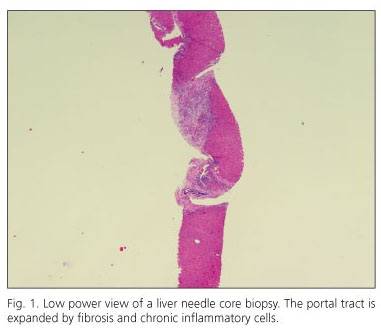
A 28-year old male suffering from CF, affecting lungs and pancreas started with a progressive deterioration of lung function: forced expiratory volume in one second (FEV1) 40%, forced vital capacity (FVC) 99%, the ratio FEV1/FVC 55% and arterial blood oxygen saturation (SO2) 92%. This fact led us to consider LT. In the previous study, HCV was detected (genotype 1b, viremia 1.58e7 IU/mL). The laboratory data showed a normal blood count with 102% of prothrombin activity and the next hepatic biochemical profile: aspartate aminotransferase (AST) 96 IU/L, alanina aminotrasnferase (ALT) 12 IU/L, gamma-glutamyl transpeptidase (GGT) 64 IU/L, and alkaline phosphatase (AF) 156 IU/L. The abdominal ultrasound demonstrated a chronic liver disease without portal hypertension or focal lesions. Liver biopsy showed a marked typical CF affectation that prevented evaluation of HCV damage (Figs. 1 and 2). No other causes for liver disease were found. The analytical controls carried out up until then had showed no signs of liver disease except for occasional slight GGT increase. Ursodeoxicolic acid treatment was started but LT was rejected by reference unit because of the HCV infection.

Owing to this, we decided to start treatment with weekly pegINF alfa 2b 80 mcg and daily ribavirin 1000 mg for 48 weeks. Common secondary effects such as asthenia, anorexia and weight loss followed. No anemia or neutropenia was found to force patterned dose adjustments or use blood growth factors (Basal: hemoglobin 12.9 g/dL, neutrophil 1,800/mL. Nadir: hemoglobin 11.2 g/dL [10th week], neutrophil 1,060/mL [22th week]. Initially, he was followed up monthly (with a first visit at 15th day). However, from the 4th week until the end of treatment, he was admitted at hospital eight times because of sudden respiratory deterioration, so part of the monitoring was performed during hospitalization. In the last one, coinciding with the eighth month of treatment showed the next parameters: FEV1 30%, FVC 67%, FEV1/FVC 38%, arterial pH 7.21 and arterial oxygen pressure (pO2) = 59 mmHg. Before the treatment, he had been admitted to the hospital (specifically four times last year) for worsening respiratory. The germs detected colonising respiratory tract had been H influenzae and S aureus meticilin-sensible in that moment, whereas during the treatment new germs were isolated in the sputum cultures such as A. xilosoxydans or S. aureus meticillin-resistant. Antibiogram-based antibiotics and standard therapy slightly improved respiratory function. Antiviral treatment obtained early and end-of-treatment virological responses (RNA HCV undetectable by PCR at 12th and 48th week respectively). One month after peg-INF and RBV, respiratory function was still severely deteriorated although slightly better than previously (FEV 43%, FVC 82%, FEV1/FVC 44%, SO2 92%). Nevertheless, six months later he suffered a greater spirometric deterioration and he was presented as a candidate for LT. At that moment HCV RNA was undetectable (SVR), allowing him to be listed for LT.
Discussion
CHC has received little attention in the LT field. Although in immuno-competent patients CHC is slowly progressive (2-8% of patients under 40 develop cirrhosis after 20 years) (5), natural history aggravates in immunodeficients (6,7). For this reason the International Guidelines for the Selection of Lung Transplant Candidates list hepatitis C as a contraindication to LT (4). Therefore although this is not uniformly followed in all Transplant Units (3), HCV-infected patients should be ideally treated before LT. Nevertheless this strategy has many limitations mainly derived from pulmonary function deterioration. On the other hand to carry out treatment after LT-associated respiratory improvement increases the risk rejection, being considered an absolute contraindication 1. This situation makes it necessary to re-evaluate the contraindication degree of peg-INF and RBV in CF patients in pre-LT situation. In the case that has been presented, the necessary LT, because of his precarious pulmonary function, forced to us to treat HCV infection that contraindicated LT.
]]> Data proceeding from kidney, heart and liver transplant suggest an HCV negative impact in survival rates (8-10). Information available from LT is limited and from small series. In Sahi's et al. retrospective study (6,11) HCV-infected patients received LT (one of them because of CF). Previously, one was treated with alpha 2b INF, without identifying who it was nor what the complications were. After one year, acute rejections and survival were similar to HCV-negative patients, with a single acute rejection attributed to azathioprine.In Doucette's et al. study (12) pegINF and RBV were given to 5 HCV-LT candidates (none of them with CF). All had at least one acute exacerbation of their neumopathy that required antibiotic treatment and three of them needed more oxygen due to an increase of the dyspnea. Authors concluded that selected HCV-patients can be safely and effectively treated before LT.
