
Un Programa para la Mejora de las Relaciones Padres-Hijos. La Terapia de Interacción Padres-Hijos
Anthony J. Urquiza y Susan Timmer
University of California at Davis Children's Hospital, USA
ABSTRACT
]]> Disruptive child behavior problems are common problems for parents and can be associated with serious delinquent behaviors and aggressive/violent behaviors in adolescence and adulthood. Parenting interventions to address disruptive child behavior problems has gained widespread acceptance. One of these parenting interventions is Parent-Child Interaction Therapy (PCIT). PCIT is a 14- to 20-week, founded on social learning and attachment theories, designed for children between 2 and 7 years of age with disruptive, or externalizing, behavior problems. This article will provide a brief review of the history of PCIT, a description of the basic components of PCIT, and an overview of recent developments that highlight the promise of PCIT with maltreating parent-child relationships, traumatized children, and in developing resilience in young children. In addressing the three basic treatment objectives for PCIT (i.e., reduction in child behavior problems, improving parenting skills, enhancing the quality of parent-child relationships), there is an abundance of research demonstrating very strong treatment effects and therefore, its value to the field. Recent research has also demonstrated the value of PCIT in reducing trauma symptoms in young children.Keywords: behavior problems, Parent-Child Interaction Therapy, parenting skills, treatment.
RESUMEN
Los problemas de comportamiento infantil disruptivo son frecuentes para muchos padres y pueden estar asociados con graves conductas delictivas o agresivas/violentas en la adolescencia o en la edad adulta. Las intervenciones con los padres que tratan este tipo de problemas de comportamiento disruptivo han ganado aceptación. Unos de estos programas de intervención con los padres es la Terapia de Interacción Padres-Hijos (PCIT). El PCIT es un programa, basado en las teorías del apego y del aprendizaje social, diseñado para niños y niñas de entre 2 y 7 años de edad que presenten problemas de conducta disruptiva o externalizados, y que tiene una duración de entre 14 y 20 semanas. En este artículo se presentará una breve revisión de la historia del PCIT, una descripción de sus componentes básicos, y una visión general de los avances recientes que subrayan las posibilidades del PCIT para mejorar las relaciones padres-hijos en familias maltratantes, para tratar a niños y niñas víctimas de situaciones traumáticas y para mejorar la resiliencia en niños y niñas de corta edad. En relación con los tres objetivos básicos del PCIT (es decir, reducción de los problemas de conducta, mejora de las habilidades parentales y mejora de la calidad de las relaciones entre padres e hijos), hay una abundancia de investigaciones que demuestran robustos efectos del tratamiento y, por tanto, su validez para ser aplicado de manera generalizada. La investigación más reciente ha demostrado también el valor de PCIT en la reducción de síntomas traumáticos en niños y niñas de corta edad.
Palabras clave: Palabras clave: habilidades parentales, problemas de conducta, Terapia de Interacción Padres-Hijos, tratamiento.
Disruptive child behavior problems -including aggression, oppositional behaviors, and noncompliance- are the most common problems for which parents seek professional intervention (Kazdin, Bass, Ayers, & Rodgers, 1990). Although discrete instances of oppositional or defiant behaviors are fairly common throughout childhood, a stable pattern of disruptive behavior is strongly associated with serious delinquent behaviors and aggressive/violent behaviors in adolescence and adulthood (Broidy et al., 2003; Fergusson, Horwood, & Lynskey, 1994; Tolan & Gorman-Smith 1998). Throughout the history of delivery of child mental health services, 'child-only' approaches (e.g., play therapy, individual therapy) have been the primary interventions to reduce these types of behavioral problems. However, during the last few decades there has been a strong movement toward treating these types of disruptive child behavior problems through interventions that incorporate parents or are focused on enhancing parenting skills (Bourke & Nielsen, 1995; Graziano & Diament, 1992). This movement toward using parenting interventions to address disruptive child behavior problems has gained widespread acceptance (Kazdin & Weisz, 2003). Further, this approach is also supported by a recent meta-analysis of parenting interventions (Kaminski, Valle, Filene, & Boyle, 2008) that found interventions with the largest effects focused on increasing positive parent-child interactions and emotional communication skills, teaching parents to use time-out and the importance of parenting consistency, and requiring parents to practice new skills with their children during parent training session. One of these parenting interventions, Parent-Child Interaction Therapy (PCIT; Eyberg & Robinson, 1983) incorporates all three of these elements.
In the following pages, this chapter will provide a brief review of the history of PCIT, a description of the basic components of PCIT, and an overview of recent developments that highlight the promise of PCIT with maltreating parent-child relationships, traumatized children, and in developing resilience in young children.
Initially Sheila Eyberg emphasized PCIT's consistency with principles of operant conditioning, with stated objectives of decreasing child disruptive behavior and improving parenting skills. However, Eyberg (2004) has also noted the influences of early pioneers in play therapy in the development of PCIT: Virginia Axline (1947) and Bernard Guerney (1964). In her description of the origin of PCIT, Eyberg (2004) expressed her support of the play therapy goals and techniques proposed by the Axline and Guerney therapeutic approaches of promoting warmth and acceptance. Eyberg (2004) added that Diana Baumrind's work (1966; 1967) encouraged her to conceptualize healthy parenting as including clear communication and firm limit-setting, reflected in authoritative parenting. As a result, Eyberg developed PCIT with the objective of increasing positive parent and child relationship skills to achieve the underlying objective of promoting the foundational elements of a healthy parent-child relationship. The genius of Eyberg's innovation was to expand upon Hanf's (1968) ideas of in vivo parenting and use the structure of a 'coaching' paradigm to teach parents the skills employed by child therapists (e.g., nurturing, warmth, and responsiveness, enhancing the relationship) and the skills needed for managing children's difficult behavior.
