Regression of gastric intestinal metaplasia after the eradication of Helicobacter pylori infection in a hospital in Mexico
Regresión de la metaplasia intestinal gástrica tras la erradicación de la infección por Helicobacter pylori en un hospital de México
Jaime Alberto Sánchez-Cuén1,2, Ana Bertha Irineo-Cabrales1,2, Gregorio Bernal-Magaña1 and Felipe de Jesús Peraza-Garay3
1Department of Digestive Diseases. Hospital Regional del Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado. Culiacán, Sinaloa. Mexico.
2Department of Postgraduate Studies. School of Medicine. Universidad Autónoma de Sinaloa. Culiacán, Sinaloa. Mexico.
3Centro de Investigación y Docencia en Ciencias de la Salud. Universidad Autónoma de Sinaloa. Culiacán, Sinaloa. Mexico
ABSTRACT
Background: Intestinal metaplasia is a precursor lesion of gastric cancer. Infection by Helicobacter pylori is the principal cause of metaplasia. While evidence of the regression of metaplasia after treatment to eradicate this infection has been demonstrated, controversy remains with regard to this subject.
Objective: The objective of this study was to determine the frequency of the regression of gastric intestinal metaplasia one year after the eradication of Helicobacter pylori.
Methods: A prospective longitudinal designed study was carried out. The population studied in this research consisted of patients attending the Endoscopy Unit to undergo an upper endoscopy, in whom various symptoms indicated intestinal metaplasia associated with Helicobacter pylori, and who received standard empiric triple therapy to eradicate the bacteria. An upper endoscopy was performed in which four gastric biopsy samples were taken (two from the antrum and two from the body) before and after the eradicating treatment, with the endoscopic and histological findings studied after one year of monitoring. The statistical analysis was conducted using the Fisher's exact test and the McNemar's test.
Results: Forty-six patients were studied, of whom 20 (43.5%) were men and 26 (56.5%) were women, with an average age of 58.9 (DE 11.2). Intestinal metaplasia was found in 46 (100%) patients before treatment and in 21 (45.7%) patients post-eradication. Complete intestinal metaplasia (type I) was found in 35 patients (76.1%) before treatment and in 11 (23.9%) patients post-eradication (p = 0.000), while incomplete intestinal metaplasia (type II) was found in 10 (21.7%) patients before treatment and in 10 (21.7%) patients post-eradication. Non-atrophic chronic gastritis was found in 35 (76.1%) patients before treatment and in 32 (69.6%) patients post-eradication.
Conclusions: In this study, gastric intestinal metaplasia associated with Helicobacter pylori infection showed a regression of 54.3% one year after the eradication of this microorganism. This treatment could modify the natural history of the development of gastric cancer.
Key words: Metaplasia. Helicobacter pylori. Precancerous lesions.
Introducción: la metaplasia intestinal es una lesión precursora del cáncer gástrico. La infección por Helicobacter pylori es la principal causa de metaplasia. Aunque se ha demostrado evidencia de regresión de metaplasia intestinal tras el tratamiento erradicador de esta infección, aún existen controversias al respecto.
Objetivo: el objetivo de este estudio fue determinar la frecuencia de la regresión de la metaplasia intestinal gástrica al año de haber erradicado Helicobacter pylori.
Métodos: se realizó un diseño prospectivo, longitudinal. La población estudiada fueron pacientes que acudieron a la Unidad de Endoscopia para la realización de una endoscopia digestiva alta por distintas indicaciones, comprobándose metaplasia intestinal asociada a Helicobacter pylori, y que recibieron terapia triple estándar empírica con erradicación de la bacteria. Se realizó una endoscopia digestiva alta con toma de cuatro muestras de biopsias gástricas (dos en antro y dos en cuerpo) antes y después del tratamiento erradicador, estudiándose los hallazgos endoscópicos e histológicos al año de seguimiento. Análisis estadístico con prueba exacta de Fisher y McNemar.
