CASE REPORTS
Pseudoaneurysm associated with complicated pancreatic pseudocysts
Pseudoaneurisma asociado a pseudoquiste pancreático complicado
Laura Larrey-Ruiz1, Marisol Luján-Sanchis1, Laura Peño-Muñoz1, Carmen Barber-Hueso2, Rafa Cors-Ferrando1, Ana Belén Durá-Ayet1 and Javier Sempere-García-Argüelles1
Departments of 1Digestive Diseases and
2Radiodiagnosis. Consorcio Hospital Universitario de Valencia. Valencia, Spain
ABSTRACT
A pseudoaneurysm associated with a pseudocyst is a serious and unusual complication of chronic pancreatitis. Its treatment is complex due to its elevated mortality and the need for multidisciplinary management. Initial measures consist of locating the hemorrhage through computerized dynamic tomography and arteriography. The treatment of choice is controversial due to the lack of controlled studies. For managing hemorrhages in stable patients, the most accepted initial measure is currently arterial embolization. In the event of failure of the same, hemodynamic instability or the impossibility of drainage of the pseudocyst, surgery is the subsequent therapeutic option.
Key words: Pseudoaneurysm. Pancreatic pseudocyst. Chronic pancreatitis.
RESUMEN
El pseudoaneurisma asociado a pseudoquiste es una complicación grave e infrecuente de la pancreatitis crónica. Su tratamiento es complejo por su elevada mortalidad y la necesidad de un manejo multidisciplinar. La medida inicial consiste en la localización de la hemorragia mediante tomografía computarizada dinámica y arteriografía. El tratamiento de elección es controvertido por la ausencia de estudios controlados. Para el manejo de la hemorragia en pacientes estables, la medida terapéutica inicial más aceptada actualmente es la embolización arterial. Ante fracaso de la misma, inestabilidad hemodinámica o imposibilidad de drenaje del pseudoquiste la cirugía es la siguiente opción terapéutica.
Palabras clave: Pseudoaneurisma. Pseudoquiste pancreático. Pancreatitis crónica.
]]> Introduction
A pseudoaneurysm (PSA) associated with pancreas pseudocyst (PSC) is an uncommon complication that generally occurs in patients with chronic pancreatitis (CP). Its early diagnosis and individualized management are essential given that it can reach mortality rates of up to 24% (10-57%) (1).
To present, the therapeutic strategy for PSA hemorrhages is controversial due to the lack of prospective random trials, as the data available based on very heterogeneous studies is scarce.
The initial management strategy that is most broadly utilized in current clinical practice consists of the localization of the hemorrhage through abdominal dynamic computerized tomographies (CT) and arteriography, following therapeutic artery embolization (AE) (2).
We present a complicated case of CP with PSA associated with PSC (PSC-PSA) that we consider to be of interest due to the confluence in one patient of all the complications that this entity may cause; the complex diagnostic process, which included endoscopic ultrasound; and the therapeutic process, which was carried out in a pathological process that was serious, and that finally ended successfully.
Case Report
This case was of a 40-year-old man with a history of CP of toxic origin (tobacco, alcohol and cocaine) complicated by PSC in the head of the pancreas, known for the last nine months, who came to the Emergency Room of the clinic over three days, with epigastric abdominal pain radiating to both hypochondria with growing intensity and without other associated symptomatology. Upon examination, the patient presents a regular general state, an under-nourished appearance and upon abdominal palpation, a sensation of painful occupation in the epi-mesogastrium, without signs of peritoneal irritation.
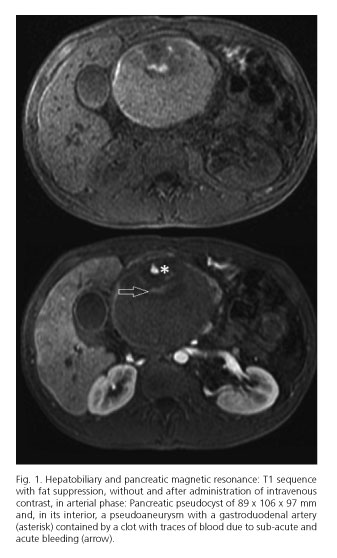
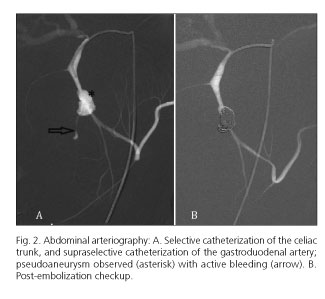
During admission, medical treatment is begun with good progress in terms of pain, but presents progressive cutaneous-mucous jaundice, and a magnetic resonance (MR) is thus indicated for the Hepatobiliary and pancreatic area with cholangiography (Fig. 1) objectivizing PSC with a known increase in size, producing extrinsic compression of the extrahepatic bile duct and in its interior, PSA, caused by a gastroduodenal artery contained by a clot with remnants of blood due to acute and sub-acute bleeding. An arteriography is ordered, showing the PSA of the gastroduodenal artery with active bleeding in the interior of the PSC, and a supra-selective AE is performed on the same via metallic spirals (coils), without incident (Fig. 2)
]]>
After five days, the AE presents melena and anemization without hemodynamic repercussion. An endoscopic ultrasound (EUS) is performed, showing traces of blood in the gastric cavity and a large cystic collection reaching from the posterior face of the gastric body to the second duodenal portion. On the posterior face of the bulb, there is a small ulceration on a rounded and pulsing mucosa suggestive of corresponding to the fistulization of the PSC-PSA, which is confirmed by the presence of arterial flow in Doppler mode (Fig. 3). An urgent arteriography is performed in which there are several pseudoaneurysmal formations dependent on the PSA, previously treated proceeding to the AE with coils of the same.