]]> What is Parent-Child Interaction Therapy?Parent-Child Interaction Therapy (PCIT) is a 14- to 20-week, manualized intervention founded on social learning and attachment theories. PCIT is designed for children between 2 and 7 years of age with disruptive, or externalizing, behavior problems (Eyberg & Robinson, 1983). The underlying model of change is similar to that of other parent-training programs. These programs promote the idea that through positive parenting and behavior modification skills, the parents themselves become the agent of change in reducing their child's behavior problems. However, unlike other parenting-focused interventions, PCIT incorporates both parent and child in the treatment sessions and uses live, individualized therapist coaching for an idiographic approach to changing the dysfunctional parent-child relationship.
PCIT is conducted in two phases. The first phase focuses on enhancing the parent-child relationship (Child-Directed Interaction; CDI), and the second on improving child compliance (Parent-Directed Interaction; PDI). Both phases of treatment begin with an hour of didactic training, followed by sessions in which the therapist coaches the parent during play with the child. From an observation room behind a two-way mirror, via a 'bug-in-the-ear' receiver that the parent wears, the therapist provides the parent with feedback on their use of the skills. Parents are taught and practice specific skills of communication and behavior management with their children. In addition to practicing these skills during clinic sessions, parents are asked to practice with their children at home for 5 minutes every day.
In CDI (typically 7-10 sessions), parents are coached to follow their children's lead in play by describing their activities, reflecting their appropriate verbalizations, and praising their positive behavior. By the end of CDI, parents generally have shifted from rarely noticing their children's positive behavior to more consistently attending to or praising appropriate behavior. When caregivers master the skills taught in CDI by demonstrating that they can give behavior descriptions (e.g., "You are building a tall tower"), reflections (i.e., repeating back or paraphrasing the child's words), and praises (e.g., "Thank you for playing so gently with these toys"), with few instances of asking a question, giving a command, and eliminate criticizing their child in a 5-minute assessment, they move to the second phase of treatment. An example of CDI coaching would include:
(Parent and child are playing with Legos; the therapist is watching from an adjacent observation room and talking to the parent through the 'bug-in-the-ear' system)
Therapist: Describe to Robert what he is doing with
his hands.Parent: You put all of the blue Legos on the table.
]]> Therapist: That was a great behavioral description! Child: Yes, I'm going to make a big blue tower.
[Behavioral Description]Parent: You're going to make a big blue tower
[Reflection]Coach: You got it! That was a perfect reflection of
what Robert said. He knows you are paying attention to what he is doing. When
you give him praise and attention for his
good behavior, he will do more of that
behavior.Parent: I like it when you play nicely with the toys. [Labeled Praise]
Therapist: Great labeled praise.
]]> Child: And I'm going to make a red tower too!
And a yellow one!
In PDI (typically 7-10 sessions) therapists train parents to give only essential commands, to make them clear and direct, maximizing chances for compliance. Parents participating in PCIT traditionally learn a specific method of using time-out for dealing with non-compliance. Parents also may be taught "hands-off" strategies (e.g., removal of privileges) if indicated. These strategies are designed to provide caregivers tools for managing their children's behavior while helping them to avoid using physical power, focusing instead on using positive incentives and promoting children's emotional regulation. Mastery of behavior management skills during PDI is achieved when therapists observe that caregivers are able to use the behavior management strategies they were taught without being coached and when parents report that these strategies are effective. By the end of PDI, the process of giving commands and obtaining compliance are predictable and safe for parents and children. An example of PDI coaching would include:
(Parent and child are playing with Legos; the therapist is watching from an adjacent observation room and talking to the parent through the 'bug-in-the-ear' system)
Therapist: It is now time to clean up the toys. Tell
Robert to put the Legos back in the box.Parent: Robert, it's time to clean up. Please put the
Legos back in the box. [Direct Command]Therapist: That was a wonderful Direct Command. ]]>
Now Robert knows exactly what he is supposed to do.Child: (Robert starts to put a couple of Legos in the
box)Parent: Great job of putting the Legos back in the box!
[Labeled Praise]Therapist: That was a great praise for putting the
Legos away. The will help Robert want to
clean-up more in the future.
PCIT with Oppositional, Defiant Children
There have been numerous studies demonstrating the efficacy of PCIT for reducing child behavior problems (Eisenstadt, Eyberg, McNeil, Newcomb, & Funderburk, 1993; Eyberg, 1988; Eyberg & Robinson, 1982). Positive effects have been maintained for up to six years post-treatment (Hood & Eyberg, 2003). In addition, treatment effects have been shown to generalize to the home (Boggs, Eyberg, & Reynolds, 1990), school settings (McNeil, Eyberg, Eisenstadt, Newcomb, & Funderburk, 1991), and to untreated siblings (Eyberg & Robinson, 1982). In addition, there is research indicating that PCIT yields positive treatment outcomes with different types of cultural and language groups, including Spanish-speaking families (McCabe, Yeh, Garland, Lau, & Chavez, 2005), Chinese-speaking families (Leung, Tsang, Heunh, & Yiu, 1999), and African-American families (Fernandez, Butler, & Eyberg, 2011).
]]> PCIT with Abusive FamiliesWith the numerous studies demonstrating the value of PCIT with oppositional and defiant children, Urquiza and McNeil (1996) argued that some (if not many) of the children involved in PCIT studies were also victims of physical abuse and/or exposed to domestic violence and promoted the use of PCIT with maltreatment and exposure to domestic violence. There are many reasons to expect that PCIT would be a beneficial treatment for maltreating families. Effective treatments for these families should incorporate both the parent and the child because the behaviors of each contribute to the maladaptive responses of each, feeding a continuing cycle of hostility and coercion. The treatment should also provide a means to directly decrease negative affect and coercive control, while promoting (i.e., teaching, coaching) greater positive affect and discipline strategies. PCIT satisfies both of these conditions; and it has been demonstrated to be a highly effective treatment. It is for these reasons that in the last decade there has been a pattern of research findings showing positive outcomes with physically abusive parent-child dyads (Timmer, Urquiza, Zebell, & McGrath, 2005), and other types of maltreated children, including abused children, children exposed to domestic violence, and children with their foster parents (Borrego, Timmer, Urquiza, & Follette, 2004; Chaffin et al., 2004; Timmer, Borrego, & Urquiza, 2002; Timmer, Urquiza, & Zebell, 2006; Timmer, Ware, Zebell, & Urquiza, 2010). In summary, while PCIT was initially developed as an intervention specifically for children with disruptive behavioral problems, there is currently ample research that identifies PCIT as an effective evidence-based parenting program for high-risk and abusive families.