Resultados: fueron estudiados 46 pacientes, 20 (43,5%) hombres y 26 (56,5%) mujeres, con edad media de 58,9 (DE 11,2) años. Se encontró metaplasia intestinal en 46 (100%) pacientes antes del tratamiento y en 21 (45,7%) tras la erradicación; metaplasia intestinal completa (tipo I) en 35 pacientes (76,1%) antes del tratamiento y en 11 (23,9%) posterior a la erradicación (p = 0,000); metaplasia intestinal incompleta (tipo II) en 10 (21,7%) pacientes antes del tratamiento y en 10 (21,7%) posterior a la erradicación; y gastritis crónica no atrófica en 35 (76,1%) pacientes antes del tratamiento y en 32 (69,6%) pacientes posterior a la erradicación.
Conclusiones: en este estudio la metaplasia intestinal gástrica asociada a la infección por Helicobacter pylori presentó una regresión al año del 54,3% posterior a la erradicación de este microorganismo. Este tratamiento podría modificar la historia natural del desarrollo del cáncer gástrico.
Palabras clave: Metaplasia. Helicobacter pylori. Lesiones precancerosas.
Introducción
Helicobacter pylori (H. pylori) infection is common, with a global prevalence of more than 50% and distinct geographical variations (1). When H. pylori colonize the stomach, the initial immune response of the gastric mucosa varies considerably according to the virulence of the strain (2). Reports describe an evolving succession of pre-neoplasic lesions (atrophic gastritis, intestinal metaplasia, displasia) developing from H. pylori infection and the development of gastric cancer (3). In the initial pre-cancerous lesion, atrophic gastritis is characterized by the death of the parietal cells and the loss of the glandular epithelium that covers the mucosa of the stomach (4). Intestinal metaplasia involves the replacement of glandular and/or foveolar epithelium by intestinal epithelium and is characterized by its morphological similarity to enterocytes. There are many classifications for intestinal metaplasia, with no universally accepted classification. Histopathological and histochemical studies have identified two types of metaplasia: type I, or complete, which is characterized by the presence of non-secretory absorption cells with well delineated brush-borders, Paneth cells, and cells that secrete sialomucins, and which corresponds to a phenotype from the small intestine; and type II, or incomplete or colonic, including types IIA and IIB, which are characterized by the presence of columnar cells and cells which secrete sialomucins (type IIA) and sulphomucins (type IIB) (5). Intestinal metaplasia is associated with H. pylori infection and bile reflux, although H. pylori is cited as the principal cause of metaplasia (6,7).
]]> Some studies have demonstrated the following as risk factors for developing intestinal metaplasia: an age of ≥ 61, H. pylori infection, the ingestion of spicy food, a history of smoking (8), male gender, a family history of gastric cancer, a below-university educational level, the consumption of dairy products (9), and dietary factors, such as excessive salt consumption, deficient ascorbic acid, and insufficient ingestion of carotene (10). However, among the risk factors, H. pylori infection is considered to be the most significant risk factor for intestinal metaplasia (11). As few studies have been conducted that estimate the prevalence of intestinal metaplasia in the general asymptomatic population, it is necessary to carry out an upper endoscopy and a histological examination. The prevalence of intestinal metaplasia varies from 7.1% to 42.5% depending on country and diagnostic method (12).Controversy has arisen with regard to the impact of the eradication of H. pylori and the risk of gastric carcinoma. There is evidence of the regression of precancerous lesions such as intestinal metaplasia after the eradication treatment (13). However, although some authors have observed a regression of gastric atrophy and low grade dysplasia (14), the reversibility of the intestinal metaplasia continues to be controversial (15,16). The objective of this study was to determine the frequency with which gastric intestinal metaplasia regresses one year after the eradication of H. pylori infection.
Material and methods
This research consisted of a longitudinal and prospective quasi-experimental study, with pre and post-test readings taken from solely one group. Approved by the Commission for Research and Ethics at the Hospital Regional of the Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado, or ISSSTE, in Culiacán, Sinaloa, this study did not violate concepts of authorship, plagiarism, conflict of interests, or informed consent.