Following the new AE, the patient continues to be clinically and hemodynamically stable, with significant cutaneous-mucous depigmentation 48 hours after the spontaneous drainage of the PSC, pending a scheduled surgical operation. However, four days after the second AE, the patient presents hematemesis and rectal bleeding with hemodynamic compromise, requiring urgent surgical operation. During the same, an active digestive hemorrhage is shown with a discharge of blood through pylorus from the PSC. A cystic gastrostomy is performed, suture of the gastroduodenal artery and its collaterals. Following the same, an antrectomy is completed, with Billroth II-type reconstruction.
The patient presents favorable progress with clinical and analytical stability in the post-operative phase and up until the current day.
]]>Discussion
The occurrence of spontaneous hemorrhage of a PSC is very low (1.4-8.4%), this being in prospective series with follow-up during more than 10 years, approximately 6% (3) and in retrospective series of 8 years of 10.4% (1).
Regarding the PSC-PSA, as in the case of our patient, there are very few published cases, and they should be differentiated from the simple isolated pancreatic PSAs, without PSC that have been described in 10% of the cases of pancreatitis evaluated through arteriography (1). In the majority of these, the characteristics of the patients are similar to ours, young (around 39-45 years of age) who frequently present a CP underlying the alcoholic etiology, although this can also happen in 3.5-10% of acute pancreatitis (4). The most frequent form of presentation is manifest gastrointestinal bleeding (> 80% of cases), although it can also present itself as abdominal pain or jaundice (5).
The three possible mechanisms described in the formation of PSA of the pancreas are: serious swelling and/or enzymatic self-digestion of pancreatic or peri-pancreatic arteries; the transfer of an established PSC in a peri-pancreatic vessel, which becomes a large PSA; and a PSC which erodes the intestinal wall and produces digestive bleeding (2). All three situations coincided in our case.
The arteries involved with greatest frequency by decreasing order are the spleen artery (40%), followed by the gastro-duodenal artery (30%), the pancreatic duodenal artery (20%), the gastric (5%), and the hepatic arteries (2%) (6,7).
The early diagnosis of the PSA is key to scheduling the most efficient treatment. The technique of choice is arteriography, which offers 100% sensitivity for its detection (8%). Other Methods help a diagnosis of suspected CT which allow the elimination of other complications associated with CP (9) or EUS, with Doppler being useful in the evaluation of peri-pancreatic liquid collections and its complications, such as aneurysms or pseudoaneurysms upon observing a flow with an arterial pattern within a collection (10).
The handling of the PSA-PSC is complex given the high morbi-mortality associated with the same. The AE and the surgery are currently the most used therapeutic strategies, such as we performed in our case, and which are considered to be complementary treatments. The AE is recommended as an initial approach in hemodynamically stable patients and represents the treatment of choice in 80% of cases (11,12).
The majority of PSA-PSC in CP can be treated successfully and safely through a combination of radiological obliteration of the PSA and subsequent trans-papillary endoscopic drainage of the PSC through an ERCP (5). On other occasions, the ERCP is not necessary, such as in our case, because a spontaneous drainage of the PSC occurs to the digestive tract (13).
The surgery should be reserved for those cases with an active hemorrhage; in the case of hemodynamic instability; when the AE is not possible or fails (such as with our patient); if the endoscopic care of the PSC is unsuccessful; when the hemorrhage proceeds to the pancreatic tail; and in the case of applications, such as infection or extrinsic compression (1,4,14). However, other authors recommend early surgical intervention following the AER to avoid re-bleeding (1,2,12). In our case, re-bleeding occurred a few days after the AE and required a second embolization while waiting for the surgery to be scheduled.