PCIT and Child Trauma
Urquiza and colleagues (Mannarino, Lieberman, Urquiza, & Cohen, 2010) have reported several interventions that are effective at reducing trauma symptoms with young children- including PCIT. Research conducted by Urquiza & Timmer (2008) found that young children with trauma symptoms and disruptive behavior problems had a significant reduction in both types of problems after receiving traditional PCIT treatment. However, this research raises questions regarding why child trauma symptoms would decrease as a result of involvement in a parenting program. To better understand why young traumatized children improve as a result of involvement in PCIT, it is important to examine developmental characteristics associated with children's expression of trauma, parent-child relationships, and resiliency.
Younger and older children respond differently to trauma, with younger children appearing to be more responsive to the stability (or lack of stability) of parental functioning and older children less likely to be adversely affected by parent instability (Scheeringa & Zeanah, 2001). In particular, younger children (i.e., toddlers, preschool-age, elementary-age children) are highly responsive to parent cues of affective stability, instability, and distress related to adverse family events (e.g., interpersonal violence), often because their means of coping is still co-regulated by the parent (Chu & Lieberman, 2010; Fogel, Garvey, Hsu, & West-Stroming, 2006). In contrast, older children (i.e., schoolage, adolescents) tend to rely more on their own coping skills and cognitions, may be more independent, developing other sources of support, such as peers or kin (Werner, 1995). Because of these factors, approaches to treatment including both the parent and child are likely to be more effective with younger than older children (Runyon, Deblinger, Ryan, & Thakkar-Kolar, 2004).
Many common child traumas (e.g., child physical abuse, child sexual abuse, exposure to domestic violence) have a range of common and disturbing responses. Children who experience traumatic events exhibit symptoms consistent with Posttraumatic Stress Disorder (American Psychiatric Association, 2000), including nightmares, affective dysregulation, intrusive imagery, and intense distress related to internal or external cues associated with the traumatic event (Copeland, Keeler, Angold, & Costello, 2007). However, it is more difficult to detect the effects of trauma in young children, because they do not recognize or cannot articulate the connection between the traumatic event and how they feel and behave because of limitations in their expressive language ability, social cognition, and cognitive functioning.
One characteristic of many violent families that contributes to children's disruptive behavior problems is the absence of positive, warm, and nurturing parenting (Fantuzzo, DePaola, Lambert, Martino, Anderson, & Sutton, 1991). When traumatized children live in families with chaotic lifestyles, in which consistent and positive parent-child relationships are infrequent or nearly nonexistent, their behavioral problems may be less related to their trauma than the overall chaotic and dysfunctional lifestyle in which they are being raised. The population of children who have disruptive behavioral problems resulting from inconsistent and poor parenting is the group for whom some type of intensive parenting intervention may be most effective (Kaminski et al., 2008), although this type of intervention may not directly address the cognitions and affect related to the child's trauma.
Improved child relationship security and stability with their primary caregiver. One of the avenues to recovery from child trauma involves eliciting support from important caregivers. That is, supportive parenting is associated with positive child outcomes in many domains (Greenberg, 1999; Kim et al., 2003), especially when a child is required to deal with some type of adverse experience. Therefore, it is essential to sustain a positive parent-child relationship and parental support in order to optimize the child's ability to deal with any adverse or traumatic experience. The combination of parental stress associated with child trauma and problematic child symptoms can erode a parent's ability to be supportive, warm, and understanding. By teaching parents child-centered play skills, warmth and positive affiliation increase, thereby strengthening the parent-child relationship.
Decreasing Child Behavioral Problems May Increase Parental Capacities. For relationship-based interventions to be effective, the caregiver must be able to participate and implement the skills learned or ideas discussed during therapy sessions. When primary caregivers have other sources of stress and trying to cope with the effects of their own traumatic experiences, these problems contribute to children's mental health problems, dampening parents' warmth and sensitivity and interfere with effective parenting (Lovejoy, Graczyk, O'Hare, & Neuman, 2000), and disrupt treatment effectiveness (Stevens, Ammerman, Putnam, & Van Ginkel, 2002). Symptoms of post-traumatic stress, such as depression, fatigue, dissociation and poor concentration can interfere with the acquisition of parenting skills (Reyno & McGrath, 2006). Furthermore, parental depression increases the likelihood of early treatment termination (Kazdin, 2000), completely removing the children from the possibility of being helped. However, research has shown that if traumatized parents can overcome their tendencies to drop out of treatment and are motivated to participate in a relationship-based treatment their own psychological symptoms can be relieved (Timmer et al., 2011). In PCIT, parents are taught how to cope with the emotions that often accompany their children's disruptive behavior by using anxiety reduction skills such as deep-breathing and counting silently when frustrated. They are coached to observe, notice, and react to their children's positive behavior. They are coached to show warmth, enthusiasm, and enjoyment in their interactions with their children. When traumatized parents repeatedly perform these positive and adaptive behaviors throughout the course of PCIT, it is thought that these adaptive responses may begin to generalize, or "spill over" into other parts of their lives, replacing maladaptive responses (Timmer et al., 2011).
]]> PCIT Case Study
The family in treatment was a 27-year-old mother and her 4 year-old son, "A." The mother was married, but had been separated from her husband, the boy's biological father, for approximately two years. The family was referred to treatment by their Child Protective Services (CPS) social worker because of the child's extremely aggressive verbal and physical behavior towards his mother, his temper tantrums, destructiveness, and impulsive behavior. The referral also noted that the child displayed separation anxiety, crying uncontrollably whenever the mother left him. The therapist saw the mother and A for 34 PCIT sessions in the clinic: 2 assessment sessions, 2 teaching sessions, and 30 coaching sessions (these were more than the typical 14-20 sessions). In addition to these inclinic PCIT sessions, the mother intermittently received her own individual therapy. Toward the end of treatment, the family received adjunct, in-home support services (4 sessions) to help the mother generalize her PCIT skills to the home setting.