This research studied a population of adult patients attending the Endoscopy Unit to undergo an upper endoscopy for various symptoms (a dyspepsia test, gastrointestinal bleeding, anemia, and dysphagia, among others), and in whom the presence of gastric metaplasia associated with H. pylori infection has been identified. All the patients included in the study were treated with standard empiric triple therapy (40 mg omeprazole, 500 g clarithromycin, and 1 g amoxicillin, twice daily for two weeks). The study was conducted at the Department of Digestive Diseases at the ISSSTE Hospital Regional in the city of Culiacan, Sinaloa, in Northeastern Mexico, from June 2013 to June 2015. The patients were monitored for one year, with an upper endoscopy conducted one year after the eradication of H. pylori, and the findings of the stomach endoscopy were evaluated, as were the findings of the histological analysis performed on the gastric mucosa. The inclusion criteria were: both male and female subjects, aged between 30 and 80, in whom the eradication of H. pylori had been confirmed using the carbon-14 urea breath test and who had provided their informed consent. The exclusion criteria included patients with a history of two or more treatments for the eradication of H. pylori infection, pregnant women, and patients with a history of gastrointestinal surgery or a diagnosis of gastric cancer. The elimination criteria included patients who had not been monitored for a year, patients for whom the presence of H. pylori bacillus had been confirmed via histology during monitoring, and patients with errors in data collection.
Definition of the variables
The histological and endoscopic findings of the gastric mucosa and H. pylori infection were defined according to the Sidney system (18-21). Gastric intestinal metaplasia was defined according to the Filipe and Jass classification (5). Gastrointestinal bleeding was defined according to the Forrest classification (22).
Sample
The sample size was set at 49 patients, a power of 80% to detect a difference among the hypothetical proportions and the alternative of 0.20 (Delta) was calculated. The proportion for the null hypothesis was 0.30, assumed by the review of a Spanish study (17), and under the alternative hypothesis of 0.50. The bilateral (two tails) Z test was applied with a level of significance of 0.05, with a 10% expected patient loss. Due to convenience and the number of consecutive patients, the type of sampling was not probabilistic.
]]> Collection of dataThe data were collected from a primary source via the direct observation of the stomach (fundus, body and antrum) via two gastric antrum samples, and two body samples taken via an upper video endoscopy, as well as findings from the histological study of the gastric mucosa samples.
Equipment management, biological samples
Upper endoscopy techniques and gastric biopsies
Oropharyngeal lidocaine spray was applied in a left lateral decubitus position and a mouthpiece was placed. The endoscopy was performed under intravenous sedation using an Olympus EG 29-90I video endoscope. The macroscopic characteristics of the stomach were registered. Four biopsies were taken (two in the antrum and two in the body) using FB 25K-1 series biopsy forceps. The endoscopies were evaluated by two endoscopy specialists.
Identification of gastric intestinal metaplasia
Histological study
The gastric mucosa biopsies (two from the antrum and two from the body) were processed using standard paraffin techniques with histological sections colored with hematoxylin and eosin and Giemsa stain. Complementary stains with toluidine blue were used, with a sensitivity and specificity of 96 and 99, respectively (23). The sections were then evaluated by two pathologists. Type I metaplasia was identified by the presence of non-secretory absorption cells with well delineated brush-borders and Paneth cells (enterocytes), while the presence of columnar cells were used to identify type II (24).
Identification of H. pylori in gastric biopsy samples
Histological studies were performed with sections colored with hematoxylin and eosin, according to the criteria from the modified Sydney system and Giemsa stain (23).
]]> Statistical analysisThe data were analyzed with the SPSS v 16 software package (SPSS, Inc., Chicago IL, USA). Average and standard deviation were used for the quantitative variables, while the categorical variables were presented as frequencies and percentages. The Fisher's exact test and the McNemar's test with binomial distribution were used. The data are presented in tables and figures. A p value of 0.05 was considered as significant.
