HBsAg seroclearance or seroconversion induced by peg-interferon alpha and lamivudine or adefovir combination therapy in chronic hepatitis B treatment: a meta-analysis and systematic review
Yun Zhang1, Bangtao Chen1,2, Lin Wang3, Junjie Chi2, Shaojuan Song1, Mingshe Liu1 and Zhongfu Zhao1
1 Institute of Liver Diseases. Changzhi Medical College. Changzhi, China.
2 First Hospital of Shanxi Medical University. Shanxi Medical University. Taiyuan, China.
3 Liver Research Center. Beijing Friendship Hospital. Capital Medical University. Beijing, China
Yun Zhang and Bangtao Chen contributed equally this work.
]]> Correspondence
ABSTRACT
Background and aims: Seroclearance or seroconversion of hepatitis B surface antigen (HBsAg) is generally considered as a clinical endpoint. The purpose of the present meta-analysis was to evaluate the effect of combined therapy with pegylated interferon alpha (PEG-IFNα) with or without lamivudine (LAM) or adefovir (ADV) on HBsAg seroclearance or seroconversion in subjects with chronic hepatitis B (CHB).
Methods: Randomized controlled trials performed through May 30th 2015 in adults with CHB receiving PEG-IFNα and LAM or ADV combination therapy or monotherapy for 48-52 weeks were included. The Review Manager Software 5.2.0 was used for the meta-analysis.
Results: No statistical differences in HBsAg seroclearance (9.9% vs. 7.1%, OR = 1.47, 95% CI: 0.75, 2.90; p = 0.26) or HBsAg seroconversion (4.2% vs. 3.7%, OR = 1.17, 95% CI: 0.57, 2.37; p = 0.67) rates were noticed between PEG-IFNα + LAM and PEG-IFN α + placebo during post-treatment follow-up for 24-26-weeks in subjects with hepatitis Be antigen (HBeAg)-positive CHB.
No statistical differences in HBsAg clearance (10.5% vs. 6.4%, OR = 1.68, 95% CI: 0.75, 3.76; p = 0.21) were seen, but statistical differences in HBsAg seroconversion (6.3% vs. 0%, OR = 7.22, 95% CI: 1.23, 42.40; p = 0.03) were observed, between PEG-IFNα + ADV and PEG-IFNα for 48-52 weeks of treatment in subjects with HBeAg-positive CHB.
A systematic evaluation showed no differences in HBsAg disappearance and seroconversion rates between PEG-IFNα + placebo and PEG-IFNα + LAM for 48-52 weeks in subjects with HBeAg-positive CHB.
A systematic assessment found no differences in HBsAg disappearance and seroconversion rates between PEG-IFNα + placebo and PEG-IFNα + LAM during 24 weeks' to 3 years' follow-up after treatment in subjects with HBeAg-negative CHB. ]]>
Conclusion: Combined therapy with PEG-IFNα and LAM or ADV was not superior to monotherapy with PEG-IFNα in terms of HBsAg seroclearance or seroconversion.
Key words: Adefovir. Chronic hepatitis B. Combination therapy. Hepatitis B surface antigen. Peginterferon alpha. Lamivudine.
Introduction
Approximately 350 million individuals are infected with hepatitis B virus (HBV) in the whole world. Chronic HBV infection remains a health problem worldwide, which is closely associated with hepatic fibrosis, compensated or decompensated liver cirrhosis, and liver cancer, especially in the Asia-Pacific region (1). Antiviral therapy may be crucial to prevent the progression of liver cirrhosis, and to reduce end-stage liver disease and hepatocellular carcinoma (HCC). Antiviral agents for the treatment of chronic hepatitis B (CHB) include nucleoside/nucleotide analogues (NAs) and interferon-alpha (standard or pegylated). Seroclearance or seroconversion of hepatitis B surface antigen (HBsAg) is generally considered as the ideal clinical goal of antiviral therapy (2,3). Meanwhile, an increasing number of research studies have emphasized the prognostic role of serum HBsAg levels in CHB patients treated with peg-interferon alfa (PEG-IFNα) and/or NAs, especially in HBeAg-positive individuals. However, few systematic reviews of the ideal endpoint have been thus far proposed to provide a scientific basis for the evaluation of these different antiviral therapies.