Child History. "A" lived with his mother and 6 year- old brother, visiting with his father on weekends at the home of his paternal grandmother. A's mother and father had a long history of domestic violence; the most recent incident of extreme violence took place approximately a year before their referral to PCIT. The mother had arranged to pick the children up after the father's visitation in the parking lot of a grocery store. While the mother was trying to get A out of his car seat, she and the father's girlfriend began exchanging insults, which escalated into scratching and hair pulling. The father, who had been putting the brother into the mother's vehicle, pulled the mother out of his car and held her while the girlfriend physically assaulted the mother, then pushed her back into his car and continued to kick and punch her in front of A. Bystanders called the police and emergency medical services.
In the initial clinical interview, the mother reported that A had been aggressive, destructive, defiant, and impulsive "for years." She believed that the child's behavioral problems resulted from his witnessing domestic violence. However, it should be noted that in addition to being exposed to violence between his parents, the mother had a history of severe depression. It is suspected that the mother was experiencing depressive symptoms throughout A's life. At the time she brought A for PCIT services, she was not receiving any counseling, nor was she taking medication. The mother denied any drug or alcohol abuse.
PCIT Assessment and Treatment Procedures
PCIT is an assessment driven treatment. Prior to treatment and upon graduation, parents complete a battery of standardized assessments including the following measures: Child Behavior Checklist (CBCL, 1 ½- 5 yrs; Achenbach & Rescorla, 2000) and the Eyberg Child Behavior Inventory (ECBI; Eyberg & Pincus, 1999), two standardized measures of the severity of children's behavior problems; the Trauma Symptom Checklist for Young Children (TSCYC; Briere et al., 2001), a measure of the severity of children's trauma symptoms; the Brief Symptom Inventory (BSI; Derogatis, 1993), a self-report measure of the parent's psychological symptoms; and the short form of the Parenting Stress Index (PSI; Abidin, 1995), a measure of the severity of three sources of stress in the parent role: parental distress, dysfunction in the parent-child relationship, and difficult child behavior.
In addition, the therapist conducts a behavioral assessment pre- and post-treatment, observing the dyad as they play together in three semi-structured activities, using the Dyadic Parent-Child Coding System-III (DPICS-III; Eyberg, Nelson, Duke, & Boggs, 2005), a micro-analytic coding system, designed by Eyberg and her colleagues (2005) to categorize parent verbalizations in parent-child interactions. The three play situations vary in the amount of control the parent is asked to use. In the first situation (Child-Directed Interaction), the parent is asked to follow the child's lead in play. Parents are told to let the child pick an activity and to play along. In the Parent- Directed Interaction, parents are instructed to pick an activity and have the child play with the parent according to the parent's rules. In the third, and final situation, the parent is directed to have the child to 'clean up' without the parent's assistance. For research purposes, we also used a global assessment of the quality of the caregiver-child relationship, the Emotional Availability Scales (EAS, 3rd Ed.; Biringen, 2000), to illustrate the quality of change in the parent-child relationship from pre- to post-treatment. The EAS consists of four scales measuring aspects of the parent's behavior toward the child and two scales measuring qualities of the child's behavior toward the parent. In addition to assessing the parent and child behavior in the DPICS sessions, the therapist uses the first 5 minutes of each weekly treatment session to observe the parent-child interactions in child-directed play. The therapist remains silent during this time, coding the parent-child verbalizations.
Course of Treatment in PCIT
The mother agreed with the therapist's suggestion that PCIT would fit their needs, and weekly sessions were scheduled. After the therapist conducted a CDI teaching session, teaching the mother about the skills she would need and what to expect from treatment, coaching sessions began. At the beginning of each session, the therapist talked briefly with the mother, asking how A had behaved since she had last seen her and how the mother was doing. During the third session, the mother complained about feeling stressed by financial difficulties and depressed by breaking up with her boyfriend. Her children were also more difficult to manage. The therapist referred mother for her own counseling, suggesting that if she had some support it might be easier for her to make progress in PCIT. Two weeks later, the mother reported that her depressive symptoms were worsening, but that she had an appointment with her physician in two weeks to obtain anti-depressant medication. According to the children's social worker, a few days later (just before the 6th coaching session), the mother phoned the social worker and told her that she was too depressed and overwhelmed to take care of the children. The social worker decided to remove the children from the mother's custody temporarily.
A little more than a month later, A and his mother began coming in to PCIT again. At this time the mother had two days of visitation a week and had been taking anti-depressants for about a month, and reported some decrease in depressive symptoms. A and his mother made unsteady progress over the next month. At times, she seemed focused and able to use her PCIT skills, reporting better and calmer behavior in her son. At other times, she reported that A kicked and hit her. At these times she also seemed disconnected from treatment and the child unresponsive to her attempts to perform the skills. The therapist arranged for the mother to receive weekly adjunct services to the mother for problems related to depression and trauma. Two weeks after beginning adjunct individual treatment, the mother regained full custody of both boys. Two weeks after this, on the 15th coaching session (3 months after returning to PCIT), A and his mother moved on to the second phase of treatment: the mother showed mastery of play therapy skills and her son was more consistently responsive to her.
]]> Altogether, the dyad received 14 PDI coaching sessions before the therapist was confident that the mother could manage her son's behavior, and that her son's behavior problems were sufficiently diminished. During this time, the mother received 15 of her own weekly individual services. At PDI session number 12, the family began to receive in-home services to help the mother generalize her skills to the home setting.Description of Mother's Treatment
Knowing that the mother had a long history of domestic violence and a previous history of abuse and foster care, the therapist anticipated that he would be doing trauma-related therapy with the mother, uncovering triggers that made it difficult for her to implement the skills she was learning in PCIT. After initial clinical interviews, it was the therapist's opinion that the mother's depressive symptoms, dependency needs, helplessness, and low self-efficacy were the greatest barriers to progress in PCIT. Consequently, he implemented two-pronged approach for treatment: a cognitive-behavioral approach to help promote healthy cognitions and discourage depressive ones, and mindfulness training to help her control impulsivity and solve problems. Sessions were mostly devoted to disentangling problems she was having with her ex-husband and his girlfriend, the schools, the custody dispute, and how she could use the skills she was learning in PCIT better.