]]> If the hemorrhage caused by PSA is located in the pancreatic tail or a free hemorrhage occurs in the peritoneal cavity, removal is the most utilized procedure, while for lesions located on the head or body of the pancreas, more conservative surgical procedures are recommended (12,15).In conclusion, we present this case of PSC in a patient with CP which presented several serious complications that required multidisciplinary care with satisfactory resolution. It began with a digestive clinic secondary to its increase in size, and the formation of a PSA required an AE due to intra-cystic hemorrhage. Subsequently, the patient presented digestive hemorrhaging secondary to fistulization of the PSC to the digestive tract, along with post-embolization relapse of the PSA which required a second AE, and both of which were resolved through a definitive surgery.
References
1. Bender JS, Bouwman DL, Levison MA, et al. Pseudocysts and pseudoaneurysms: surgical strategy. Pancreas 1995; 10: 143-7. [ Links ]
2. Chiang KC, Chen TH, Hsu JT. Management of chronic pancreatitis complicated with a bleeding pseudoaneurysm. World J Gastroenterol 2014; 20: 16132-7. DOI: 10.3748/wjg.v20.i43.16132. [ Links ]
3. Carr JA, Cho JS, Shepard AD, et al. Visceral pseudoaneurysms due to pancreatic pseudocysts: rare but lethal complications of pancreatitis. J Vasc Surg. 2000; 32: 722-30. DOI: 10.1067/mva.2000.110055. [ Links ]
]]>4. O'Connor OJ, Buckley JM, Maher MM. Imaging of the complications of acute pancreatitis. AJR Am J Roentgenol. 2011; 197: W375-81. DOI:10.2214/AJR.10.4339. [ Links ]
5. Bhasin DK, Rana SS, Sharma V, et al. Non-surgical management of pancreatic pseudocysts associated with arterial pseudoaneurysm. Pancreatology 2013; 13: 250-3. DOI: 10.1016/j.pan.2013.02.011. [ Links ]
6. Mallick IH, Winslet MC. Vascular complications of pancreatitis. JOP 2004; 5: 328-37. [ Links ]
7. Balachandra S, Siriwardena AK. Systematic appraisal of the management of the major vascular complications of pancreatitis. Am J Surg 2005; 190: 489-95. DOI: 10.1016/j.amjsurg.2005.03.009. [ Links ]
8. Hsu JT, Yeh CN, Hung CF, et al. Management and outcome of bleeding pseudoaneurysm associated with chronic pancreatitis. BMC Gastroenterology 2006; 6: 3. DOI: 10.1186/1471-230X-6-3. [ Links ]
]]>9. Balthazar EJ, Fisher LA. Hemorrhagic complications of pancreatitis: radiologic evaluation with emphasis on CT imaging. Pancreatology 2001; 1: 306-13. DOI: 10.1159/000055829. [ Links ]
10. Fukatsu K, Ueda K, Maeda H, et al. A case of chronic pancreatitis in which endoscopic ultrasonography was effective in the diagnosis of a pseudoaneurysm. World J Gastrointest Endosc 2012; 4: 335-8. DOI: 10.4253/wjge.v4.i7.335. [ Links ]
11. Vázquez J, Mansilla D, Civera JF, et al. Therapeutic options in pancreatic pseudoaneurysms. Rev Esp Enferm Dig 2012; 104: 502-3. [ Links ]
12. Udd M, Leppäniemi AK, Bidel S, et al. Treatment of bleeding pseudoaneurysms in patients with chronic pancreatitis. World J Surg 2007; 31: 504-10. DOI: 10.1007/s00268-006-0209-z. [ Links ]
13. Azcano E, Álvarez CJ, Irurzun J, et al. Gastrointestinal bleeding due to pseudoaneurism with spontaneous pancreatic pseudocyst drainage. Rev EspEnferm Dig 2008; 100; 179-87. [ Links ]
]]>14. Pang TC, Maher R, Gananadha S, et al. Peripancreatic pseudoaneurysms: a management based classification system. Surg Endosc 2014; 28: 2027-38. DOI: 10.1007/s00464-014-3434-9. [ Links ]
15. Chong CN, Lee KF, Wong KT, et al. Ruptured gastroduodenal artery pseudoaneurysm as the initial presentation of chronic pancreatitis. Am J Surg 2009; 197: e38-40. DOI: 10.1016/j.amjsurg.2008.05.014. [ Links ]
![]() Correspondence:
Correspondence:
Laura Larrey-Ruiz.
Department of Digestive Diseases.
Consorcio Hospital General Universitario de Valencia. ]]>
Av. Tres Cruces no2.
46014 Valencia, Spain
e-mail: larrey.laura@gmail.com
Received: 20/05/2015
Accepted: 08/06/2015