One meta-analysis (including nine trials) published in 2011 tried to analyze the efficacy of lamivudine (LAM) monotherapy and PEG-IFNa + LAM combination therapy focusing on HBsAg seroclearance or seroconversion, and the result indicated that PEG-IFNa + LAM combination therapy was more effective than LAM monotherapy for HBsAg clearance or seroconversion. However, the result of this study was poorly accepted by doctors in clinical practices because the meta-analysis had ignored either treatment duration (24 weeks or 52 weeks) or HBeAg status (positive or negative). Moreover, among the nine original trials included, combination therapy had followed a simultaneous or a sequential approach, and treatment-free follow-up exhibited different durations (4). Another meta-analysis (three trials included) published in 2013 showed no difference in HBsAg clearance between combined interferon plus adefovir (ADV) therapy and interferon monotherapy, but no reference was made to HBsAg seroconversion (5).
In our present meta-analysis, we aimed to determine the efficacy of PEG-IFNα + NA combination therapy and PEG-IFNα monotherapy on HBsAg seroclearance or seroconversion in HBeAg-positive/negative CHB patients.
Methods
Inclusion and exclusion criteria
]]> Studies that met all the following inclusion criteria were included: a) study type: clinical randomized controlled trial (RCT); b) study population: HBsAg-positive and HBeAg-positive/negative CHB patients; c) intervention type: PEG-IFNα combined with LAM or ADV therapy vs. PEG-IFNα monotherapy for at least 48 weeks; d) outcomes: HBsAg clearance or HBsAg seroconversion measured at the end of treatment or follow-up.Studies that met any of the following exclusion criteria were excluded: a) non-clinical studies; b) non-adult patients; pregnant or breast-feeding women; patients co-infected with hepatitis C virus, hepatitis D virus, or human immunodeficiency virus; patients with a history of alcohol or drug abuse, hepatocellular carcinoma, decompensated liver disease, serious medical or psychiatric illness, or liver transplantation; c) therapy period less than 48 weeks; concurrent use of corticosteroids, immunosuppressive agents, tyrosine alpha-1 or Chinese herbal medicine; d) not reporting any of the efficacy measures of HBsAg clearance or HBsAg seroconversion as defined by the authors; e) republished studies or full text not available; and f) abstracts in English with full text in a language other than Chinese or English.
Literature search strategy
Two researchers independently performed a literature retrieval by electronic searches of The Cochrane Central Register of Controlled Trials (CENTRAL) in The Cochrane Library, MEDLINE (via Ovid), EMBASE (via Ovid), and the Chinese Biomedical CD Database (CBM), China Network Knowledge Information (CNKI), Chinese Science Journal Database (CQVIP), and Wanfang Database. All the above databases were searched from their date of inception onwards through May 30th 2015. The following search terms were used: "hepatitis B", "interferon", "nucleoside/nucleotide analogs", "lamivudine", "adefovir", and "combination therapy". In addition, conference proceedings in Chinese and citations in previous publications were searched.
Selection of studies
Two authors independently screened the studies according to the prespecified selection criteria. Disagreements were resolved by their conferring with each other.
Efficacy measures and definitions
HBsAg clearance was defined as the disappearance of HBsAg from the serum. HBsAg seroconversion was defined as HBsAg disappearance plus anti-HBs antibody appearance.
Data extraction and management
Two researchers extracted data independently using the same data extraction form, and reached consensus by discussion with each other when discrepancies developed. The following key characteristics and data were extracted from each trial: study design, sample size calculations, methods of combination, HBeAg positivity or negativity, country, interventions (species, dosage, duration of therapy, length of follow-up), outcomes (events and total number).
]]> Assessment of methodological quality in included studiesTwo authors independently assessed the methodological quality of each randomized trial included according to the Jadad quality scale (6). We examined randomization, concealment , blinding, and reporting of patient withdrawal and dropout rates, and a score greater than or equal to 3 was defined as high-quality. Disagreements were resolved by further conferring with each other.
Assessment of heterogeneity and statistical analyses
Quantitative meta-analyses were performed to assess the difference in effectiveness between the PEG-IFNa plus LAM or ADV combination group and PEG-IFNa monotherapy group. In order to further distinguish the difference between ADV and LAM, we performed a subgroup analysis and also took HBeAg status into account. A data synthesis was performed and forest plots were generated using Review Manager Software 5.2 (Cochrane Collaboration, Oxford, England). Due to the dichotomous data, odds ratios (ORs) and their 95% confidence intervals (CIs) were chosen together to evaluate the strength of the association. Heterogeneity was assessed using a Chi-squared test. Heterogeneity was measured using the I2 statistic, and statistical significance was set at p < 0.10. The fixed-effect method (the Peto OR was calculated if "zero" was present in the 2 × 2 table, otherwise the Mantel-Haenszel OR was used) or the random-effect method (D-L OR) (p < 0.10, I2 > 50%) was used to combine the results with different weights in the absence of statistically significant heterogeneity (p ≥ 0.10, I2 ≤ 50%). The overall effect was judged by the Z-test, and p < 0.05 was deemed significant.