Standardized Measures
Child behavior problems. Table 1 shows the scores of measures completed by A's mother pre-treatment, the 7th session (ECBI only) and post-treatment. The mother's ratings of her son on the ECBI and the CBCL show that the number and frequency of his behavior problems are in the clinical range at pre-treatment. In particular, the mother noted problems with A's emotional reactivity (e.g., sulky, whiny, moody, upset by new things), anxiety/depression (e.g., clingy, nervous, fearful), aggressiveness (e.g., angry, destructive, temper tantrums), resulting in elevated scores on the internalizing and externalizing behavior problems scales. By the 7th session, the intensity of disruptive behavior problems reported on the ECBI had dropped more than one standard deviation and was just out of the clinical range. By the end of treatment, the intensity of problems had dropped another 1.5 standard deviations. Similar decreases in the severity of A's behavior problems were also reported on the CBCL. In contrast to the mother's report of A's behaviors, the change in the degree to which A's problems were still a problem for her decreased more slowly and less dramatically. We observed no change in the numbers of behaviors considered as problems for her from pre-treatment to the 7th coaching session (26 out of 36 behaviors), but a change in more than one standard deviation from pre- to post-treatment, although the post-treatment score remained in the clinical range.
Child trauma symptoms. A's scores on the TSCYC pre-treatment (per mother's report) show symptoms of post-traumatic stress in the clinical range. In particular, the mother reported that A was bothered and still frightened by his bad memories. Additionally, A's mother reported that he exhibited clinical levels of anxiety, depressive symptoms, anger and aggression, and sexual concerns. By post-treatment, T-scores had dropped at least two standard deviations, and all of the TSCYC scales were out of the clinical range.
Parent functioning. In addition to measures of her child's functioning, A's mother completed the BSI, measuring her own psychological symptoms, and the short form of the PSI, a measure of the severity stress in the parent role. As can be seen in Table 1, at pretreatment her symptom profile on the BSI showed general symptomatic distress in the clinical range, endorsing clinical levels of symptoms on the depression, anxiety, hostility, and phobic anxiety scales. Post-treatment, scores on these scales reflecting self-reported psychological symptoms decreased at least 1.5 standard deviations and were within normal limits. The mother's reporting on the PSI pre-treatment suggests that she was experiencing considerable stress in the parent role. Her distress related to feelings of incompetence, of being restricted in other parts of her life because of being a parent, depression, and conflict with her spouse. She reported significant stress in her relationship with A, noting that he would "do things that bother her just to be mean." She also reported clinical levels of stress resulting from parenting a child with difficult behaviors. As Table 1 shows, the mother's parental stress decreased from pre- to post-treatment.
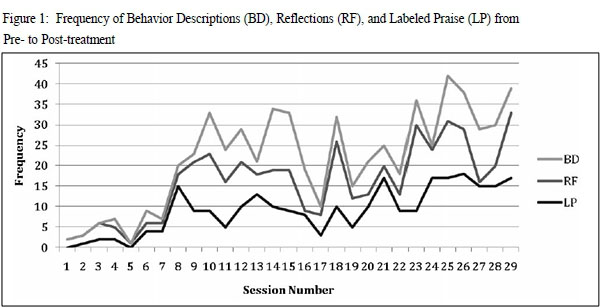
Parent verbalizations. Figure 1 and Figure 2 show the results of coding the mother for the first 5 minutes of the observational assessment (child-led play) as well as the 5-minute observations at the beginning of each treatment session, using the DPICS coding system. In the first phase of treatment (CDI), the goal is to increase parents' praise, reflections, and behavioral descriptions and reducing commands, questions, and negative talk. The variability of the mother's performance is notable in CDI. During the first five sessions, when A's mother is suffering most from depression, she shows little change in the way she interacts with her son. After a brief hiatus, she returns to PCIT and slowly improves until she meets "CDI mastery" (i.e.,giving 10 praises, 10 reflections, and 10 behavior descriptions in the 5 minute observation, and gives no more than 3 commands, questions, or negative verbalizations). Once the parent meets CDI mastery, instructions during the 5 minutes change slightly in order to give the parent a chance to practice giving effective commands. During PDI the mother was instructed to give four commands during the five minutes of play, but was still expected to use her CDI skills (i.e., PRIDE skills). The first four months of PDI when the dyad inconsistently attended PCIT, the mother's performance in the 5-minute observational assessment was also inconsistent to poor. As A and his mother attended more regularly, her performance improved markedly. While the mother never gave consistently effective commands during the observational assessment in the latter part of PDI, the child was compliant with her commands.
]]>
Emotional Availability. Table 2 shows the pre- and post-treatment Emotional Availability scale scores for A and his mother. When they came into treatment, A's mother was mostly quiet and withdrawn. When she participated in play, her voice was well-modulated (i.e., not flat or depressed), but she primarily varied between trying a little too hard to be cheerful and long periods of silence. In parent-led play and clean up, she appeared afraid to give her son a command to change the activity, asking "Okay, honey? Okay, hostility, so received optimal scores on that scale in all three activities.