We know that in patients with genotype 1 chronic hepatitis C, the viral kinetics is a prediction of response to treatment with peg IFN and RBV (13). The reduction in viremia > or = 2 logs at week 2 was associated with 100% SVR, and at 4 weeks the negative predictive values was 96.5% in a recent prospective study (14). However, we have no information about SVR durability after LT. In Sahi's study the treated patient didn't respond (11). In Doucette's, 3 out the 5 achieved SVR. On the publication date, two were on the waiting list; whereas the third one was transplanted 21 months earlier, maintaining SVR (12). According to kidney and liver series, post-transplant relapse risk would be 3.6% after 2-7 years after the transplant (15).
In conclusion, there's no consensus on pre-LT HCV-infected patients management. PegI/R experience is scarce and until this report there were none on CF patients. In case of treatment, respiratory deterioration is expected. Adequate attention of intercurrent complications allows scheduled antiviral treatment to be completed and if SVR results, this facilitates LT. More studies are necessary with these types of patients in order to agree an appropriate management of these patients.
References
1. Ghany M, Strader DB, Thomas D, Seeff LB. Diagnosis, management and treatment of hepatitis C: An Update. AASLD Practice guidelines. Hepatology 2009; 4: 1335-64. [ Links ]
2. Antonini MG, Babudieri S, Maida I, Baiguera C, Zanini B, Fenu L, et al. Incidence of neutropenia and infections during combination treatment of chronic hepatitis C with pegylated interferon alfa-2a or alfa-2b plus ribavirin. Infection. 2008; 36: 250-5. [ Links ]
3. Cotler SJ, Jensen DM, Kensten S. Hepatitis C virus infection and lung transplantation: a survey of practices. J Heart Lung Transplant 1999; 18: 456-9. [ Links ]
4. International guidelines for the selection of lung transplant candidates. The American Society for Transplant Physicians (ASTP)/American Thoracic Society (ATS)/European Respiratory Society (ERS)/International Society for Heart and Lung Transplantation (ISHLT). Am J Respir Crit Care Med 1998; 158: 355-64. [ Links ]
5. Seeff LB. Natural history of chronic hepatitis C. Hepatology 2002; 36: S35-S46. [ Links ]
6. Soto B, Sánchez-Quijano A, Rodrigo L, del Olmo JA, García-Bengoechea M, Hernández-Quero J, et al. HIV infection modifies the natural history of chronic parenterally acquired hepatitis C with an unusually rapid progression to cirrhosis. A multicenter study on 547 patients. J Hepatol 1997; 26: 1-5. [ Links ]
7. Prieto M, Berenguer M, Rayón JM, Córdoba J, Argüello L, Carrasco D, et al. High incidence of allograft cirrhosis in hepatitis C virus genotype 1b infection following transplantation: relationship with rejection episodes. Hepatology 1999; 29: 250-6. [ Links ]
8. Bouthot BA, Murthy BV, Schmid CH. Long term follow-up of hepatitis C virus infection among organ transplant recipients: implications for policies on organ procurement. Transplantation 1997; 63: 849-53. [ Links ]
9. Forman LM, Lewis JD, Berlin JA, Feldman HI, Lucey MR. The association between hepatitis C and survival after orthotopic liver transplantation. Gastroenterology 2002; 122: 889-92. [ Links ]
10. Fong TL, Hou L, Hutchinson IV, Cicciarelli JC, Cho YW. Impact of hepatitis C infection on outcomes after heart transplantation. Transplantation 2009; 88: 1137-41. [ Links ]
11. Sahi H, Zein NN, Metha A, Blazey HC, Meyer KH and Budev M. Outcomes after lung transplantation in patients with chronic hepatitis C virus infection. J Heart Lung Transplant 2007; 26: 466-71. [ Links ]
12. Doucette KE, Weinkauf J, Summer S, Ens K, Lien D. Treatment of hepatitis C in potential lung trasplant candidates. Transplantation 2007; 83: 1652-5. [ Links ]
13. Aguilar Reina J. Viral dynamics and prediction of response to treatment with pegylated interferon and ribavirin in patients with chronic hepatitis C. Rev Esp Enferm Dig. 2009;101: 665-70. [ Links ]
14. Hernández A, Domper F, León A, Lorente R, López B, de la Santa E, et al. Viral kinetics during the first month of treatment in patients with genotype 1 chronic hepatitis C. Rev Esp Enferm Dig 2009; 101: 671-9. [ Links ]
15. Welter MW, Zeuzem S. Occult hepatitis C: How convincing are the current data. Hepatology 2009; 49: 665-75. [ Links ]
 Correspondence:
Correspondence:
Luisa Adán Merino.
Departamento de Aparato Digestivo.
Hospital Universitario de La Paz.
Paseo de la Castellana 261.
28046 Madrid, Spain.
e-mail: luisaadan@gmail.com