Results
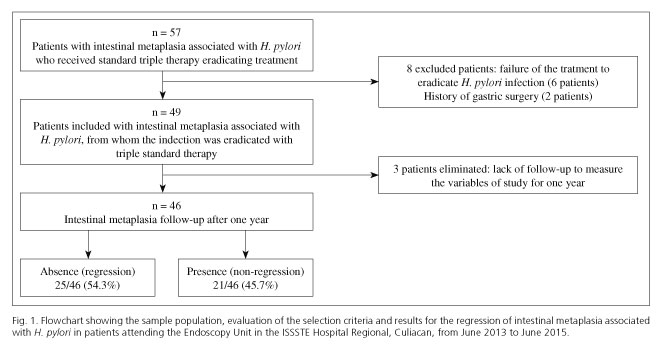
Of the 359 patients that underwent an upper endoscopy, 79 (22%) patients presented with intestinal metaplasia, 57 patients had metaplasia associated with H. pylori, 8 patients were excluded, 49 patients were included in the study, and 3 patients were finally eliminated (Fig. 1).
The average age of the patients was 58.9 (DE 11.2), of whom 20 (43.5%) were men and 26 (56.5%) were women (p = 0.207). Fifteen (32.6%) patients were referred from Primary Care, and 31 (67.4%) patients from the area of medical specialties (p = 0.002). With regard to educational level, 20 (43.5%) patients had a higher educational level and 26 (56.5%) patients had a basic or secondary level of education (p = 0.404).
The indications for upper endoscopy to be performed were dyspepsia tests in 33 (71.7%) patients, the consumption of non-steroid anti-inflammatory medication in 5 (10.8%) patients, a history of intestinal bleeding in 4 (8.7%) patients, iron-deficiency anemia in 2 (4.3%) patients and dysfagia in tests conducted on 2 (4.3%) patients.
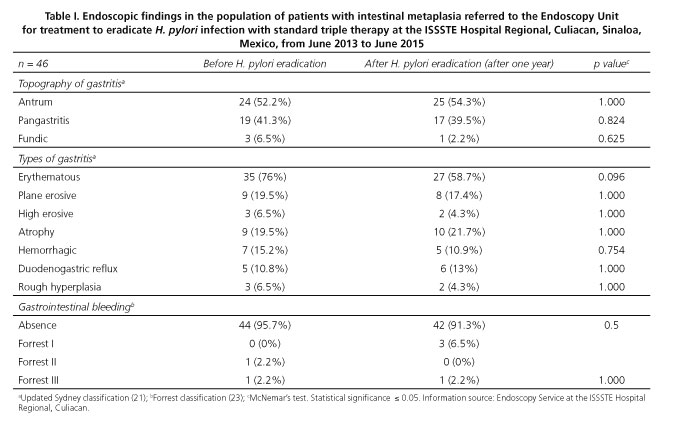
]]> Of the 57 patients who presented metaplasia associated with H. pylori and who were treated with standard triple therapy, the bacteria was not eradicated in 6 patients, resulting in an eradication rate of 89.4% (Fig. 1).There was no significant difference in the endoscopic findings from the gastric mucosa in terms of their topography, type of gastritis and intestinal bleeding both before treatment and after the eradication of H. pylori (p > 0.05) (Table I).
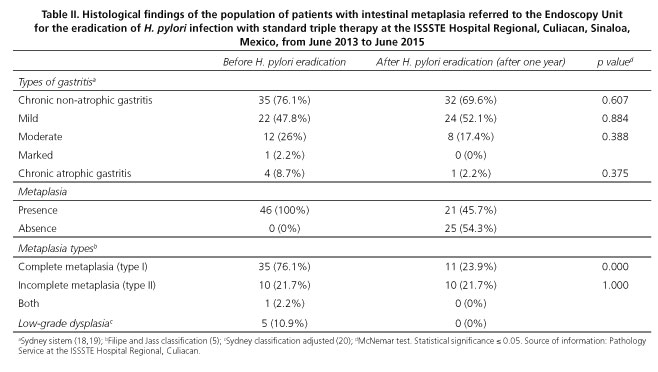
The most frequent histological finding was chronic non-atrophic gastritis, which occurred in 35 (76.1%) patients before treatment and in 32 (69.6%) patients after treatment to eradicate H. pylori. No significant difference was found between the histological findings for atrophic and non-atrophic chronic gastritis both before and after treatment to erradiacte H. pylori (p > 0.05). Intestinal metaplasia was present in 46 (100%) patients before and in 21 (4.7%) patients after treatment to eradicate H. pylori. In 25 (54.3%) patients intestinal metaplasia was absent after the eradication of H. pylori. Complete intestinal metaplasia (type I) was present in 35 (76.1%) patients before and in 11 (23.9%) patients after the eradication of H. pylori (p = 0.000). Incomplete intestinal metaplasia (type II) was present in 10 (21.7%) patients before and after treatment to eradicate H. pylori (p = 1.000). Low grade dysplasia was present in 5 (10.9%) patients before treatment to eradicate H. pylori and was not present after treatment (Table II).