As for the child, A seemed only marginally interested in playing with his mother in the pre-treatment assessment, making little eye-contact, and not really responding to her overtures or suggestions, though he asked her for help at one point in CDI. For this reason he received non-optimal scores in responsiveness in all three activities, and received an optimal score in Involvement in CDI, but non-optimal scores in PDI and Clean Up. Post-treatment, A involved his mother in his play and responded to her statements and questions. However, he wouldn't let her look while he "made a meal" in PDI and was a little sassy, asking her "how many times do I have to ask you (not to look)?" For this behavior, A received optimal scores in Responsiveness and Involvement in CDI, and nonoptimal scores in PDI and Clean Up.
honey?" multiple times; or clean up, when, checking with the therapist, she made it clear to the child that it was not her choice to clean up. The mother also had a difficult time setting limits. After cleaning up, the child told the mother to give him her keys and tried to put holes in the booster seat. She merely stared into space, not responding to this inappropriate behavior. For these reasons, the mother scored in the non-optimal range of sensitivity and structuring. She showed no hostility and was not intrusive, so she scored in the optimal range on these scales. Post-treatment, the mother appeared significantly more engaged in the child-led play, describing and praising the child's positive behaviors. She stayed involved in play, but primarily followed A's lead, not really making any contributions of her own. When she needed to take more control of the interaction, in PDI and Clean Up, she used many PRIDE skills, and the child complied with her directions. At one point after A had cleaned up, he nattered her about a surprise she had promised, being a little sassy. She wheedled a little in response, quietly, then changed the subject and disengaged a bit. As a result, her Sensitivity, Intrusiveness, and Structuring scores were in the optimal range in CDI, but declined in PDI and Clean Up. She showed no
Summary. We argue that the parenting skills taught in PCIT supported the mother's confidence in taking a responsive and authoritative role with her son. In addition to giving her an effective way to communicate with A, PCIT therapists also coach related skills like positively attending to A's desirable behaviors, consistently and calmly following through with negative consequences, planning ahead, considering his limitations, communicating clearly and directly, and, practicing and eventually mastering these skills helped A's mother to build self-efficacy as a parent, which may spill over into other life roles.
]]> Discussion
After three decades of efficacy and effectiveness research, there is no question that PCIT is a highly effective and well-supported intervention. In addressing the three basic treatment objectives for PCIT (i.e., reduction in child behavior problems, improving parenting skills, enhancing the quality of parent-child relationships), there is an abundance of research demonstrating very strong treatment effects and therefore, its value to the field (Eyberg & Bussing, 2010).
Why is PCIT Effective?
Although grounded in behavioral theory, social learning theory, and family systems theory, there are also continuing questions concerning exactly what makes PCIT so effective. The question of, 'Why is PCIT effective?' is not superfluous. As described by behavioral theories, we know that consistently reinforcing desired behaviors (e.g., therapist praise of positive parenting behaviors, parent praise of child compliance) increases the frequency of this behavior. Additionally, social learning theory explains why concepts such as modeling (e.g., parents demonstrating calm, assertive, positive behaviors in interactions with their child models these same behaviors to their child) can be an effective strategy within a PCIT session. Finally, family systems theory explains why making changes in a parent's behavior (e.g., increasing positive behaviors, decreasing negative behaviors) can influence their child's behavior (child responses to positive parenting behaviors results in a decrease in oppositional behavior). However, there are additional processes that are likely to change as a result of successful involvement in PCIT- especially with children exposed to adverse or traumatic events.
PCIT and Child Trauma
Much of the research and treatment on traumatized children has focused solely on the traumatized child's trauma symptoms, with much less attention to the disruptive behavior problems that are often present with these young children. As is evident in this case, children who experience significant trauma often have both trauma symptoms and disruptive behavioral problems. In examining the traumatized child through a broad scope of functioning and social contexts, it becomes apparent that the parent-child relationship may be both a protective factor and a risk factor, which can assist and hinder the child in their recovery from the traumatic event. For young children, this parent- child protective/risk conundrum suggests that any intervention for the child needs to incorporate both the parent in the treatment process and address the parent's capacity to provide a warm, positive, and protective relationship. In the same way that negative, coercive parent-child interactions can lead to a multitude of adverse outcomes, warm, nurturing, and supportive parent-child interactions can promote resilience. The focus of PCIT is to decrease negative interactions and increase positive interactions, increasing the parent- child dyad's capacity to support resilience in both members of the dyad. We argue that by supporting and building strength in the parent-child dyad, we help leverage ongoing mental health and well being in traumatized young children. Recent literature has reported that a positive parent-child relationship is an important protective factor, promoting resilience in distressed and traumatized children (Ellis, Saxe, & Twiss, 2011). Unfortunately, for children who exhibited aggressive and defiant behavior, their ability to sustain a positive relationship with their parents are severely compromised, thus hindering their development of resilience. The stable pattern of positive parent-child interactions sets in place a series of positive, constructive capacities for both parent and child. One asset of PCIT is that it is an intervention that promotes 'natural' resilience- developing processes by strengthening positive parent- child relationships (Ellis, Saxe, & Twiss, 2011).
We believe the potential gain of strengthening the parent-child relationship is great, and that this case illustrates the complexity of people's lives and their ongoing vulnerability to risk. At several points in the course of treatment, this family could have terminated services. The mother was depressed and not really making much positive change; she was having trouble getting out of bed and attending her child's therapy appointment. At one point, she lost custody of her children. In the face of seemingly overwhelming obstacles, the mother felt helped and supported, retaining her belief that the services make a difference for her future. By recognizing the mother's contributions and hindrance to her son's mental health, interventions could be put in place to support treatment of her son's mental health problems. All things taken together, we hope this case illustrates the way in which supporting and building a secure and nurturing parent-child relationship is both the mechanism by which some trauma symptoms can be treated and the source of a resilience- developing parent-child relationship.