Results
Search results and study characteristics
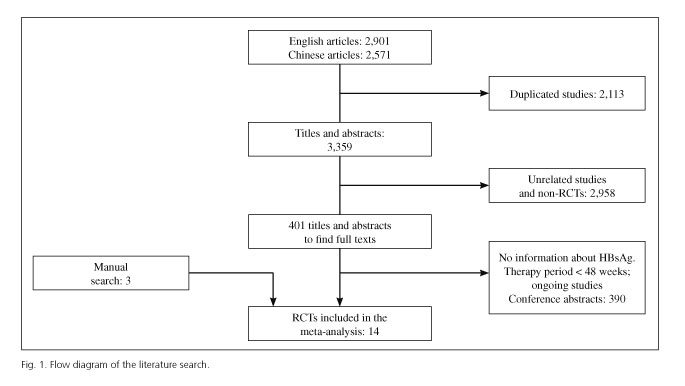
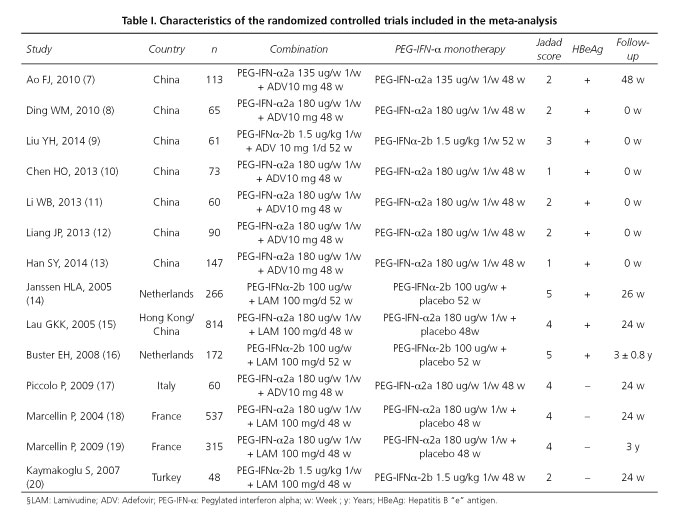
We identified a total of 5,472 publications through electronic searches. Firstly, we excluded 5,071 from these databases, as they were duplicates, clearly irrelevant articles, or non-randomized clinical trials. Then we rejected 390 trials from additional 401 full texts because of treatment duration < 48 weeks, lack of information on HBsAg or no events in both groups, ongoing studies, or only conference abstracts. Additionally, three studies meeting our inclusion criteria were included by hand-searching. A total of fourteen (7-20) clinical randomized controlled trials were included in the meta-analysis. The flow diagram of the literature search was displayed in figure 1. The fourteen studies (7 high-quality ones included) analyzed came from five countries (8 from China, 2 from the Netherlands, 2 from France, 1 from Turkey, 1 from Italy). All studies were published as full publications, eight in English (9,14-20) and six in Chinese (7,8,10-13). Fourteen trials involving a total of 2,818 patients (1,858 HBeAg-positive cases and 960 HBeAg-negative cases) were analyzed in our study; eight trials (7-13,17) and six trials (14-16,18-20), respectively, used PEG-IFNα + ADV and PEG-IFNα + LAM as simultaneous combination therapy for 48-52 weeks; four trials used PEG-IFNα2b (9,14,16,20), and the remaining ten trials used PEG-IFNα2a. Treatment-free follow-up results showed that two of six PEG-IFNα + LAM trials were conducted for an average 3 years (16,19), and the remaining four for 24-26 weeks; two (7,17) of eight PEG-IFNα + ADV trials were followed up for 24-48 weeks, and the remaining six had no follow-up. Of all these trials, three showed both HBsAg clearance and seroconversion (8,14,17), three showed HBsAg seroconversion (9,10,15), and eight showed HBsAg clearance. The characteristics of RCTs included in the meta-analysis are shown in table I.
HBsAg disappearance and seroconversion in the PEG-IFNα + LAM vs. PEG-IFNα + placebo groups for 48-52 weeks (HBeAg-positive patients)
Only a high-quality research was retrieved and analyzed in the study. Janssen HLA et al. (14) showed no difference in the proportion of patients with HBsAg clearance between PEG-IFNα plus LAM (7% [9/130]) and PEG-IFNα plus placebo (5% [7/136], p = 0.54) at the end of treatment (week 48-52). In addition, no differences in the ratio of patients with HBsAg seroconversion was seen between PEG-IFNα plus LAM (6% [8/130]) and PEG-IFNα plus placebo (4% [6/136], p = 0.53).