The regression of intestinal metaplasia was observed one year after the eradication of H. pylori in 11 (55%) men and in 14 (53.8%) women (p = 0.588). Similarly, a regression of metaplasia was observed, after the eradication of H. pylori, in 15 (57.7%) of the patients with a basic or secondary educational level, compared to the 10 (50%) patients (p = 0.766) who had received higher education. The average age of the patients in whom the regression of metaplasia was observed was 58.5 (DE 12) years, compared to an average age of 59.4 (DE 10.4) (p = 0.768) in patients with no regression of the metaplasia after the eradication of H. pylori.
]]>Discussion
Gastric intestinal metaplasia is a precursor lesion of gastric cancer, histological analysis shows the reduction or loss of the glandular component as it is replaced by enterocytes, and caliciform and Paneth cells. The Pelayo Correa "cascade" describes a sequence of histological lesions leading to the possible development of gastric cancer, beginning with chronic gastritis and evolving into chronic atrophic gastritis, intestinal metaplasia, dysplasia, and finally, cancer (2). The most important environmental factor related to the development of gastric intestinal metaplasia is H. pylori infection. In this study, the regression of intestinal metaplasia was observed in 25 (54.3%) patients one year after the eradication of H. pylori, a regression which was present preferentially in patients with type I metaplasia (complete). All 5 (10.9%) patients with low grade dysplasia from the population studied presented regression of the lesion before the eradication of H. pylori, although the results must be analyzed with caution given the reduced sample size included in the study.
While gastric intestinal metaplasia is prevalent, ranging from 7.1% to 42.5% in various countries around the world, it was found at a frequency of 22% in this study. The regression of gastric intestinal metaplasia subsequent to the eradication of H. pylori is clinically significant and represents an opportunity for the prevention of gastric cancer, which continues to be a public health problem. Moreover, prognosis is poor when this type of cancer is diagnosed in advanced stages despite treatment attempts, so the early detection of pre-neoplasic gastric lesions is important in at-risk patients, as well as monitoring and eradicating H. pylori. There is some controversy with regard to the type of pre-cancerous lesions that might lead to the evolution of gastric adenocarcinoma. Thus, González et al. (25) undertook a prospective study in 478 patients, monitored over the course of several years, who had been diagnosed with a type of pre-cancerous gastric lesion. They observed that a family history of gastric cancer and type II intestinal metaplasia (incomplete) were risk factors for progression to gastric adenocarcinoma. In this study, the regression of intestinal metaplasia type II (incomplete) was not observed in the patients when H. pylori had been eradicated.
In previous studies, various authors monitored patients with gastric intestinal metaplasia who were undergoing treatment to eradicate H. pylori, in order to evaluate the regression of the lesion. Monés et al. (26) presented a study of 37 patients with gastric intestinal metaplasia, and observed 100% regression of the lesion. Vázquez Romero et al. (17) studied 71 patients; in 50 (29.6%) of them the lesion regressed. Massarrat et al. (27) studied 30 patients, observing regression in 10 (21.7%) patients.
The discrepancies among the results described above could be related to the distinct designs of the various studies, the different methods for evaluating the grade of atrophy, the different number of gastric samples obtained, the number of patients included, the different monitoring times, the distinct strains of infectious H. pylori identified, and the types and number of treatment strategies used to eradicate H. pylori.