References
Abidin, R. R. (1995). Parenting Stress Index: Professional manual. Odessa, FL: Psychological Assessment Resources. [ Links ]
Achenbach, T. M., & Rescorla, L. (2000). Manual for the ASEBA Preschool Forms & Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth & Families. [ Links ]
American Psychiatric Association (2000). Diagnostic and statistical manual of mental disorders, IVth Edition - Text Revision. Arlington, VA: American Psychiatric Association. [ Links ]
Axline, V. (1947). Play Therapy. London: Ballantine Books. [ Links ] Baumrind, D. (1966). Effects of authoritative parental control on child behavior. Child Development, 37, 887-907. [ Links ]
Baumrind, D. (1967). Child care practices anteceding three patterns of preschool behavior. Genetic Psychology Monographs, 75, 43-88. [ Links ]
]]>Biringen, Z. (2000). Emotional availability: Conceptualization and research findings. American Journal of Orthopsychiatry 70, 104-111. [ Links ]
Boggs, S. R., Eyberg, S. M., & Reynolds, L. (1990). Concurrent validity of the Eyberg Child Behavior Inventory. Journal of Clinical Child Psychology, 19, 75-78. [ Links ]
Borrego, Jr., J., Timmer, S. G., Urquiza, A. J., & Follette, W. C. (2004). Physically abusive mothers' responses following episodes of child noncompliance and compliance. Journal of Consulting and Clinical Psychology, 72, 897- 903. [ Links ]
Bourke, M. L., & Nielsen, B. A. (1995). Parent training: Getting the most effective help for the most children. Journal of Psychological Practice, 1, 142-152. [ Links ]
Briere, J., Johnson, K., Bissada, A., Damon, L., Crouch, J., Gil, E., … Ernst, V. (2001). The Trauma Symptom Checklist for Young Children (TSCYC): Reliability and association with abuse exposure in a multi-site study. Child Abuse & Neglect, 25, 1001-1014. [ Links ]
]]>Broidy, L. M., Nagin, D. S., Tremblay, R. E., Bates, J. E., Brame, B., Dodge, K. A., ... Vitaro, F. (2003). Developmental trajectories of childhood disruptive behaviors and adolescent delinquency: A six-site, cross-national study. Developmental Psychology, 39, 222-245. [ Links ]
Chaffin, M., Silovsky, J. F., Funderburk, B., Valle, L., Brestan, E. V., Balachova, T., ... Bonner, B. L. (2004). Parent-Child Interaction Therapy with physically abusive parents: Efficacy for reducing future abuse reports. Journal of Consulting and Clinical Psychology, 72, 500- 510. [ Links ]
Chu, A. T., & Lieberman, A. (2010). Clinical implications of traumatic stress from birth to age five. Annual Review of Clinical Psychology, 6, 469-494. [ Links ]
Copeland, W. E., Keeler, G., Angold, A., & Costello, E. J. (2007). Traumatic events and posttraumatic stress in childhood. Archives of General Psychiatry, 64, 577-584. [ Links ]
Derogatis, L. R. (1993). BSI Brief Symptom Inventory. Administration, Scoring, and Procedures Manual (4th ed.). Minneapolis, MN: National Computer Systems. [ Links ]
]]>Eisenstadt, T. H., Eyberg, S., McNeil, C. B., Newcomb, K., & Funderburk, B. (1993). Parent-child interaction therapy with behavior problem children: Relative effectiveness of two stages and overall treatment outcome. Journal of Clinical Child Psychology, 22, 42-51. [ Links ]
Ellis, B. H., Saxe, G. N., & Twiss, J. (2011). Trauma Systems Therapy: Intervening in the interaction between the social environment and a child's emotional regulation. In V. Ardino (Ed.), Post-traumatic syndromes in childhood and adolescence. Wiley: Oxford. [ Links ]
Eyberg, S. M. (1988). Parent-child interaction therapy: Integration of traditional and behavioral concerns. Child & Family Behavior Therapy, 10, 33-46. [ Links ]
Eyberg, S. M. (2004). The PCIT story-part one: The conceptual foundation of PCIT. The Parent-Child Interaction Therapy Newsletter, 1, 1-2. [ Links ]
Eyberg, S., & Bussing, R. (2010). Parent-child interaction therapy. In M. Murrihy, A. Kidman, & T. Ollendick (Eds.), A Clinicians Handbook for the Assessment and Treatment of Conduct Problems in Youth (pp. 139-162). New York: Springer. [ Links ]
]]>Eyberg, S., Nelson, M., Duke, M., & Boggs, S. (2005). Manual for the Dyadic Parent-Child Interaction Coding System, (3rd ed.). Unpublished manuscript. [ Links ]
Eyberg, S., & Pincus, D. (1999). ECBI & SESBI-R: Eyberg Child Behavior Inventory and Sutter-Eyberg Student Behavior Inventory-Revised, Professional Manual. Odessa, FL: Psychological Assessment Resources. [ Links ]
Eyberg, S. M., & Robinson, E. (1982). Parent-child interaction training: Effects on family functioning. Journal of Clinical Child Psychology, 11, 130-137. [ Links ]
Eyberg, S., & Robinson, E. (1983). Conduct problem behavior: Standardization of a behavioral rating scale with adolescents. Journal of Clinical Child Psychology, 12, 347- 354. [ Links ]
Fantuzzo, J. W., DePaola, L. M., Lambert, L., Martino, T., Anderson, T., & Sutton, B. (1991). Effects of interparental violence on the psychological adjustment and competencies of young children. Journal of Consulting and Clinical Psychology, 59, 258-265. [ Links ]
]]>Fergusson, D. M., Horwood, L. J., & Lynskey, M. (1994). The childhoods of multiple problem adolescents: A 15- year longitudinal study. Journal of Child Psychology and Psychiatry, 35, 1123-1140. [ Links ]
Fernandez, M. A., Butler, A. M., & Eyberg, S. M. (2011). Treatment outcome for low socioeconomic status African American families in Parent-Child Interaction Therapy: A pilot study. Child and Family Behavior Therapy, 33(1), 32-48. [ Links ]
Fogel, A., Garvey, A., Hsu, H., & West-Stroming, D. (2006). Change processes in relationships: A relational-historical research approach. Cambridge, UK: Cambridge University Press. [ Links ]
Graziano, A. M., & Diament, D. M. (1992). Parent behavioral training: An examination of the paradigm. Behavior Modification, 16, 3-38. [ Links ]