HBsAg disappearance and seroconversion in the PEG-IFNα + LAM vs. PEG-IFNα + placebo groups for 24-26 weeks of treatment-free follow-up (HBeAg-positive patients)
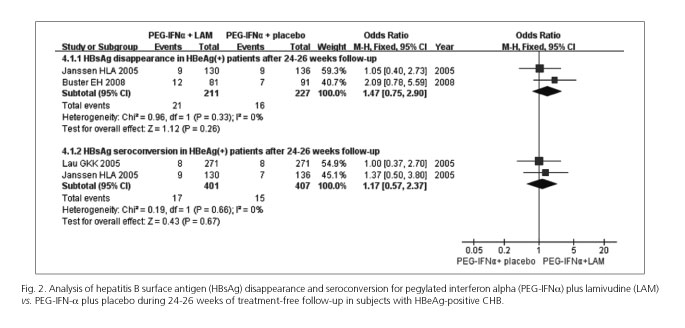
HBeAg-positive patients were followed for 24-26 weeks, and the pooled rates of HBsAg clearance and seroconversion were 9.9% and 4.2% in the PEG-IFNα + LAM group, and 7.1% and 3.7% in PEG-IFNα + placebo group, respectively. No evidences of inter-trial heterogeneity were identified (χ2 = 0.96, d.f. = 1, p = 0.33, I2 = 0%; χ2 = 0.19, d.f. = 1, p = 0.66, I2 = 0%, respectively), and the pooled ORs in our meta-analysis, using a fixed-effects model, showed no significant differences in HBsAg clearance rate (M-H OR = 1.47, 95% CI 0.75, 2.90; p = 0.26) and HBsAg seroconversion rate (M-H OR = 1.17, 95% CI 0.57, 2.37; p = 0.67) (Fig. 2).
]]> HBsAg disappearance and seroconversion in the PEG-IFNα + LAM vs. PEG-IFNα + placebo groups for 24 weeks-3 years of treatment-free follow-up (HBeAg-negative patients)
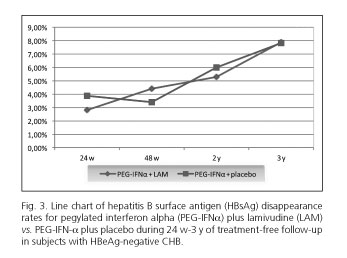
We noticed a highly valuable study for the PEG-IFNα-2a HBeAg-negative chronic hepatitis B study group (18,19), which reported that the HBsAg seroconversion rate of HBeAg-negative patients treated with PEG-IFNα-2a + LAM was 1.7% (3/179), and 2.8% (5/177) for those treated with PEG-IFNα-2a + placebo for 24 weeks of treatment-free follow-up, with no statistical difference detected (p = 0.47). Interestingly, the 3-year follow-up study showed that the HBsAg clearance rates of two treatment groups at the 24th week, 48th week, 2nd year, and 3rd year of follow-up had a general ascending trend; however, there was no significant statistical difference between the PEG-IFNα-2a + LAM group (2.8% [5/179] at week 24, 4.4% [5/114] at week 48, 5.3% [6/114] at year 2, 7.9% [9/114] at year 3) and PEG-IFNα-2a + placebo group (3.9% [7/177] and p = 0.55 at week 24, 3.4% [4/116] and p = 0.71 at week 48, 6.0% [7/116] and p = 0.80 at year 2, 7.8% [9/116] and p = 0.97 at year 3) (Fig. 3). Meanwhile, no statistical difference (p = 0.35) was detected at week 24 of follow-up when the PEG-IFNα + LAM group (3.4% [1/29]) was compared with the PEG-IFNα group (10.5% [2/19]) in a relatively low-quality RCT (without placebo) from Turkey (20).
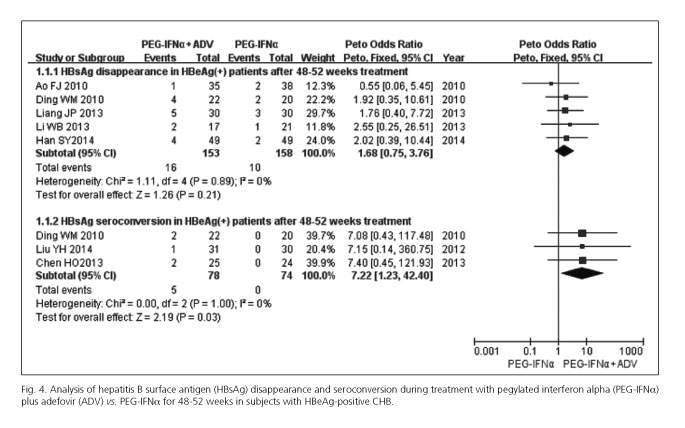
HBsAg disappearance and seroconversion in the PEG-IFNα + ADV vs. PEG-IFNα groups during 48-52 weeks of treatment (HBeAg-positive patients)
The pooled rates of HBsAg disappearance and seroconversion were 10.5% and 6.4% in the PEG-IFNα + ADV group, and 6.3% and 0% in the PEG-IFNα group, respectively. No evidences of inter-trial heterogeneity were identified (χ2 = 1.11, d.f. = 4, p = 0.89, I2 = 0%; χ2 = 0.00, d.f. = 2, p = 1.0, I2 = 0%, respectively); the combined ORs in our meta-analysis using a fixed-effects model demonstrated no significant differences (Peto OR = 1.68, 95% CI 0.75, 3.76; p = 0.21) in terms of HBsAg clearance, while a statistically significant difference was seen in HBsAg seroconversion (Peto OR = 7.22, 95% CI 1.23, 42.40; p = 0.03) (Fig. 4).