With regard to the endoscopic findings of this study, no significant difference was observed in the behavior of gastritis, in terms of type and topography, during the disease monitoring conducted a year after eradication treatment in this study (p > 0.05). No association was found between the regression of intestinal metaplasia and age, gender and educational level of the patients studied (p > 0.05).
The main limitations of this study include the fact that it did not determine the density of H. pylori, gastric biopsies were not taken from the angular incisure, and types IIA and IIB gastric intestinal metaplasia were not identified by histochemistry. Another limitation was not performing chromoendoscopy tests, which are more sensitive and thus precise for the identification of areas with metaplasia or dysplasia in the gastric mucosa. The methodology used in this study did not use a control group, which limited the ability of the research to establish evidence that the changes observed were due to the treatment being evaluated. However, this was a prospective study, and the data collection method used facilitated the control of the variables, while monitoring of the patients in the study enabled us to ensure losses of no more than 5% of the total sample population studied.
It can be concluded from this research that gastric intestinal metaplasia associated with H. pylori infection presented a 54.3% regression rate in those patients attending an endoscopy unit one year after their infection had been eradicated via standard triple therapy. The eradication of this micro-organism could modify the natural history of the progression of lesions in the gastric mucosa and their evolution into gastric carcinoma.
]]> Acknowledgments
We would like to acknowledge the technical support received from the endoscopy service and the Pathological Anatomy service at the ISSSTE Regional Hospital, Culiacan.
References
1. Suerbaum S, Michetti P. Helicobacter pylori infection. N Engl J Med 2002;347:175-86. DOI: 10.1056/NEJMra020542. [ Links ]
2. Correa P, Piazuelo MB, Camargo MC. Etiopathogenesis of gastric cancer. Scand J Surg 2006;95:218-24. [ Links ]
3. Conteduca V, Sansonno D, Lauletta G, et al. H. pylori infection and gastric cancer: State of the art (review). Int J Oncol 2013;42:5-18. [ Links ]
]]>4. Fuentes-Pananá E, Camorlinga-Ponce M, Maldonado-Bernal C. Infection, inflammation and gastric cancer. Salud Publica Mex 2009;51:427-33. DOI: 10.1590/S0036-36342009000500010. [ Links ]
5. Jass JR, Filipe MI. The mucin profiles of normal gastric mucosa, intestinal metaplasia and its variants and gastric carcinoma. Histochem J 1981;13:931-9. DOI: 10.1007/BF01002633. [ Links ]
6. Quingalahua Flores Aldo, Mendoza Jaime Francisco. Helicobacter pylori, metaplasia intestinal de estómago y cáncer gástrico. Oncología 2004;14:64-7. [ Links ]
7. Piñol Jiménez F, Paniagua Estévez M, Pérez Sánchez G, et al. Metaplasia intestinal en pacientes con reflujo duodenogástrico y ácidos biliares totales elevados. Rev Cubana Med 2010;49:17-32. [ Links ]
8. Kim N, Park YS, Cho SI, et al. Prevalence and risk factors of atrophic gastritis and intestinal metaplasia in a Korean population without significant gastroduodenal disease. Helicobacter 2008;13:245-55. DOI: 10.1111/j.1523-5378.2008.00604.x. [ Links ]
]]>9. Joo YE, Park HK, Myung DS, et al. Prevalence and risk factors of atrophic gastritis and intestinal metaplasia: A nationwide multicenter prospective study in Korea. Gut Liver 2013;7:303-10. DOI: 10.5009/gnl.2013.7.3.303. [ Links ]