Greenberg, M. T. (1999). Attachment and psychopathology in childhood. In J. Cassidy and P. R. Shaver (Eds.), Handbook of attachment: Theory, research, and clinical applications. New York: Guilford Press. [ Links ]
]]>Guerney, B., Jr. (1964). Filial therapy: Description and rationale. Journal of Consulting Psychology, 28, 304-310. [ Links ]
Hanf, C. (1968). A two-stage program for modifying maternal controlling during mother-child (M-C) interaction. Paper presented at the meeting of the Western Psychological Association, Vancouver, BC. [ Links ]
Hood, K., & Eyberg, S. (2003). Outcomes of Parent-child Interaction Therapy: Mothers' reports of maintenance three to six years after treatment. Journal of Clinical Child and Adolescent Psychology, 32, 412-429. [ Links ]
Kaminski, J. W., Valle, L. A., Filene, J. H., & Boyle, C. L. (2008). A meta-analytic review of components associated with parent training program effectiveness. Journal of Abnormal Psychology, 36, 567-589. [ Links ]
Kazdin, A. E. (2000). Perceived barriers to treatment participation and treatment acceptability among antisocial and their families. Journal of Child & Family Studies, 9, 157- 174. [ Links ]
]]>Kazdin, A. E., Bass, D., Ayers, W. A., & Rodgers, A. (1990). Empirical and clinical focus of child and adolescent psy-chotherapy research. Journal of Consulting and Clinical Psychology, 58, 729-740. [ Links ]
Kazdin, A. E., & Weisz, J. R. (2003). Evidence-based therapies for children and adolescents. New York, NY: Guilford. [ Links ]
Kim, I. J., Ge, X., Brody, G. H., Conger, R., Gibbons, F. X., & Simons, R. I. (2003). Parenting behaviors and the occurrence and co-occurrence of depressive symptoms and conduct problems among African American children. Depression, Marriage, & Families, 17, 571-583. [ Links ]
Leung, C., Tsang, S., Heung, K., & Yiu, I. (1999). Effectiveness of Parent Child Interaction Therapy (PCIT) in Hong Kong. Research on Social Work Practice, 19, 304-313. [ Links ]
Lovejoy, M. C., Graczyk, P. A., O'Hare, E., & Neuman, G. (2000). Maternal depression and parenting behavior: A meta-analytic review. Clinical Psychology Review, 20, 561-592. [ Links ]
]]>Mannarino, A., Lieberman, A., Urquiza, A., & Cohen, J. (2010, August). Evidence-based treatments for traumatized children. Paper presented at the 118th Annual Convention of the American Psychological Association, San Diego, CA. [ Links ]
McCabe, K. M., Yeh, M., Garland, A. F., Lau, A. S., & Chavez, G. (2005). The GANA program: A tailoring approach to adapting parent-child interaction therapy for Mexican Americans. Education and Treatment of Children, 28, 111-129. [ Links ]
McNeil, C., Eyberg, S., Eisenstadt, T., Newcomb, K., & Funderburk, B. (1991). Parent-child interaction therapy with behavior problem children: Generalization of treatment effects to the school setting. Journal of Clinical Child Psychology, 20, 140-151. [ Links ]
Reyno, S., & McGrath, P. (2006). Predictors of parent training efficacy for child externalizing behavior problems- a meta-analytic review. Journal of Child Psychology and Psychiatry, 47, 99-111. [ Links ]
Runyon, M. K., Deblinger, E., Ryan, E. E., & Thakkar-Kolar, R. (2004). An overview of child physical abuse: Developing an integrated parent-child cognitive-behavioral treatment approach. Trauma, Violence, & Abuse, 5, 65-85. [ Links ]
]]>Scheeringa, M. S., & Zeanah, C. (2001). A relational perspective of PTSD in early childhood. Journal of Traumatic Stress, 14, 799-815. [ Links ]
Stevens, J., Ammerman, R., Putnam, F., & Van Ginkel, J. (2002). Depression and trauma history in first-time mothers receiving home visitation. Journal of Community Psychology, 30, 551-564. [ Links ]
Timmer, S. G., Borrego, J., & Urquiza, A. J. (2002). Antecedents of coercive interactions in physically abusive mother-child dyads. Journal of Interpersonal Violence, 17, 836-853. [ Links ]
Timmer, S., Ho, L., Urquiza, A., Zebell, N., Fernandez y Garcia, E., & Boys, D. (2011). The effectiveness of Parent-Child Interaction Therapy with depressive mothers: The changing relationship as the agent of individual change. Child Psychiatry & Human Development, 42, 406-423. [ Links ]
Timmer, S. G., Urquiza, A. J., & Zebell, N. (2006). Challenging foster caregiver-maltreated child relationships: The effectiveness of Parent Child Interaction Therapy. Child & Youth Services Review, 28, 1-19. [ Links ]
]]>Timmer, S., Urquiza, A., Zebell, N., & McGrath, J. (2005). Parent-Child Interaction Therapy: Application to physically abusive and high-risk dyads. Child Abuse & Neglect, 29, 825-842. [ Links ]
Timmer, S., Ware, L., Zebell, N., & Urquiza, A. (2010). The effectiveness of Parent-Child Interaction Therapy for victims of interparental violence. Violence & Victims, 25, 486-503. [ Links ]
Tolan, P. H., & Gorman-Smith, D. (1998). Development of serious and violent offending careers. In R. Loeber, & D. P. Farrington (Eds.), Serious and violent juvenile offenders: Risk factors and successful interventions (pp. 68-85). Thousand Oaks, CA: Sage. [ Links ]
Urquiza, A. J., & Timmer, S. G. (2008, February). Trauma symptom reduction with delivery of Parent-Child Interaction Therapy services. Paper presented at the Twenty second Annual San Diego International Conference on Child and Family Maltreatment. San Diego, CA. [ Links ]
Urquiza, A. J., & McNeil, C. B. (1996). Parent-Child Interaction Therapy: an intensive dyadic intervention for physically abusive families. Child Maltreatment, 1, 134-144. [ Links ]
]]>Werner, E. (1995). Resilience in Development. Current Directions in Psychological Science 4(3), 81-85. [ Links ]
 Correspondence:
Correspondence:
Anthony J. Urquiz
CAARE Diagnostic & Treatment Center, Dept. of Pediatrics, UC Davis Children's Hospita
3300 Stockton Blvd., Sacramento, CA 95825, USA.
E-mail: anthony.urquiza@ucdmc.ucdavis.edu
PCIT Training Center web site: www.pcit.tv