]]> HBsAg disappearance in the PEG-IFNα + ADV vs. PEG-IFNα groups during 24-48 weeks of treatment-free follow-up (HBeAg-negative/positive subjects)
Piccolo et al. (17) reported that the HBsAg clearance rate in HBeAg-negative patients treated with PEG-IFNα + ADV was 3.3% (1/30), whereas with PEG-IFNα it was 0% (0/30) after 24 weeks of treatment-free follow-up; no statistical difference was detected between the two treatment groups (p = 0.32). Ao FJ et al. (7) reported a HBsAg eradication rate of 2.8% (1/35) in the PEG-IFNα and ADV combined treatment group for HBeAg-positive patients, and of 2.6% (1/38) in the PEG-IFNα group after 48 weeks of treatment-free follow-up, and no statistical differences were seen (p = 0.95).
Sensitivity analysis and publication bias
A sensitivity analysis was conducted using the M-H OR method instead of the Peto OR when evaluating HBsAg clearance rate in the PEG-IFNα + ADV combination therapy group vs. the PEG-IFNα monotherapy group during 48-52 weeks of treatment. Results showed no statistically significant differences (M-H OR = 1.71, 95% CI 0.74, 3.91; p = 0.21); without inter-trial heterogeneity (χ2 = 1.09, d.f. = 4, p = 0.90, I2 = 0%) stable meta-analysis results were noted. Asymmetric funnel plots were produced based on HBsAg clearance and seroconversion rates between the PEG-IFNα + ADV group and the PEG-IFNα group, which indicated a moderate possibility of publication bias.
Discussion
Currently, two kinds of antiviral drugs (interferon alpha and NAs) have been used in clinical practice to treat HBV infection. NAs have proved to effectively suppress HBV DNA replication, but HBsAg seroclearance or seroconversion, which is considered to be the ideal endpoint of therapy, is rarely obtained and long-term use of NAs frequently results in an increased risk of drug resistance. On the other hand, the advantages of IFN over NAs include absence of resistance, limited duration, and higher HBeAg seroconversion rate; however, a long-lasting response occurs only in a small proportion of patients. Therefore, an identification of novel strategies is needed to induce durable responses in a larger subset of patients. Recent studies have suggested that combination therapy with PEG-IFNα and NAs (LAM, ADV) may enhance therapeutic efficacy. However, it remains controversial whether this combination therapy is more efficient than PEG-IFNα monotherapy when focusing on HBsAg seroclearance or seroconversion.
It was reported that HBsAg seroclearance was 7% among HBeAg-positive patients after 52 weeks on pegylated interferon (14); 5% to 8% after 2-5 years of entecavir monotherapy (21,22); and 1.4% to 10% after 3-4 years of tenofovir monotherapy (23,24). LAM or ADV are no longer used as monotherapy regimens since the advent of tenofovir or entecavir; therefore, in this study, therapeutic efficacy was compared between PEG-IFNα combined with LAM or ADV and PEG-IFNα monotherapy using a meta-analysis of clinical data from 14 eligible trials. Since HBeAg positivity or negativity could reflect a cellular immune response against hepatocytes infected with HBV, we set up subgroups according to HBeAg positivity or negativity in our meta-analysis. Pooled rates of HBsAg seroclearance and seroconversion in our meta-analysis were 10.5% and 6.3% in the PEG-IFNα plus ADV combination treatment group, as compared with 6.4% and 0% in the PEG-IFNα monotherapy group (HBeAg-positive subjets) after 48-52 weeks, respectively; and 9.9% and 4.2% in the PEG-IFNα plus LAM group, as compared with 7.1% and 3.7% in the PEG-IFNα combined with placebo treatment group (HBeAg-positive subjects) after 24-26 weeks of treatment-free follow-up, respectively. Consistently, we also noticed the possibility of a publication bias according to the asymmetric funnel plots. Certainly, our analysis showed that in HBeAg-positive and HBeAg-negative CHB patients higher rates of HBsAg clearance and seroconversion were observed in the PEG-IFNα plus NAs (ADV or LAM) combination group as compared with those in the PEG-IFNα (with or without placebo) monotherapy group. No significant difference was detected in HBsAg clearance and seroconversion. And, interestingly, we found that, with increased follow-up time, HBsAg clearance rates in the two groups (PEG-IFNα + LAM group and PEG-IFNα + placebo group) were enhanced for HBeAg-negative patients. However, there was no significant difference at each follow-up time point.