10. Correa P. Human gastric carcinogenesis: A multistep and multifactorial process - First American Cancer Society Award Lecture on Cancer Epidemiology and Prevention. Cancer Res 1992;52:6735-40. [ Links ]
11. Kim N, Park RY, Cho SI, et al. Helicobacter pylori infection and development of gastric cancer in Korea: Long-term follow-up. J Clin Gastroenterol 2008;42:448-54. DOI: 10.1097/MCG.0b013e3180 46eac3. [ Links ]
12. Park YH, Kim N. Review of atrophic gastritis and intestinal metaplasia as a premalignant lesion of gastric cancer. J Cancer Prev 2015;20:25-40. DOI: 10.15430/JCP.2015.20.1.25. [ Links ]
13. A review of human carcinogens. B. Biological agents. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Lyon, 24 February-3 March 2009. IARC Monogr Eval Carcinog Risks Hum 2012;100:385-423. [ Links ]
]]>14. Micu G, Stăniceanu F, Zurac S, et al. Regression of precancerous epithelial alteration in patients with Helicobacter pylori chronic gastritis. Rom J Intern Med 2010;48:89-99. [ Links ]
15. Lahner E, Bordi C, Cattaruzza MS, et al. Long term follow-up in atrophic body gastritis patients: Atrophy and intestinal metaplasia are persistent lesions irrespective of Helicobacter pylori infection. Aliment Pharmacol Ther 2005;22:471-81. DOI: 10.1111/j.1365-2036.2005.02582.x. [ Links ]
16. Wang J, Xu L, Shi R, et al. Gastric atrophy and intestinal metaplasia before and after Helicobacter pylori eradication: A meta-analysis. Digestion 2011;83:253-60. DOI: 10.1159/000280318. [ Links ]
17. Vázquez Romero M, Boixeda de Miquel D, Valer López-Fando MP, et al. Intestinal metaplasia: Evolution after Helicobacter pylori eradication and influence in the success of eradicating therapy. Rev Esp Enferm Dig 2003;95:781-4. [ Links ]
18. Correa P, Bravo L. Investigaciones sobre cáncer gástrico en Nariño. Rev Med Hospital Universitario Departamental de Nariño 2007;3:6-12. [ Links ]
]]>19. Correa P, Piazuelo MB. The gastric precancerous cascade. J Dig Dis 2012;13:2-9. DOI: 10.1111/j.1751-2980.2011.00550.x. [ Links ]
20. Salas Caudevilla A. Evaluation of dysplasia in gastrointestinal diseases. Gastroenterol Hepatol 2007;30:602-11. DOI: 10.1157/13112598. [ Links ]
21. Valdivia Roldán M. Gastritis and gastropathies. Rev Gastroenterol Perú 2011;31:38-48. [ Links ]
22. Peetsalu A, Kirsimägi U, Peetsalu M. Giant peptic ulcer hemorrhages: Epidemiology, treatment, and outcome in the teaching hospital of Tartu. Medicina (Kaunas) 2011;47(1):19-24. [ Links ]
23. Abdo-Francis JM, Uscanga-Domínguez LF, Sobrino-Cossio S, et al. Tercer consenso mexicano de Helicobacter pylori. Rev Gastroenterol Mex 2007;72(3):321-38. [ Links ]
]]>24. Calle Astudillo G, Jerves T, Pesántez L, et al. Utility of routine gastric biopsies and staining with methylene blue in the diagnosis of intestinal metaplasia in patients over 40 years. Acta Gastroenterol Latinoam 2013;43(3):189-97. [ Links ]
25. González CA, Pardo ML, Liso JM, et al. Gastric cancer occurrence in preneoplastic lesions: A long-term follow-up in a high-risk area in Spain. Int J Cancer 2010;127:2654-60. DOI: 10.1002/ijc.25273. [ Links ]
26. Monés J, Rodrigo L, Sancho F, et al. Helicobacter pylori eradication versus one-year maintenance therapy: Effect on relapse and gastritis outcome. Rev Esp Enferm Dig 2001;93(6):372-89. [ Links ]
27. Massarrat S, Haj-Sheykholeslami A, Mohamadkhani A, et al. Precancerous conditions after H. pylori eradication: A randomized double blind study in first degree relatives of gastric cancer patients. Arch Iran Med 2012;15(11):664-9. [ Links ]
]]>
Received: 13-01-2016
Accepted: 03-06-2016