HBV DNA replication cannot be completely eliminated because covalently closed circular DNA (cccDNA) persists in the nucleus of infected hepatocytes. HBsAg production is related to HBV whole virions, and HBsAg seroclearance would reflect a reduction of cccDNA. So, HBsAg seroclearance or seroconversion was developed as an indicator to evaluate the efficiency of antiviral treatment. Since the antiviral mechanisms of PEG-IFNα and NAs are different, higher HBsAg clearance and seroconversion rates are expected in the combination group when compared to the PEG-IFNα monotherapy group. The immune mechanisms of HBsAg clearance and seroconversion remain unclear, and progress is affected by many factors. Firstly, HBV-specific T-cells are functionally impaired in CHB. It has been reported that NAs may indirectly promote a reduction of PD-1 level and restore HBV-specific T-cell responsiveness by efficiently suppressing HBV DNA replication, even though NA treatment has no remarkable effects on the survival and function of immune cells (25). Secondly, regulatory T-cells (Tregs) and dendritic cells (DCs) play key roles in immune response regulation. The numbers and functions of Tregs and DCs are restored to normal levels after NA treatment (26,27). Thirdly, natural killer cell characteristics in CHB patients are associated with HBsAg clearance (28). Combination treatment with PEG-IFNα and ADV significantly influences NK-cell function (29,30). In addition, B-cells play an important role in the clearance of HBV and in protection against reinfection. IFNα may reverse B-cell hyperactivation and functional impairment, which is related to HBsAg seroconversion in CHB patients (31).
Admittedly, our meta-analysis suggested that the combination of PEG-IFNα and NAs was not more efficient than PEG-IFNα (with or without placebo) monotherapy according to HBsAg clearance and seroconversion, but our study contained several limitations. On the one hand, sample sizes were inadequate and most of the studies included were low-quality studies, which led to difficulties in classifying the risk of bias, which might weaken our meta-analysis conclusions in this regard. On the other hand, we did not take serum HBsAg levels and HBV genotypes into account as we focused on a meta-analysis (32) published in Hepatology Research, which concluded that lower serum HBsAg levels (≤ 100 IU/ml) and HBV genotype B or C were associated with a higher rate of spontaneous HBsAg seroclearance (51.4% vs. 11.7%, p < 0.05). Therefore, most importantly, the decreases in serum HBsAg levels induced by antiviral drugs in the later meta-analysis are also welcomed if they meet the purpose of directing clinical medication for the better, rather than just focusing on HBsAg seroclearance or seroconversion. In addition, this study included a short follow-up period. As it may take longer for the host to enhance their immune response and induce a decline in HBsAg level, it is necessary that observation occurs during a long follow-up period, such as over 3 years. Finally, our study did not analyze ALT levels, as it is generally believed that serum ALT levels reflect the host's immune response to chronic HBV infection and the intensive immune response is quickly restored after antiviral treatment.
]]> In conclusion, after treating patients with CHB for 48-52 weeks, and after a treatment-free follow-up of 24 weeks to 3 years, the combination of PEG-IFNα and LAM or ADV was not superior to monotherapy with PEG-IFNα in terms of HBsAg seroclearance or seroconversion. More homogeneous original researches are needed to clarify therapeutic efficiency in HBeAg-negative CHB patients, since our results are based only on a clinical report of patients with HBeAg negativity. In future studies, subgroup analyses should mainly be conducted according to HBsAg levels, ALT levels, follow-up duration, and HBV genotype when more homogeneous reports are published.
References
1. Lavanchy D. Hepatitis B Virus epidemiology, disease burden, treatment, and current and emerging prevention and control measures. J Viral Hepat 2004;11:97-107. DOI: 10.1046/j.1365-2893.2003.00487.x. [ Links ]
2. Lok ASF, Mcmahon BJ. AASLD guidelines. Chronic hepatitis B: Update 2009. Hepatology 2009;50:661-2. DOI: 10.1002/hep.23190. [ Links ]
3. European Association for the Study of the Liver. EASL clinical practice guidelines: Management of chronic hepatitis B virus infection. J Hepatol 2012;57:167-85. [ Links ]
4. Li WC, Wang MR, Kong LB, et al. Peginterferon alpha-based therapy for chronic hepatitis B focusing on HBsAg clearance or seroconversion: A meta-analysis of controlled clinical trials. BMC Infect Dis 2011;11:165. DOI: 10.1186/1471-2334-11-165. [ Links ]
5. Huang R, Hao Y, Zhang J, et al. Interferon-alpha plus adefovir combination therapy versus interferon-alpha monotherapy for chronic hepatitis B treatment: A meta-analysis. Hepatol Res 2013;43:1040-51. DOI: 10.1111/hepr.12058. [ Links ]
6. Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control Clin Trials 1996;17:1-12. DOI: 10.1016/0197-2456(95)00134-4. [ Links ]
7. AO FJ, Ma WM, Zhou BP, et al. Comparison of efficacy and safety of pegylated interferon alfa-2a or adefovir dipivoxil monotherapy with combination therapy in HBeAg positive chronic hepatitis B patients. Chin J Infect Dis 2010;28:214-7. [ Links ]
8. Ding WM. Twenty-two chronic hepatitis B patients treated with pegylated interferon and adefovir dipivoxil. Chin J Mod Drug Appl 2010;4:164-5. [ Links ]
9. Liu YH, Wu T, Sun N, et al. Combination therapy with pegylated interferon alpha-2b and adefovir dipivoxil in HBeAg-positive chronic hepatitis B versus interferon alone: A prospective, randomized study. J Huazhong Univ Sci Technolog Med Sci 2014;34:542-7. DOI: 10.1007/s11596-014-1312-2. [ Links ]
10. Chen HO, Liu HJ, Hu XX. Efficacy of adefovir dipivoxil combined with pegylated interferon alfa-2a in treatment of chronic hepatitis B patients with high levels virus load. Chin J Gastroenterol Hepatol 2013;22:456-8. [ Links ]
11. Li WB, Ding JG, Sun QF, et al. Efficacy of pegylated interferon alfa-2a combined with adefovir dipivoxil in treatment of HBeAg positive chronic hepatitis B. Chin J Nosocomiol 2013;23:1250-2. [ Links ]
12. Liang JP, Zhang XM, Xia J, et al. Clinical efficacy of interferons combined with adefovir dipivoxil in treatment of chronic hepatitis B. Chin J Nosocomiol 2013;23:3498-500. [ Links ]
13. Han SY, Rong G, Wang Y. Therapeutic effect of pegylated interferon alpha-2a combined with adefovir dipivoxil in the treatment of HBeAg-positive chronic hepatitis B. China Prac Med 2014;9:1-2. [ Links ]
14. Janssen HL, Van Zonneveld M, Senturk H, et al. HBV 99-01 Study Group; Rotterdam Foundation for Liver Research: Pegylated interferon alfa-2b alone or in combination with lamivudine for HBeAg-positive chronic hepatitis B: a randomized trial. Lancet 2005;365:123-9. DOI: 10.1016/S0140-6736(05)17701-0. [ Links ]
15. Lau GK, Piratvisuth T, Luo KX, et al. Peginterferon alfa-2a HBeAg-positive chronic hepatitis B study group: Peginterferon alfa-2a, lamivudine, and the combination for HBeAg-positive chronic hepatitis B. N Engl J Med 2005;352:2682-95. DOI: 10.1056/NEJMoa043470. [ Links ]
16. Buster EH, Flink HJ, Cakaloglu Y, et al. Sustained HBeAg and HBsAg Loss after longterm follow-up of HBeAg-positive patients treated With peginterferon alpha-2b. Gastroenterology 2008;135:459-67. DOI: 10.1053/j.gastro.2008.05.031. [ Links ]
17. Piccolo P, Lenci I, Demelia L, et al. A randomized controlled trial of pegylated interferon-(alpha)2a plus adefovir dipivoxil for hepatitis B e antigen-negative chronic hepatitis B. Antivir Ther 2009;14:1165-74. DOI: 10.3851/IMP1466. [ Links ]
18. Marcellin P, Lau GK, Bonino F, et al. Peginterferon alfa-2a HBeAg-negative chronic hepatitis B study group: peginterferon alfa-2a alone, lamivudine alone, and the two in combination in patients with HBeAg-negative chronic hepatitis B.N Engl J Med 2004;351:1206-17. DOI: 10.1056/NEJMoa040431. [ Links ]
19. Marcellin P, Bonino F, Lau GK, et al. Peginterferon alfa-2a in HBeAg-negative chronic hepatitis B study group: Sustained response of hepatitis B e antigen-negative patients 3 years after treatment with peginterferon alfa-2a. Gastroenterology 2009;136:2169-79. DOI: 10.1053/j.gastro.2009.03.006. [ Links ]
20. Kaymakoglu S, Oguz D, Gur G, et al. Pegylated interferon alfa-2b monotherapy and pegylated interferon alfa-2b plus lamivudine combination therapy for patients with hepatitis B virus E antigen-negative chronic hepatitis B. Antimicrob Agents Chemother 2007;51:3020-2. DOI: 10.1128/AAC.00088-07. [ Links ]
21. Gish RG, Chang TT, Lai CL, et al. Loss of HBsAg antigen during treatment with entecavir or lamivudine in nucleoside-naive HBeAg-positive patients with chronic hepatitis B. J Viral Hepat 2010;17:16-22. DOI: 10.1111/j.1365-2893.2009.01146.x. [ Links ]
22. Chang TT, Lai CL, KewYoon S, et al. Entecavir treatment for up to 5 years in patients with hepatitis B e antigen-positive chronic hepatitis B. Hepatology 2010;51:422-30. DOI: 10.1002/hep.23327. [ Links ]
23. Heathcote EJ, Marcellin P, Buti M, et al. Three-year efficacy and safety of tenofovir disoproxil fumarate treatment for chronic hepatitis B. Gastroenterology 2011;140:132-43. DOI: 10.1053/j.gastro.2010.10.011. [ Links ]
24. Heathcote EJ, Gane EJ, de Man RA. Long term (4 year) efficacy and safety of tenofovir disoproxil fumarate (TDF) treatment in HBeAg-positive patients (HBeAg+) with chronic hepatitis B (Study 103): preliminary results. Hepatology 2010;52:556A(abstract 477). DOI: 10.1016/S0168-8278(10)61007-0. [ Links ]
25. Boni C, Laccabue D, Lampertico P, et al. Restored function of HBV-specificT cells after long-term effective therapy with nucleos(t)ide analogues. Gastroenterology 2012;143:963-73. DOI: 10.1053/j.gastro.2012.07.014. [ Links ]
26. Zhang JY, Song CH, Shi F, et al. Decreased ratio of Treg cells to Th17 cells correlates with HBV DNA suppression in chronic hepatitis B patients undergoing entecavir treatment. PLoS One 2010; 5:e13869. DOI: 10.1371/journal.pone.0013869. [ Links ]
27. Lin C, Zou H, Wang S. Hepatitis B e antigen seroconversion is related with the function of dendritic cells in chronic hepatitis B virus infection. Gastroenterol Res Pract 2014;2014:413952. [ Links ]
28. Yan W, Wu D, Wang X, et al. Upregulation of NKG2C(+) natural killer cells, TLR-2 expression on monocytes and downregulation of regulatory T-cells influence PEG-IFN treatment efficacy in entecavir-suppressed patients with CHB. Antivir Ther 2015;20:591-602. DOI: 10.3851/IMP2953. [ Links ]
29. Boni C, Lampertico P, Talamona L, et al. Natural killer cell phenotype modulation and natural killer/T-cell interplay in nucleos(t)ide analogue-treated hepatitis e antigen-negative patients with chronic hepatitis B. Hepatology 2015;62:1697-709. DOI: 10.1002/hep.28155. [ Links ]
30. Stelma F, De Niet A, Tempelmans Plat-Sinnige MJ, et al. Natural killer cell characteristics in patients with chronic hepatitis B virus (HBV) infection are associated with HBV surface antigen clearance after combination treatment with pegylated interferon alfa-2a and adefovir. J Infect Dis 2015;212:1042-51. DOI: 10.1093/infdis/jiv180. [ Links ]
31. Xu X, Shang Q, Chen X, et al. Reversal of B-cell hyperactivation and functional impairment is associated with HBsAg seroconversion in chronic hepatitis B patients. Cell Mol Immunol 2015;12:309-16. DOI: 10.1038/cmi.2015.25. [ Links ]
32. Qu LS, Liu JX, Zhang HF, et al. Effect of serum hepatitis B surface antigen levels on predicting the clinical outcomes of chronic hepatitis B infection: A meta-analysis. Hepatol Res 2014 Oct 30. DOI: 10.1111/hepr.12444. [ Links ]
![]() Correspondence: ]]>
Zhongfu Zhao.
Correspondence: ]]>
Zhongfu Zhao.
Institute of Liver Diseases.
Changzhi Medical College.
Jiefang dong Street, 161.
046000 Changzhi, China
e-mail: zhaozf_1226@163.com
Received: 07-09-2015
Accepted: 17-03-2016